
Abstract
Introduction
Venous thromboembolism (VTE), which includes deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common and potentially fatal complication during and following hospitalization for surgery. Pulmonary embolism accounts for 5% to 10% of deaths in hospitalized patients and is thus the most common preventable cause of in-hospital death.1,2 Without thromboprophylaxis during hospitalization, the incidence of DVT is approximately 10% to 40% among patients undergoing general surgery and 40% to 60% following major orthopedic surgery.1,3 Among over 7 million patients discharged from 944 US hospitals, postoperative VTE was the second most common surgical complication, the second most common cause of increased length of stay, and the third most common cause of excess mortality. 4 In addition to the acute complications, postoperative VTE is associated with long-term complications such as postthrombotic syndrome 5 and chronic thromboembolic pulmonary hypertension. 6
The mortality, acute and long-term complications, and additional resource utilization associated with postoperative VTE provide a strong impetus for the widespread implementation of thromboprophylaxis strategies. Hundreds of clinical trials of thromboprophylaxis have been conducted over the past 20 to 30 years, and these have provided strong evidence that primary prevention of VTE with the use of thromboprophylaxis in high-risk groups reduces VTE including fatal PE, 1 reduces overall hospital costs, 7 and is associated with a negligible risk of clinically important bleeding that is comparable to placebo or no prophylaxis.8,9 As a result, several evidence-based guidelines published over the past 15 to 20 years strongly support the widespread use of thromboprophylaxis in the surgical setting.1,10–12 Although implementation of thromboprophylaxis strategies has been shown to be cost-effective with an advantageous benefit-to-risk ratio, 13 rates of adherence to guideline recommendations remain low and range anywhere between 19% and 60% in surgical patients.14–18 For example, the recent large-scale Epidemiologic International Day for the Evaluation of Patients at risk of Venous Thrombosis in the Acute Hospital Care Setting (ENDORSE) study revealed that 51% of almost 70 000 patients in 368 hospitals across 32 countries were considered to be at increased risk of VTE but only 60% of surgical patients received thromboprophylaxis. 14 In another large retrospective cohort study of 10 744 patients older than 65 years, having undergone hip or knee replacement, only 2059 (19%) patients were prescribed thromboprophylaxis at discharge. 18
Few studies have evaluated clinical factors associated with nonadoption of and nonadherence to VTE prophylaxis guidelines. Using a large administrative hospital database, we sought to assess the rate of use and appropriate use of thromboprophylaxis as defined by the 7th Edition American College of Chest Physicians (ACCP) guidelines in a tertiary care center among patients undergoing general and orthopedic surgery deemed to be at risk for VTE, to identify clinical factors associated with nonuse and inappropriate use of thromboprophylaxis, and to estimate the risk of postoperative thrombosis according to thromboprophylaxis use.
Patients and Methods
We conducted a retrospective cohort study of all consecutive surgical admissions between January 1, 2006, and December 31, 2006, at the Centre Hospitalier Universitaire de Sherbrooke (CHUS), a large tertiary care center in Sherbrooke, Quebec, Canada. The CHUS is a 700-bed acute care hospital that services a population catchment area of about 200 000 persons. The following surgical admissions were excluded from the study population: (1) admissions with duration of stay of less than 24 hours as these are considered to be at “low risk” of postoperative thrombosis, (2) patients under 40 years of age undergoing minor surgeries (for example, nonlaparoscopic endoluminal surgeries, knee arthroscopy in the absence of more complicated surgery, elective abdominal, or thoracic surgery) for which thromboprophylaxis according to the 7th ACCP guidelines is not recommended, (3) admissions of patients less than 18 years of age since the ACCP surgical thromboprophylaxis recommendations apply to adults, and (4) admissions of patients with contraindications to anticoagulant treatment (recent symptomatic bleeding in critical area or organ, such as intracranial or intraspinal bleeding [defined by the International Classification of Diseases Ninth Revision, ICD-9, coding 430.0, 432.9, 432.1 within 30 days prior to surgery date], thrombocytopenia [ICD-9 code 287.3, 287.5, 289.84, 287.30, 287.4], or active peptic ulcer disease [ICD-9 code 531.0-531.3]). In doing so, our aim was to assess the adequacy of pharmacologic prophylaxis in patients without contraindications to anticoagulant use.
The Centre Informatisé de Recherche Évaluative en Soins et Systèmes de Santé (CIRESSS) database is a clinical data warehouse operational at the CHUS since 2002 and contains the following patient admission information: patient demographic information, admission and discharge date, primary and secondary discharge diagnoses coded by ICD-9, treatment and procedure codes (coded by the Canadian Classification of Diagnostic, Therapeutic and Surgical Procedures [CCP]), and in-hospital prescriptions (medication name, dosage, and time of medication administration). All coding is attributed by the medical records department and is updated every 24 hours. The CIRESSS is used primarily for quality assurance in the biochemistry department and by the emergency department to assess patient occupancy.
