In patients presenting non-high clinical pretest probability (PTP), a negative d-dimer can exclude venous thromboembolism without imaging tests. However, each d-dimer assay should be validated in prospective studies. We evaluated an automated d-dimer immunoassay using the Sclavo Auto d-dimer (Sclavo Diagnostics Int, Sovicille, Italy) provided by Dasit Diagnostica (Cornaredo, Milan, Italy). Three hundred two consecutive outpatients suspected of leg deep vein thrombosis (DVT) with non-high PTP were included. The Sclavo Auto d-dimer assay was evaluated on 2 analyzers (Sysmex CA-7000 and Sysmex CS-2100; Sysmex Corporation, Kobe, Japan, provided by Dasit). The cutoff value (200 ng/mL) was established a priori. Prevalence of DVT was 11.9%. Since no false-negative patients were detected, the sensitivity and negative predictive values (NPVs) were 100% (sensitivity = CA-7000: 100% [95% confidence interval, CI: 93.3-100], CS-2100: 100% [95% CI: 93.3-100]; NPV = CA-7000: 100% [95% CI: 97.9-100], CS-2100: 100% [95% CI: 98.0-100]). Specificity was 65.4% (95% CI: 59.4-71.1) and 69.2% (95% CI: 63.3-74.7) for CA-7000 and CS-2100, respectively. Specificity increased when a higher cutoff value (234 ng/mL) was used for patients aged ≥60 years without compromising the safety. Assay reproducibility was satisfactory at concentrations near the cutoff value (total coefficient of variations <10%). In conclusion, the Sclavo Auto d-dimer assay was accurate when used for DVT diagnostic workup in outpatients with non-high PTP. Based on its high sensitivity and NPV, it can be used as a stand-alone test in outpatients with non-high PTP. Given its high specificity, the number of patients in whom further imaging techniques can be avoided increased, improving the yield of the test.
d-Dimer measurement is widely used in the diagnostic workup of deep vein thrombosis (DVT) and pulmonary embolism (PE) in outpatient population referred to the emergency department because of suspected venous thromboembolism event (VTE). d-Dimer testing has to be integrated with comprehensive, sequential diagnostic strategies that also include pretest clinical probability (PTP) assessment and imaging techniques (ie Doppler ultrasonography, scintigraphy, and computed tomography). Given its high sensitivity and negative predictive value (NPV), a negative d-dimer test can safely rule out VTE event in outpatients presenting a non-high PTP, without performing imaging test.1–4
However, the performance of each d-dimer assay should be evaluated in specific prospective outcome studies in the appropriate patient population before clinical use because of the lack in standardization of this assay, heterogeneity of the mixture of the analytes measured, difference in the antibodies and calibrators used in the assay, and different measurement units. Moreover, given the great number of methods that are nowadays available, based on different techniques and with variable clinical performance, the choice of the d-dimer assay for VTE exclusion should take into account the coefficient of variation (CV) at the cutoff point and the results in terms of sensitivity and specificity.5–8
Recent studies have underlined that, since d-dimer levels increase with age, the use of the conventional cutoff value in older patients is associated with a decrease in specificity with advancing age and with an increasing request of unnecessary imaging tests.9–11 The introduction of age-adjusted cutoff values for non-high PTP older patients with suspected PE or DVT has proved to increase specificity without compromising sensitivity.12–16
Here, we report on the analytical performance and the diagnostic accuracy of the application of an automated immunoturbidimetric assay, the Sclavo Auto d-dimer (Sclavo Diagnostics Int, Sovicille, Italy) on 2 different analyzers, the Sysmex CA-7000 and the Sysmex CS-2100 (Sysmex Corporation, Kobe, Japan), in outpatients with suspected DVT.