The following was obtained from CIRESSS for each patient admission included in our study population: (1) patient demographics (age, sex), (2) admission-related data (date of admission, date of discharge/transfer/death, duration of stay), (3) surgical data (type of surgery, date of surgery), (4) VTE-related risk factors (surgery within 90 days, major trauma within 90 days, malignancy (invasive or in situ, including cutaneous melanoma, but not other skin cancers [eg, squamous and basal cell carcinoma]) or cancer therapy within 90 days, previous VTE, pregnancy and the postpartum period, heart or respiratory failure within 90 days, inflammatory bowel disease, nephrotic syndrome, varicose veins, central venous catheterization, and inherited or acquired thrombophilia), (5) pharmacologic thromboprophylaxis (presence or absence, type of drug [low-dose unfractionated heparin, LDUH; low-molecular-weight heparin, LWMH; warfarin], dose, and duration), and (6) the occurrence of VTE, including DVT defined by ICD-9 coding (451.0, 451.1, 451.2, 451.8, 451.9, 453.40, 453.9, 671.4, 671.3), or PE (415.1, 415.11, 415.12, 415.19, 673.2) at 90 days following surgery.
Based on the patient’s surgery type, age, and additional VTE risk factors, each surgical admission was categorized into 4 VTE risk levels as per the 7th ACCP guidelines: “low,” “moderate,” “high,” or “very high” risk of VTE. Admissions at low risk of VTE were excluded. For all other risk categories, we determined whether pharmacologic thromboprophylaxis was prescribed (present or absent). Absent thromboprophylaxis was defined as the lack of a prescription for pharmacologic thromboprophylaxis at any time following surgery. If a prescription for thromboprophylaxis was noted following surgery, then thromboprophylaxis was considered to be present and the type, dose, and timing of pharmacologic thromboprophylaxis was compared to that recommended by the 7th ACCP guidelines according to risk category (see Table 1) and categorized as either appropriate or inappropriate. Appropriate thromboprophylaxis was defined as the recommended type of anticoagulant at the recommended dose, no later than 24 hours postsurgery, and inappropriate thromboprophylaxis was present if either the dose, the type of anticoagulant, or timing of the prescription were not in accordance with the 7th ACCP guidelines. We did not include graduated compression stockings or intermittent pneumatic compression devices in the definition of appropriate thromboprophylaxis, because the CIRESSS databank does not contain data on mechanical prevention devices. Because certain risk factors for VTE were not available in the CIRESSS database, such as oral contraceptive use or hormone replacement therapy, and obesity, we may have categorized admissions as being at a lower VTE risk level than they actually were. Consequently, we considered thromboprophylaxis to be appropriate for an admission if it corresponded to that admission’s risk level or higher. A computerized algorithm was used to classify each admission as having received appropriate, inappropriate, or absent thromboprophylaxis (Table 1).
Seventh American College of Chest Physicians Guidelines Specifications of Appropriate Thromboprophylactic Treatment According to Patient VTE Risk Level
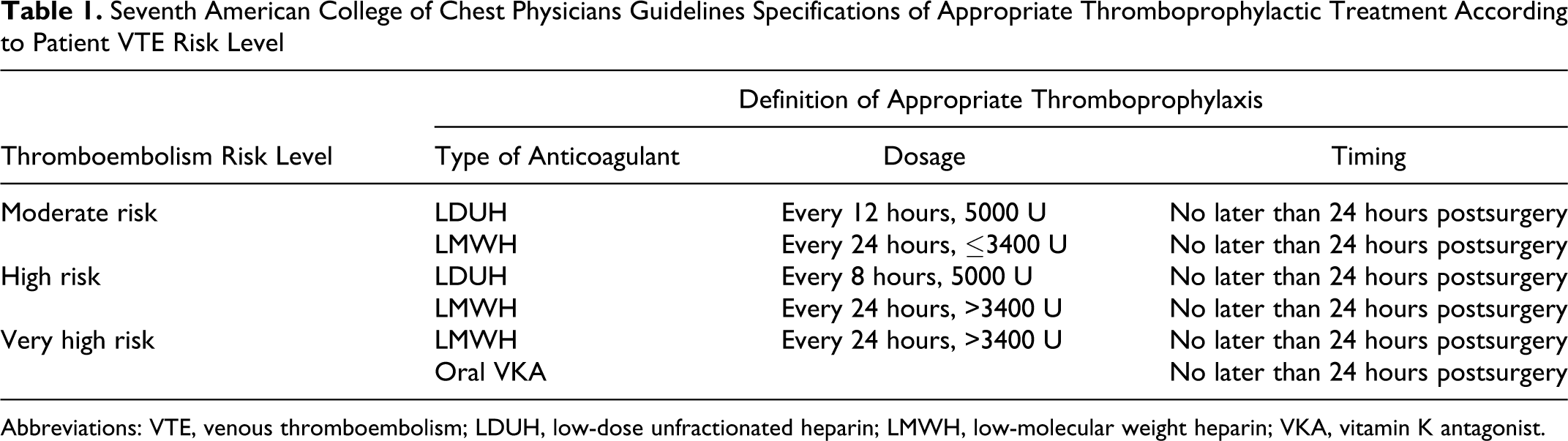
Abbreviations: VTE, venous thromboembolism; LDUH, low-dose unfractionated heparin; LMWH, low-molecular weight heparin; VKA, vitamin K antagonist.
We estimated the proportion of admissions with present thromboprophylaxis and with appropriate thromboprophylaxis. To determine which clinical factors were associated with absent and inappropriate thromboprophylaxis, multiple logistic regression analysis was used to estimate odds ratios and associated 95% confidence intervals (CI). We compared participants with and without VTE occurrence at 90 days according to VTE risk level and thromboprophylaxis absence and appropriateness using chi-square test, Student t test or Fisher exact, as appropriate. All statistical analyses were performed by means of a statistical computer program (STATA 10.1; Stata Corp., College Station, Texas).
Results
We identified a total of 4823 consecutive admissions to the surgical ward of the CHUS between January 1, 2006, and December 31, 2006. We excluded 2109 admissions with duration of stay of less than 24 hours, 187 admissions for minor orthopedic surgeries (nonlaparoscopic endoscopic and endoluminal surgeries) for which thromboprophylaxis is not recommended by the 7th ACCP guideline, 195 admissions in which the patient was deemed at low risk of VTE as per the 7th ACCP guideline, 35 admissions in which the patient was under the age of 18 years, and 11 admissions in which patients had contraindications to anticoagulant prescription. Our final study population included 2286 surgical admissions. Patient-related and surgery-related characteristics of the 2286 admissions, representing 2205 individual patients, are presented in Table 2. The average patient age was 60.5 years and women accounted for 55.8% of admissions. The majority (59.7%) of admissions were classified as being at a very high VTE risk level. Cancer within 90 days preceding surgery was the most common VTE risk factor and was present in 787 (34.4%) of admissions.