Materials and Methods
Patients and Study Protocol
Consecutive outpatients with suspected DVT of a lower limb referred from January 2010 to April 2012 at the emergency department of our clinic were evaluated. The study was designed as a management study with a 3-month follow-up. For the diagnosis of DVT, a clinical algorithm including PTP, d-dimer levels measured by the local routine assay (Liatest D-Di, Diagnostica Stago, Asniéres-sur-Seine, France), and compression ultrasonography (CUS) imaging was used, as described elsewhere.17 At presentation, the PTP was evaluated using the Wells score for DVT18; patients were classified as having a non-high PTP if the Wells score was ≤2 and a high PTP if the Wells score was >2. The CUS test was repeated after 5 to 7 days in patients with a negative initial CUS examination if they presented a high PTP or a positive d-dimer test (>500 ng/mL FEU). Patients who tested negative for DVT, at presentation or 5 to 7 days after, received a personal interview by a study nurse or a doctor after 3 months to assess their health condition. Patients were considered DVT positive in case of absence of compressibility of the common femoral and/or popliteal veins on CUS at presentation or 5 to 7 days after, or if a symptomatic VTE event, verified by objective testing, occurred within 3 months after presentation.
Only patients with a non-high PTP were included in the present analysis, and it was a priori established that the DVT prevalence in this population had to be at least of 10% as recommended by the H59-A guideline of the Clinical and Laboratory Standards Institute (CLSI).19 Further exclusion criteria were the following: isolated calf DVT, pregnancy, stable symptoms lasting more than 10 days, prophylactic or therapeutic anticoagulant treatment already underway at presentation, patients not available for the follow-up, refusal or inability to consent to the study, poor conditions (hemolyzed, partially clotted, etc), or insufficient volume of the blood sample.
At the initial visit, blood was collected from the antecubital vein into 0.109 mmol/L trisodium citrate; plasma was prepared by centrifugation for 20 minutes at 2000g at controlled room temperature, and d-dimer levels were measured by the routine assay. Platelet-poor plasma was distributed in coded plastic tubes, snap frozen, and stored at –70ºC for further analysis within 1 hour after collection. Later, thawed frozen aliquots of plasma samples collected at presentation were tested during 20 different working days, using the Sclavo Auto d-dimer by technicians unaware of the routinely assay result and the patient’s clinical outcome.
The approval of the local ethics committee was obtained as was the patient’s consent to follow the diagnostic workup adopted in our center.
Sclavo Auto d-Dimer
The Sclavo Auto d-dimer is an automated, immunoturbidimetric assay for the quantitative determination of d-dimer levels in human plasma. In our study, the assay was used on 2 different analyzers, the Sysmex CA-7000 and the Sysmex CS-2100. The Sysmex CA and CS systems are fully automated coagulation analyzers on which clotting, chromogenic, and immunologic assays can be run simultaneously. The CA-7000 is a high throughput system, whereas the CS-2100 analyzer is designed for medium-size laboratories. All reagents and instruments were provided by Dasit Diagnostica (Cornaredo, Milan, Italy). When plasma containing d-dimer is mixed with the latex reagent and the reaction buffer included in the kit, the coated latex particles aggregate and the turbidity increases. The increase in scattered light is directly proportional to the amount of d-dimer in the sample. The latex particles are coated with a monoclonal antibody that has no cross reactivity with fibrinogen. As stated by the manufacturer, the assay does not show interference for hemoglobin (up to 10 g/L), bilirubin (up to 0.5 g/L), lipid concentration (up to 20 g/L), heparin, and low-molecular-weight heparin (up to 100 U/mL); the presence of rheumatoid arthritis factor may result in false-positive results (interference not quantified), and there is no prozone effect below 130 000 ng/mL.
The results are reported in ng/mL of d-dimer unit. The linearity of the assay declared by the manufacturer is of 50 to 3500 ng/mL with auto-redilution both for lower and for higher values; results are available within 5 minutes on both the analyzers (including sample redilution if necessary).
The calibration curve was performed prior to the study using the calibrator included in the kit (lyophilized human plasma enriched with d-dimer). Each day of analysis, 2 lyophilized controls (low and high Sclavo d-dimer controls; Sclavo Diagnostics Int) were tested and, in case of controls out of range, the assay was recalibrated, and the controls retested until the results were within the specification. The clinical cutoff for VTE exclusion (200 ng/mL) was previously assessed with a derivation study (data not published). A plasma pool with a d-dimer concentration around the clinical cutoff level was locally prepared, frozen in aliquots, and tested for precision assessment.
Statistical Analysis
Sensitivity, specificity, NPV and positive predictive value, and negative and positive likelihood ratios were calculated according to standard methods for proportions; the 95% confidence interval (95% CI) limits were computed according to the binomial distribution. We also evaluated the proportion of patients in whom DVT could be excluded based on the d-dimer result using the clinical cutoff for VTE exclusion (200 ng/mL), the false-negative rates (the number of patients with VTE at diagnostic investigation or during the follow-up but with a negative d-dimer result), and the number of patients needed to test (NNT) to exclude 1 DVT (by dividing 1 by the proportion of patients in whom DVT could be excluded as previously defined).
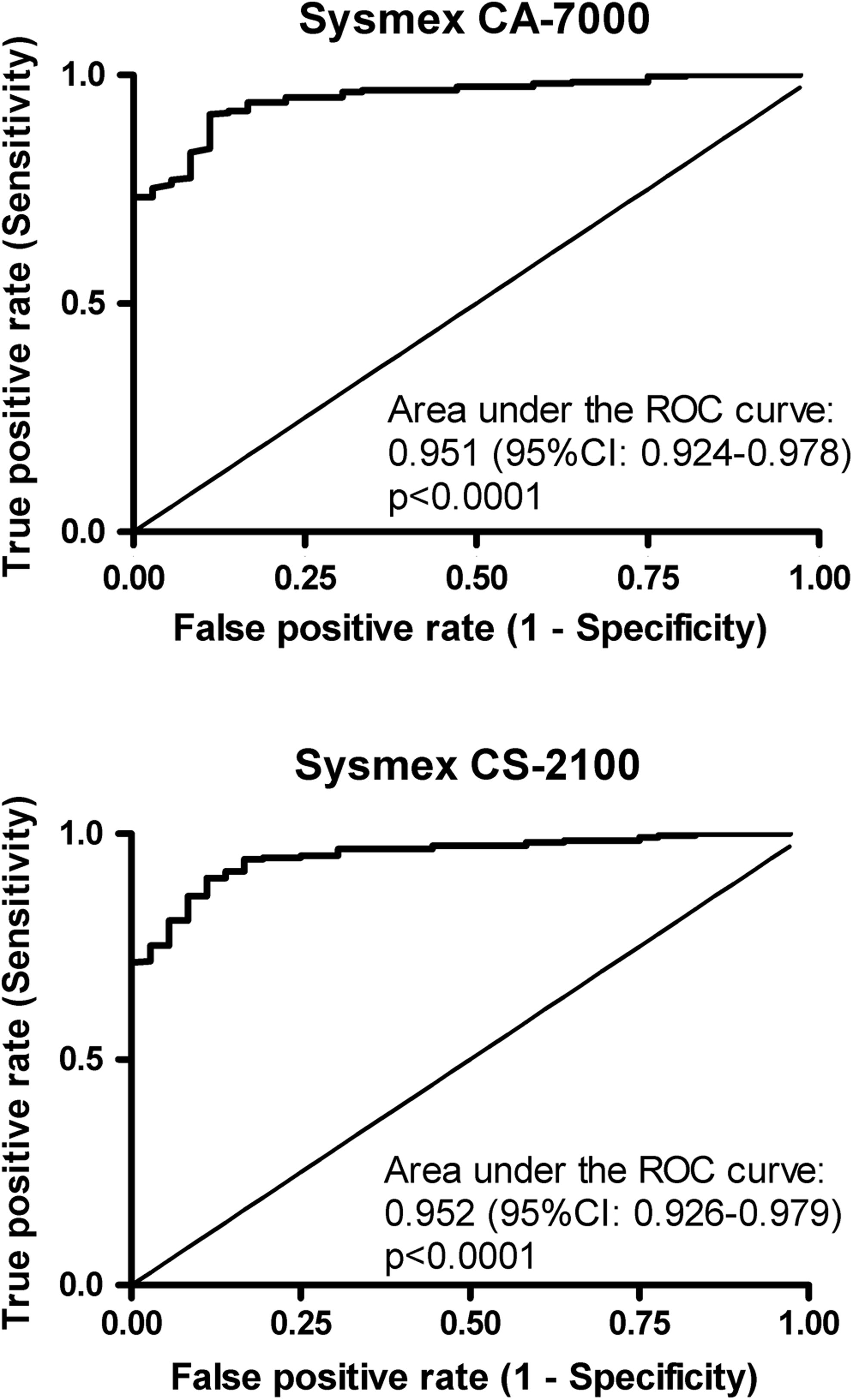
Data were also analyzed using a modified cutoff value for patients ≥60 years (234 ng/mL) and the established cutoff value for younger patients (200 ng/mL). The modified cutoff was derived performing a receiver–operating characteristics (ROC) curve analysis in the subgroup of patients aged ≥60 years and selecting the value showing the best specificity while preserving the 100% sensitivity (area under the curve resulted 0.951 [95% CI: 0.916-0.987] and 0.955 [95% CI: 0.922-0.987] for the assay performed on the Sysmex CA-7000 and Sysmex CS-2100, respectively).