Patient and Surgery-Related Characteristics of Admissions a
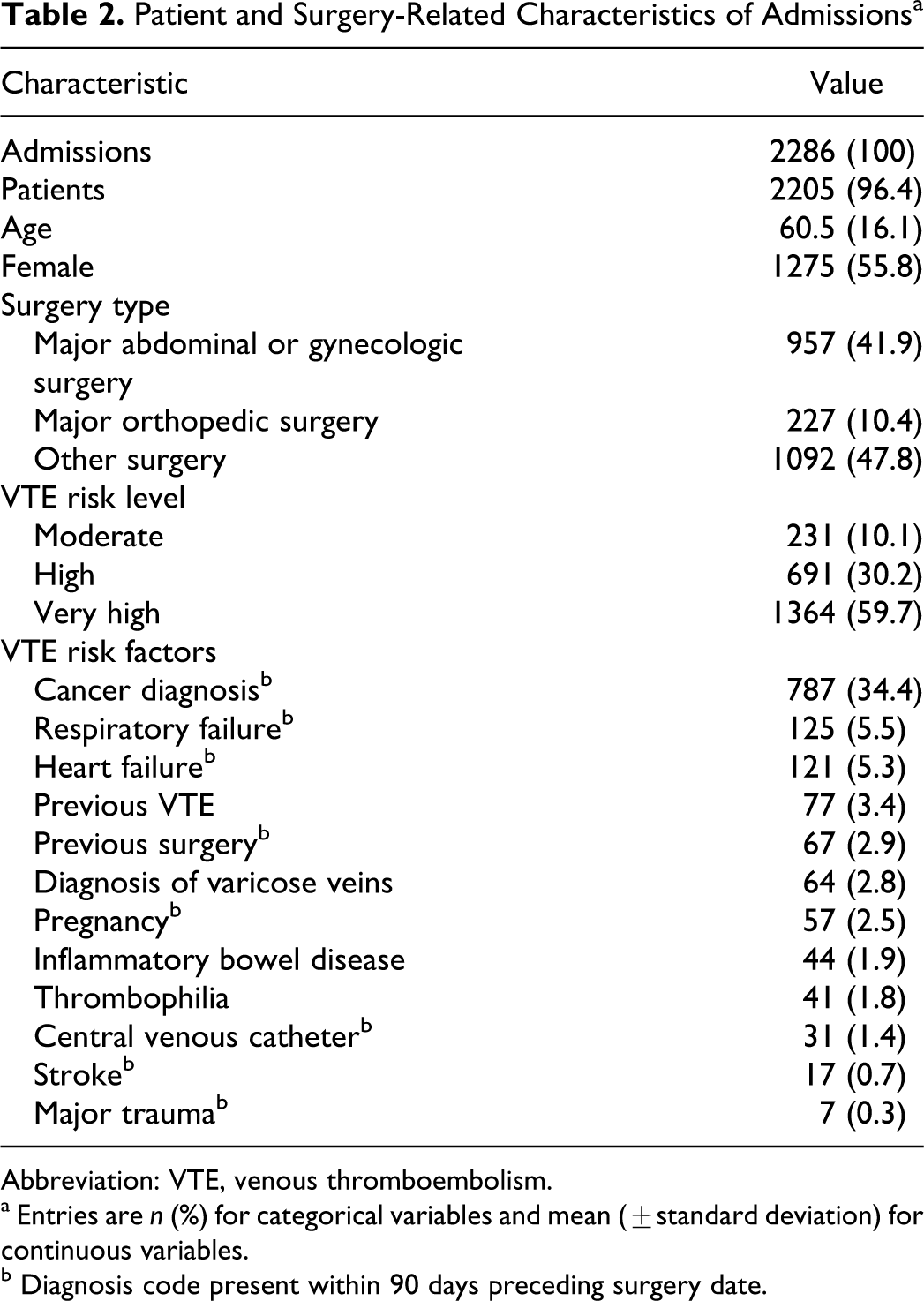
Abbreviation: VTE, venous thromboembolism.
a Entries are n (%) for categorical variables and mean (±standard deviation) for continuous variables.
b Diagnosis code present within 90 days preceding surgery date.
Overall, thromboprophylaxis was present in 1852 (81.0%) of admissions and appropriate thromboprophylaxis was observed in 582 (31.4%) of admissions that received thromboprophylaxis (Table 3). The use of thromboprophylaxis ranged from a minimum of 58.9% in at-risk patients under the age of 40 years to a maximum of 96.7% in patients with a recent diagnosis of heart failure. At-risk patients under the age of 40 years were also the least likely to receive appropriate prophylaxis (9.6%), while the highest prevalence of appropriate prophylaxis was observed in admissions for major orthopedic surgery (93.8%). With regard to surgery type, thromboprophylaxis was least present (70.4%) among admissions for procedures other than major orthopedic, abdominal, and gynecologic surgery, such as mastectomy and carotid endartectomy, and least appropriate among admissions for major abdominal or gynecologic surgery, with 11% of these admissions having received an appropriate prophylaxis regimen.
The Prevalence of Present and Appropriate Thromboprophylaxis Among Study Population of n = 2286 Surgical Admissions
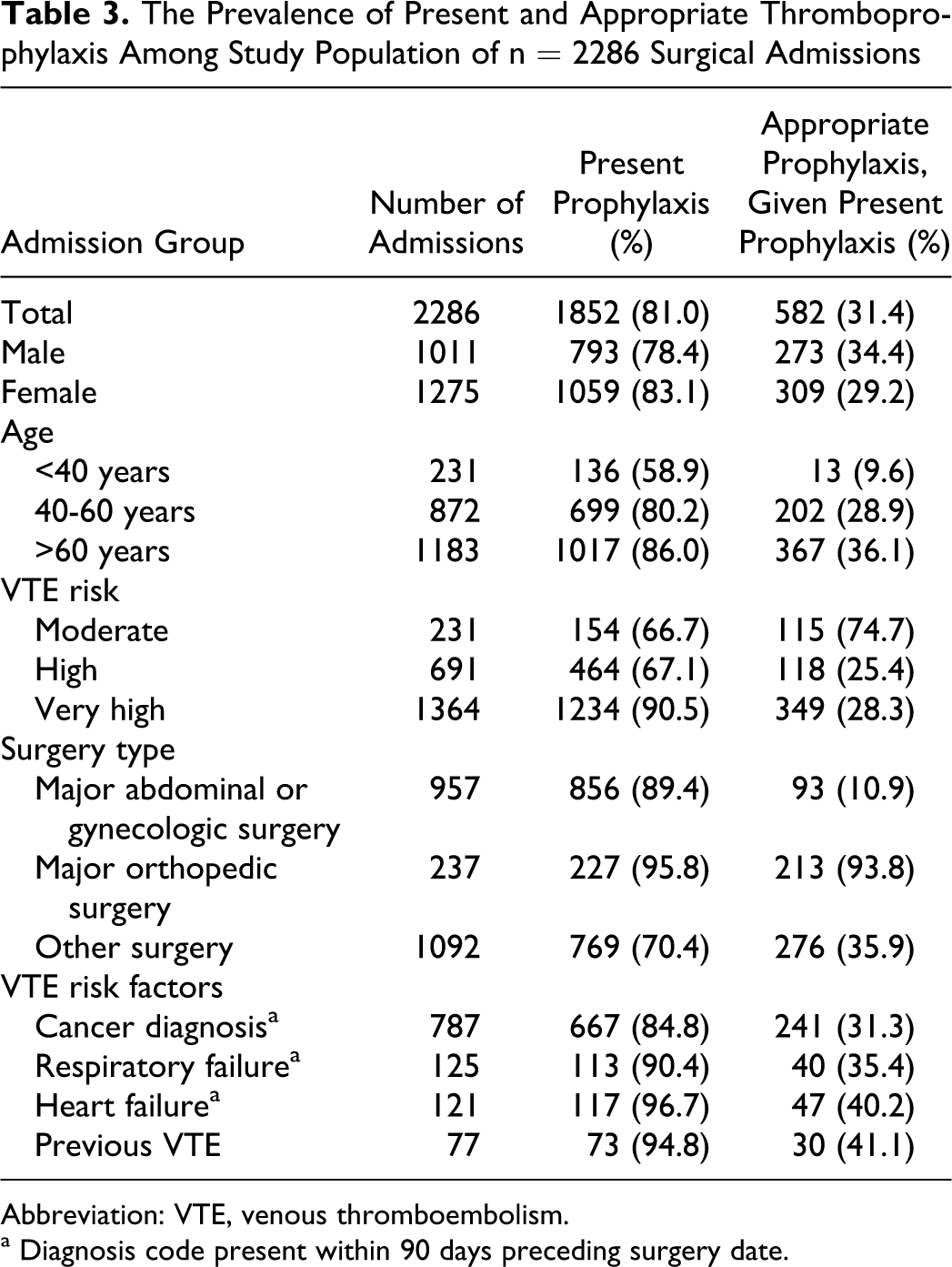
Abbreviation: VTE, venous thromboembolism.
a Diagnosis code present within 90 days preceding surgery date.