Imprecision evaluation was performed according to the CLSI EP05-A2 guideline20 using the 2 lyophilized controls (low and high Sclavo d-dimer controls) and the locally prepared plasma pool with a d-dimer concentration around the clinical cutoff level. They were measured in 2 replicates per run, 2 runs per day, before and after the analysis of plasma patient samples (for 20 days [within-laboratory precision, total number of replicates, n = 80]), and in 10 replicates on the same day (within-run precision). Results are presented as mean and standard deviation (SD), and the coefficients of variation (CV%) were also calculated.
To demonstrate that linearity was within the declared performance, according to the CLSI EP06-A guideline,21 a plasma sample with high d-dimer concentration (>3500 ng/mL) was diluted in 8 different concentration ratio (ranging from 3:4 to 1:20), with the saline solution included in the Sclavo Auto d-dimer kit. The undiluted sample and each dilution were tested in triplicate. Mean observed values were plotted against the expected concentrations in order to calculate the linear regression analysis and the Pearson correlation coefficient (r value). Bias was calculated as ([mean obtained values – expected values]/expected values × 100]). An allowable bias of ±5% was considered in the analysis for linearity.
The ROC curve analysis, the linear regression analysis, and the Pearson correlation coefficient were performed and calculated using the GraphPad Software (San Diego, California).
Results
A total of 357 patients with suspected DVT of the lower limbs were referred to our outpatient clinic from January 2010 to April 2012. According to the Wells score, 55 (15.4%) patients had a high-PTP and were excluded from the present analysis. Therefore, the study population included the remaining 302 patients with non-high PTP (males: 114 (37.7%); median age [range]: 71 [13-93]; symptomatic left leg: 155 [51.3%]). In 36 patients, DVT was diagnosed (at presentation in 35 cases and 5-7 days after in 1 case), and no VTE complication was recorded at the end of the 3-month follow-up; then, the DVT prevalence resulted 11.9%.
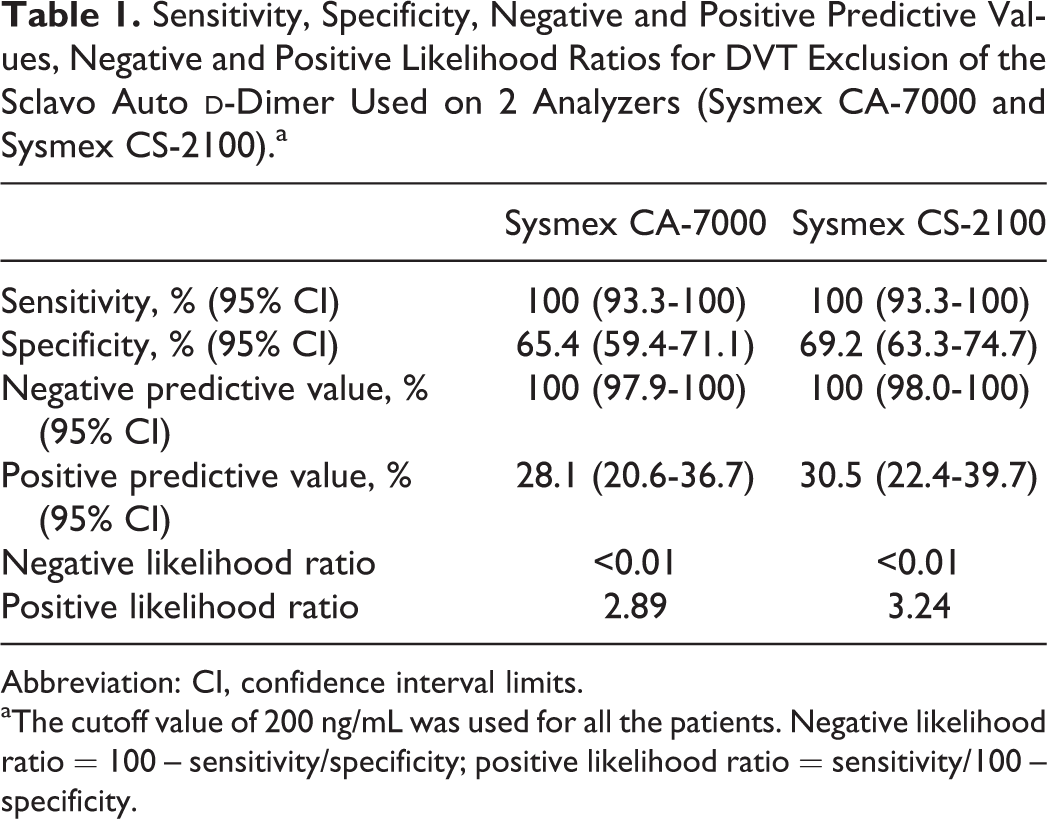
The accuracy of the Sclavo Auto d-dimer for DVT exclusion obtained using the previously established cutoff value of 200 ng/mL for all patients is presented in Table 1. Sensitivity and NPVs were 100% with both analyzers, and the lower limits of CIs were 93.3% for sensitivity with both instruments and 97.9% and 98.0% for the NPV with the Sysmex CA-7000 and Sysmex CS-2100, respectively. The negative likelihood ratios were excellent, resulting <0.01 for both analyzers. Specificity was quite high, being 65.4% (95% CI: 59.4-71.1) and 69.2% (95% CI: 63.3-74.7) with the CA-7000 and CS-2100, respectively. The ROC curves (see Figure 1) showed similar discrimination of DVT-positive and -negative patients when the Sclavo Auto d-dimer was applied on the 2 different analyzers (area under the curve: 0.951 [95% CI: 0.924-0.978] and 0.952 [95% CI: 0.926-0.979] for the CA-7000 and CS-2100, respectively).
Sensitivity, Specificity, Negative and Positive Predictive Values, Negative and Positive Likelihood Ratios for DVT Exclusion of the Sclavo Auto d-Dimer Used on 2 Analyzers (Sysmex CA-7000 and Sysmex CS-2100).a
Sysmex CA-7000
Sysmex CS-2100
Sensitivity, % (95% CI)
100 (93.3-100)
100 (93.3-100)
Specificity, % (95% CI)
65.4 (59.4-71.1)
69.2 (63.3-74.7)
Negative predictive value, % (95% CI)
100 (97.9-100)
100 (98.0-100)
Positive predictive value, % (95% CI)
28.1 (20.6-36.7)
30.5 (22.4-39.7)
Negative likelihood ratio
<0.01
<0.01
Positive likelihood ratio
2.89
3.24
Abbreviation: CI, confidence interval limits.
aThe cutoff value of 200 ng/mL was used for all the patients. Negative likelihood ratio = 100 – sensitivity/specificity; positive likelihood ratio = sensitivity/100 – specificity.