Table 4 presents associations between patient- and surgery-related characteristics and both absent and inappropriate thromboprophylaxis. Compared to women, men were less likely to receive thromboprophylaxis (adjusted OR 1.65, 95% CI (1.27-2.17)). There was no difference between men and women with regard to receiving appropriate thromboprophylaxis. Younger age groups versus the 60 years and older age group and shorter duration hospital stay versus greater than 13 days stay were significantly associated with absent thromboprophylaxis (adjusted OR 3.11, 95% CI [2.11-4.58] and OR 14.36, 95% CI [8.95-23.0], respectively) and inappropriate thromboprophylaxis (OR 5.94, 95% CI [2.96-11.94] and OR 2.44, 95% CI [1.67-3.58], respectively). With regard to VTE patient risk factors, only a diagnosis of cancer or heart failure within 90 days preceding surgery were significantly associated with appropriate thromboprophylaxis (adjusted OR 0.43, 95% CI [0.33, 0.57] and OR 0.43, 95% CI [0.26,0.70], respectively). No patient risk factors were significantly associated with absent thromboprophylaxis.
Associations Between Patient-and Surgery-Related Characteristics and Thromboprophylaxis
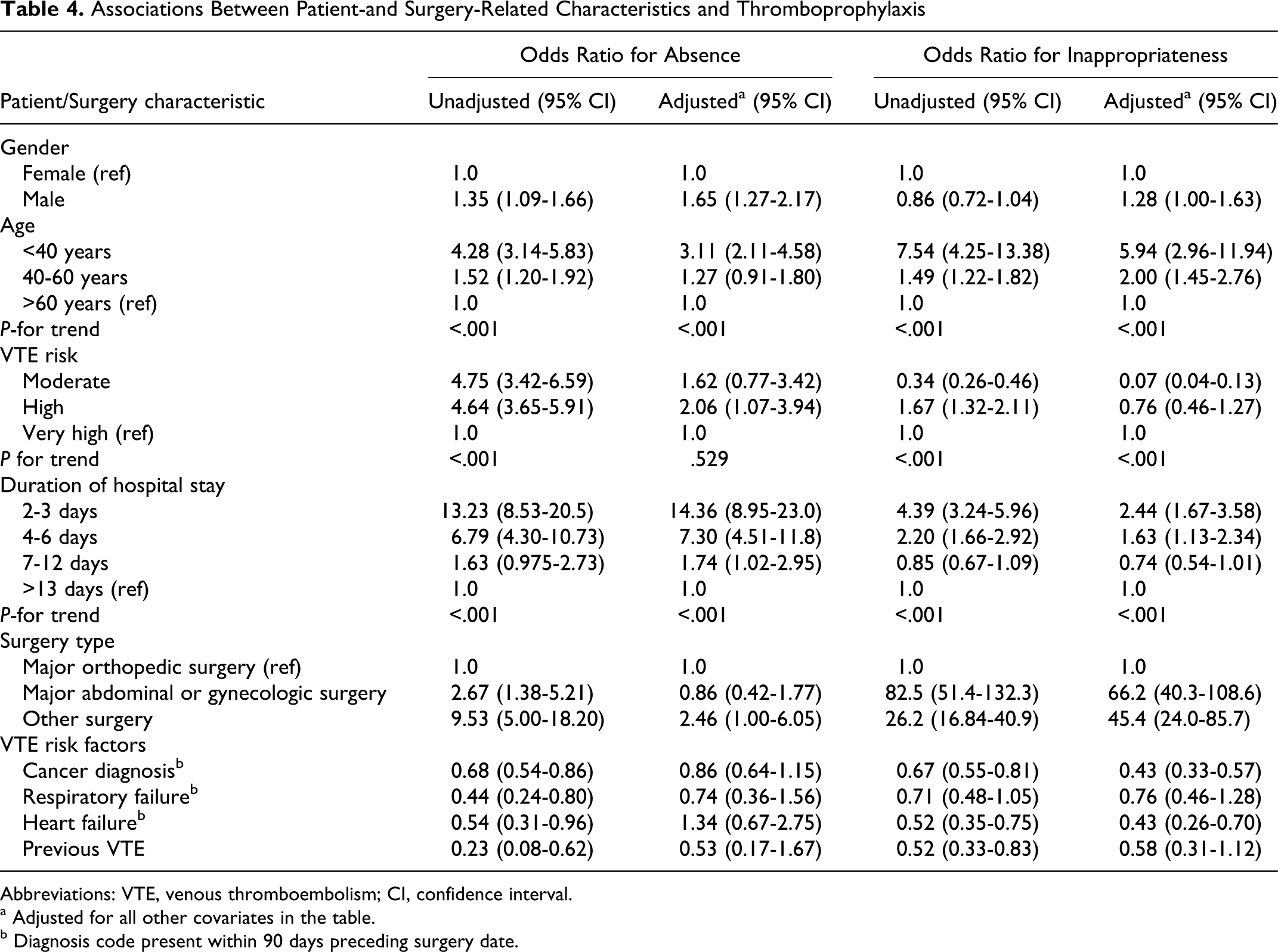
Abbreviations: VTE, venous thromboembolism; CI, confidence interval.
a Adjusted for all other covariates in the table.
b Diagnosis code present within 90 days preceding surgery date.
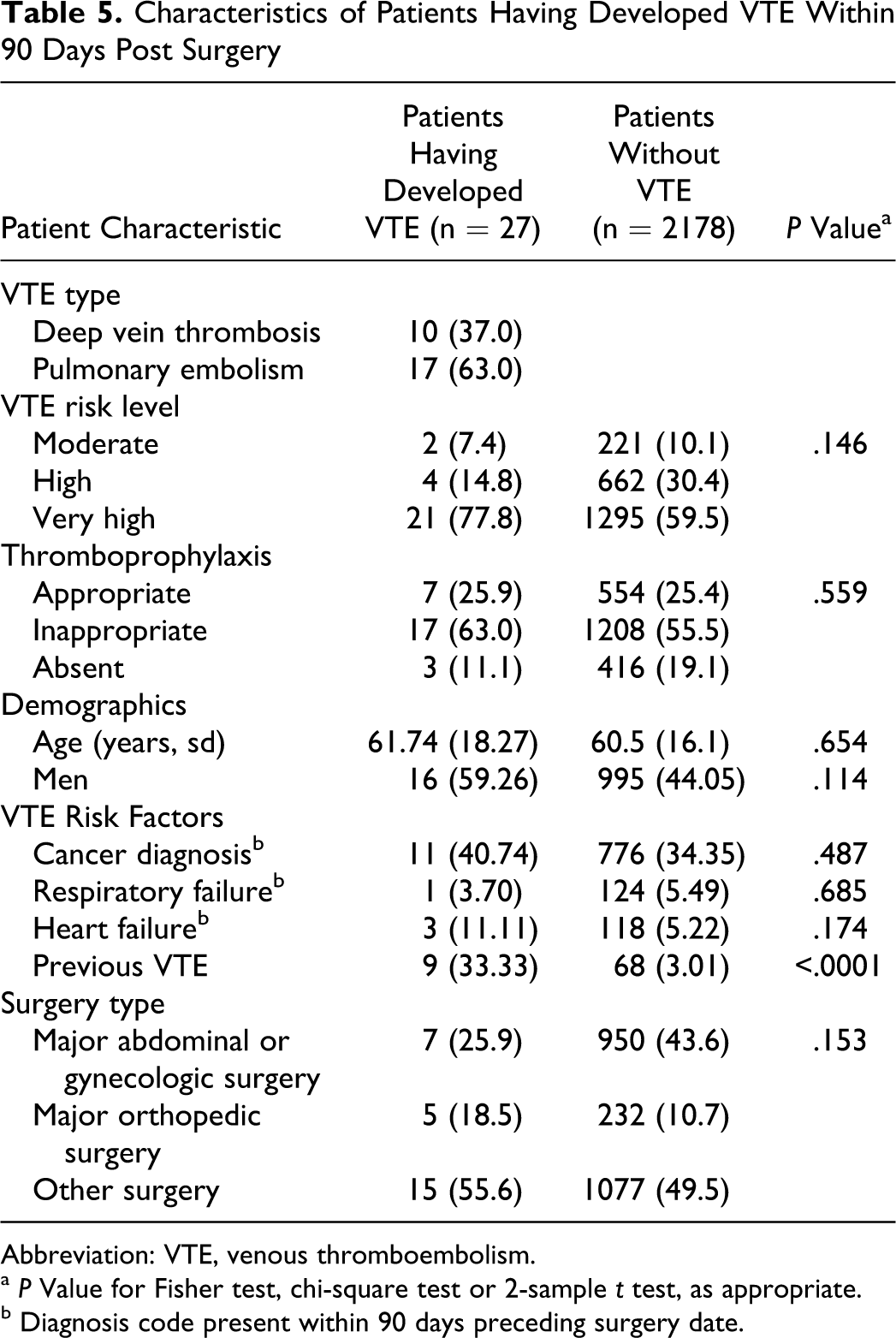
Overall, 27 (1.22%) patients developed VTE within 90 days following surgery, among whom, 17 were diagnosed with DVT alone and 10 with PE. There were no significant differences among patients with postoperative VTE versus patients without postoperative VTE with regard to VTE risk level and present and appropriate thromboprophylaxis rates (Table 5). A prior diagnosis of VTE was noted in 33.3% patients who developed VTE compared to 3.0% of patients who did not develop VTE at 90 days (P < .0001).
Characteristics of Patients Having Developed VTE Within 90 Days Post Surgery
Abbreviation: VTE, venous thromboembolism.
a P Value for Fisher test, chi-square test or 2-sample t test, as appropriate.
b Diagnosis code present within 90 days preceding surgery date.
Discussion
In our study of more than 2000 surgical admissions, we demonstrated that more than 80% of at-risk surgical patients received some form of pharmacological thromboprophylaxis. Our rate is higher than previously published rates that range anywhere between 19% and 60%.16,19–22 For example, the ENDORSE investigators determined that among 19 842 at-risk surgical patients from 32 countries, 10901 (55.5%) patients received some form of anticoagulant. Of note, ENDORSE was a world-wide study of guideline adherence rates, and there are significant differences in guideline adherence in some of the 32 countries in comparison to North America. Compared to the ENDORSE study, our population included a higher proportion of orthopedic admissions, which may have explained the higher rate of thromboprophylaxis.
We determined that absent thromboprophylaxis was associated with nonorthopedic surgery, short duration of stay, moderate VTE risk level (as compared to high), male sex, and younger age. In particular, patients undergoing orthopedic surgery were twice as likely to receive thromboprophylaxis as patients undergoing other types of surgery. VTE prophylaxis presence and appropriateness were superior in patients undergoing orthopedic surgery as compared to the other surgical patient populations. Subgroup analyses of presence and appropriateness by type of orthopedic surgery (eg, total hip replacement, total knee replacement, open reduction internal fixation) would be interesting to examine further, although this data was accessible for the purposes of this study. Despite evidence from pooled data showing that the overall incidence of VTE among general surgery patients is approximately 20% without prophylaxis, 1 the perceived risk of VTE in patients undergoing nonorthopedic surgery compared to orthopedic surgery may be considered low among health professionals. 23 Moreover, there was a significant trend toward increasing use of thromboprophylaxis and increasing duration of stay. Compared to stays greater than 13 days’ duration, surgical admissions with stays of 2 to 4 days were 93% less likely to have received thromboprophylaxis, stays 4 to 6 days were 86% less likely to have received thromboprophylaxis, and stays of 7 to 12 days were 43% less likely to have received thromboprophylaxis. Though it can be hypothesized that the higher prophylaxis rate with longer duration of stay may be attributed to a perceived high risk of thrombosis with increasing immobilization, it is more likely that a longer hospital stay leads to more patient-physician interactions, and as a result more opportunities for thromboprophylaxis to be prescribed. Surgical patients with known VTE risk factors such as underlying cancer, recent respiratory failure, heart failure, or a previous history of VTE were more likely to be prescribed any and appropriate thromboprophylaxis than patients without these risk factors (despite these patients also being at risk for postoperative VTE). The perceived risk of postoperative VTE is certainly higher in patients with established comorbidity risk factors than other risk factors such as advanced age and type of surgery. Finally, it is unclear why men are 1.7 times less likely to be prescribed thromboprophylaxis than women despite adjustment for surgery type and VTE risk factors, other than perhaps the risk of bleeding is perceived to be higher in men than in women.