Receiver–operating characteristic (ROC) curves of the Sclavo Auto d-dimer used on the 2 different analyzers, Sysmex CA-7000 and Sysmex CS-2100.
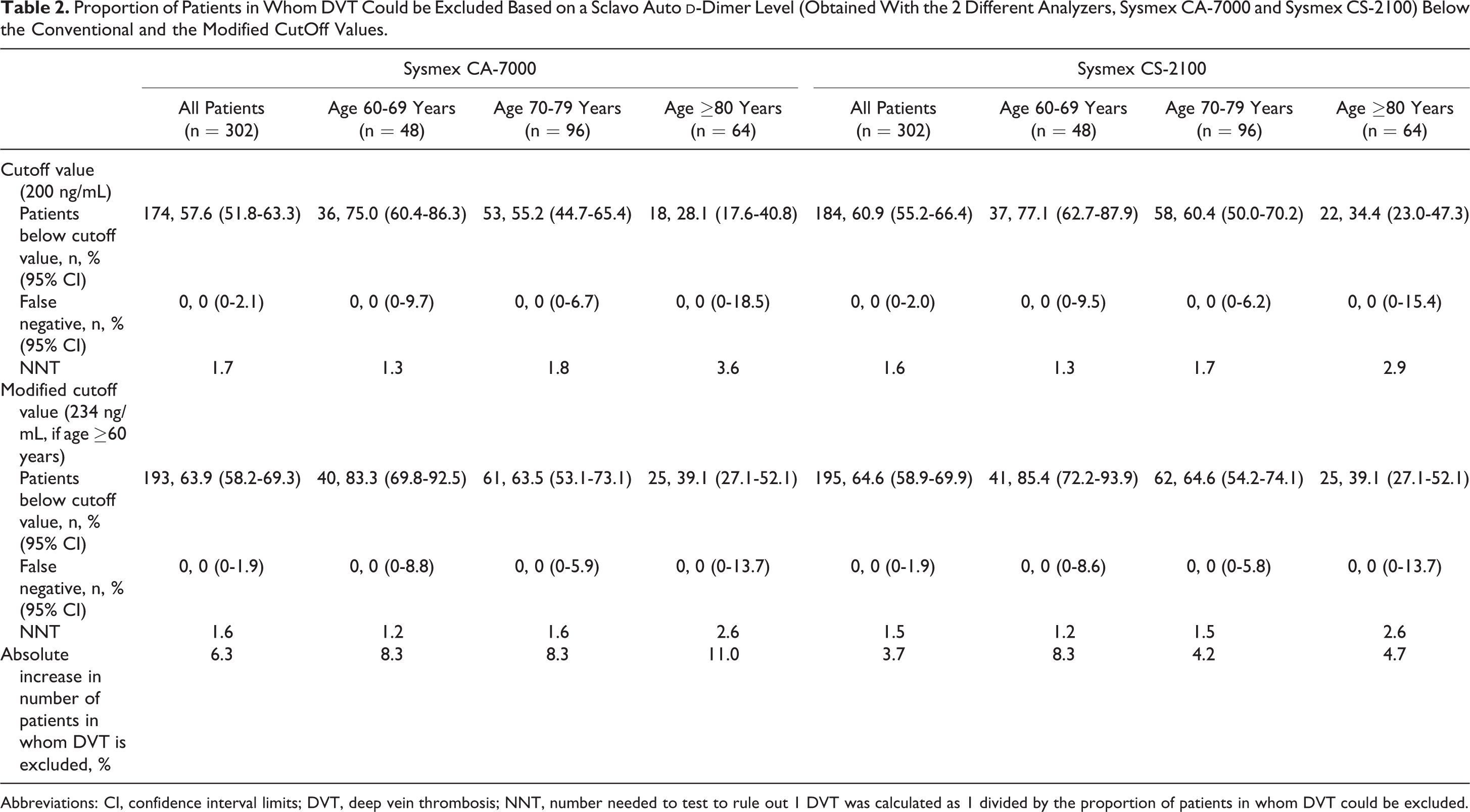
As shown in Table 2, using the cutoff value of 200 ng/mL irrespective of the patient’s age, the proportion of patients with a negative d-dimer test was 57.6% and 60.9%, and the NNT to find 1 normal d-dimer test was 1.7 and 1.6 with the CA-7000 and CS-2100, respectively. No false-negative results were recorded. Using the modified cutoff value of 234 ng/mL for patients aged ≥60 years, d-dimer test resulted negative in 63.9% and 64.6% of patients, with an absolute increase versus the results obtained using the cutoff of 200 ng/mL of 6.3% and 3.7% with the CA-7000 and CS-2100, respectively. When patients aged ≥60 years were stratified into decades, the use of the modified cutoff determined an increased efficiency in each group as shown by the absolute increase of patients in whom DVT could be excluded (ranging between 8.3% and 11.0% and between 4.2% and 8.3% with the CA-7000 and CS-2100, respectively). Increasing the efficiency did not compromise the safety: using the modified cutoff value no false-negative result was obtained during the follow-up in any age-group.
Proportion of Patients in Whom DVT Could be Excluded Based on a Sclavo Auto d-Dimer Level (Obtained With the 2 Different Analyzers, Sysmex CA-7000 and Sysmex CS-2100) Below the Conventional and the Modified CutOff Values.
Sysmex CA-7000
Sysmex CS-2100
All Patients (n = 302)
Age 60-69 Years (n = 48)
Age 70-79 Years (n = 96)
Age ≥80 Years (n = 64)
All Patients (n = 302)
Age 60-69 Years (n = 48)
Age 70-79 Years (n = 96)
Age ≥80 Years (n = 64)
Cutoff value (200 ng/mL)
Patients below cutoff value, n, % (95% CI)
174, 57.6 (51.8-63.3)
36, 75.0 (60.4-86.3)
53, 55.2 (44.7-65.4)
18, 28.1 (17.6-40.8)
184, 60.9 (55.2-66.4)
37, 77.1 (62.7-87.9)
58, 60.4 (50.0-70.2)
22, 34.4 (23.0-47.3)
False negative, n, % (95% CI)
0, 0 (0-2.1)
0, 0 (0-9.7)
0, 0 (0-6.7)
0, 0 (0-18.5)
0, 0 (0-2.0)
0, 0 (0-9.5)
0, 0 (0-6.2)
0, 0 (0-15.4)
NNT
1.7
1.3
1.8
3.6
1.6
1.3
1.7
2.9
Modified cutoff value (234 ng/mL, if age ≥60 years)
Patients below cutoff value, n, % (95% CI)
193, 63.9 (58.2-69.3)
40, 83.3 (69.8-92.5)
61, 63.5 (53.1-73.1)
25, 39.1 (27.1-52.1)
195, 64.6 (58.9-69.9)
41, 85.4 (72.2-93.9)
62, 64.6 (54.2-74.1)
25, 39.1 (27.1-52.1)
False negative, n, % (95% CI)
0, 0 (0-1.9)
0, 0 (0-8.8)
0, 0 (0-5.9)
0, 0 (0-13.7)
0, 0 (0-1.9)
0, 0 (0-8.6)
0, 0 (0-5.8)
0, 0 (0-13.7)
NNT
1.6
1.2
1.6
2.6
1.5
1.2
1.5
2.6
Absolute increase in number of patients in whom DVT is excluded, %
6.3
8.3
8.3
11.0
3.7
8.3
4.2
4.7
Abbreviations: CI, confidence interval limits; DVT, deep vein thrombosis; NNT, number needed to test to rule out 1 DVT was calculated as 1 divided by the proportion of patients in whom DVT could be excluded.