Though 80% of admissions received some form of thromboprophylaxis, only 31.4% of these admissions received appropriate thromboprophylaxis in accordance with the 7th edition ACCP guidelines. Appropriate thromboprophylaxis rates vary widely in the literature and range anywhere between 16% and 63%. This wide variability is likely due to differences in patient populations and criteria used for defining appropriate thromboprophylaxis. For example, a recent Brazilian study found that among 589 surgical patients considered at risk of VTE, 63% received appropriate prophylaxis, in accordance with ACCP guidelines. 15 Amin and collegues collected data on 188 800 surgical discharges in the United States and found that only 16.4% of patients received appropriate thromboprophylaxis. 24 Their analyses were restricted to patients with a duration of hospital stay of 6 days or longer, which may have selected higher risk patients with more stringent recommended prophylaxis regimens. A cross-sectional study conducted in Spain found an appropriateness rate of 42%. 25 However, this study included patients admitted to critical care wards, where adequacy rates were particularly high (86%), and treatment appropriateness was defined as adherence to a combination of guidelines,26,27 as determined by an institutional working group comprised of hematologists, clinical pharmacologists, surgeons, other clinical specialists, and nurses. It remains unclear why our rate of appropriate thromboprophylaxis rate was lower than most previously published rates. One possible explanation is that unlike previous studies,14,17,28,29 we did not include nonpharmacologic methods of thromboprophylaxis, and as a result, we may have underestimated the appropriateness rate. Nonetheless, we can hypothesize that the high rate of thromboprophylaxis use and low rate of appropriate thromboprophylaxis observed in our study suggest a general awareness of the need for VTE prophylaxis in at-risk surgical patients among physicians but perhaps a lack of awareness or familiarity with the guidelines themselves. As with presence of thromboprophylaxis, female sex, high VTE risk level, orthopedic surgery, and longer duration of stay were positively associated with appropriate thromboprophylaxis.
In all, among the 2205 surgical patients, 27 (1.22%) developed VTE up to 90 days following surgery. Of these, 20 (74.1%) did not receive thromboprophylaxis or received inappropriate thromboprophylaxis. Hence, these represent 20 VTE events that were probably preventable as they arose in a context in which prophylaxis was recommended but not given or given inappropriately. The other 10 VTE events were likely nonpreventable. Some authors 30 suggest that these nonpreventable cases demonstrate the limitations of the ACCP guidelines, although it is well established that thromboprophylaxis regimens are not 100% effective. 1 Present and appropriate thromboprophylaxis rates were not statistically different among patients with VTE versus without VTE, and differences with regard to baseline characteristics were not found, other than a previous history of VTE being more frequent in patients with postoperative VTE.
Our study has several limitations. First, though the CIRESSS database has been previously used for research purposes, 31 it has not been validated for the diagnosis of VTE and so misclassification of VTE occurrence is possible. Furthermore, objective-confirmation of VTE (from Doppler ultrasound, venogram, V/Q scan or spiral CT scan, as appropriate) was not reported in CIRESSS. Second, as our study was retrospective in nature, we could not fully evaluate the circumstances that may have led physicians to prescribe prophylaxis in a manner that may not comply with the 7th ACCP guidelines. Third, the CIRESSS database did not contain data on mechanical devices for thromboprophylaxis such as graduated compression stockings and as a result we may have overestimated the rates of absent and inappropriate thromboprophylaxis. Fourth, we may have underestimated the incidence of postoperative VTE since discharged study patients who developed postoperative VTE may have sought care from or referred to institutions other than CHUS and as a result not captured by the CIRESS database. This is likely a rare occurrence since most patients are usually faithful to their health care institutions, especially patients with very recent surgery. Also, we did not determine postoperative mortality and as a result may have missed fatal PE events. Importantly, since this study was conducted, the 8th ACCP guidelines have been released. 32 As compared to the 7th ACCP guidelines, the recommended duration of use of prophylaxis in patients undergoing hip and knee surgery has been increased. However, we did not assess the duration of prophylaxis in this study.
Our study highlights a higher than previously published rate of thromboprophylaxis use among surgical patients and a relatively low rate of appropriate prophylaxis. This suggests that efforts and interventions aimed at improving awareness of the need for VTE surgical thromboprophylaxis have been somewhat successful but more effort and interventions are needed specifically designed to increase appropriate application of published guidelines in the real world. As such, future research is needed to better understand the reasons and barriers to appropriate use of guideline recommendations, especially among young men, hospitalizations of short duration, and patients without major VTE risk factors.
Footnotes
This study was presented at the International Society of Thrombosis and Haemostasis meeting 2009 Boston (Oral Presentation).
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.