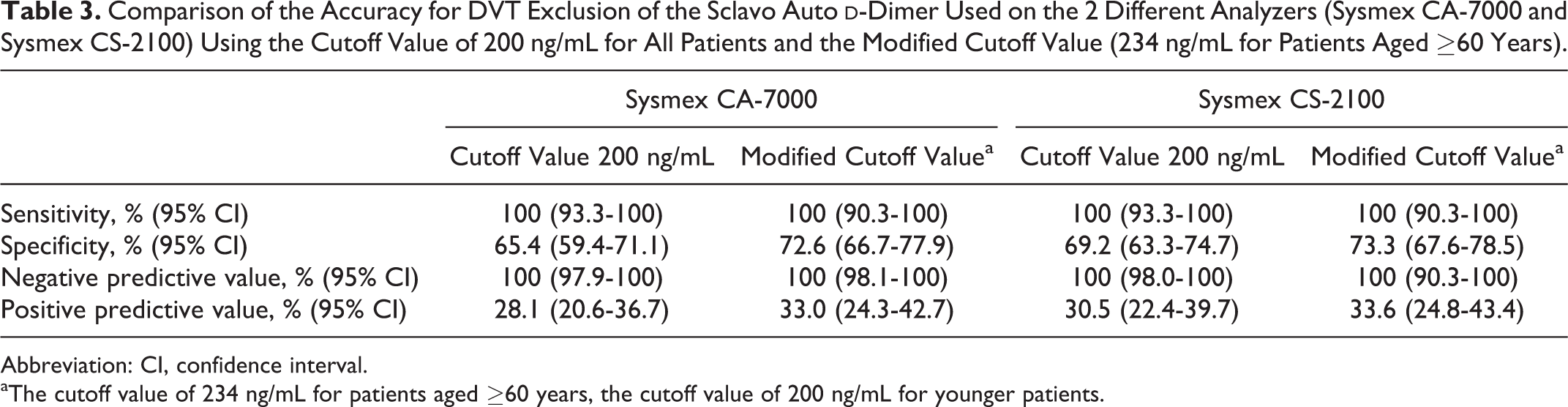
The sensitivity, specificity, NPV, and positive predictive value of the 2 different approaches to evaluate d-dimer results (cutoff values: 200 ng/mL for all patients vs higher value [234 ng/mL] for patients aged ≥60 years) are shown in Table 3. The use of the modified cutoff value was associated with a higher specificity (72.6% vs 65.4% and 73.3% vs 69.2%, with the CA-7000 and CS-2100, respectively) without any decrease in sensitivity and NPV.
Comparison of the Accuracy for DVT Exclusion of the Sclavo Auto d-Dimer Used on the 2 Different Analyzers (Sysmex CA-7000 and Sysmex CS-2100) Using the Cutoff Value of 200 ng/mL for All Patients and the Modified Cutoff Value (234 ng/mL for Patients Aged ≥60 Years).
Sysmex CA-7000
Sysmex CS-2100
Cutoff Value 200 ng/mL
Modified Cutoff Valuea
Cutoff Value 200 ng/mL
Modified Cutoff Valuea
Sensitivity, % (95% CI)
100 (93.3-100)
100 (90.3-100)
100 (93.3-100)
100 (90.3-100)
Specificity, % (95% CI)
65.4 (59.4-71.1)
72.6 (66.7-77.9)
69.2 (63.3-74.7)
73.3 (67.6-78.5)
Negative predictive value, % (95% CI)
100 (97.9-100)
100 (98.1-100)
100 (98.0-100)
100 (90.3-100)
Positive predictive value, % (95% CI)
28.1 (20.6-36.7)
33.0 (24.3-42.7)
30.5 (22.4-39.7)
33.6 (24.8-43.4)
Abbreviation: CI, confidence interval.
aThe cutoff value of 234 ng/mL for patients aged ≥60 years, the cutoff value of 200 ng/mL for younger patients.
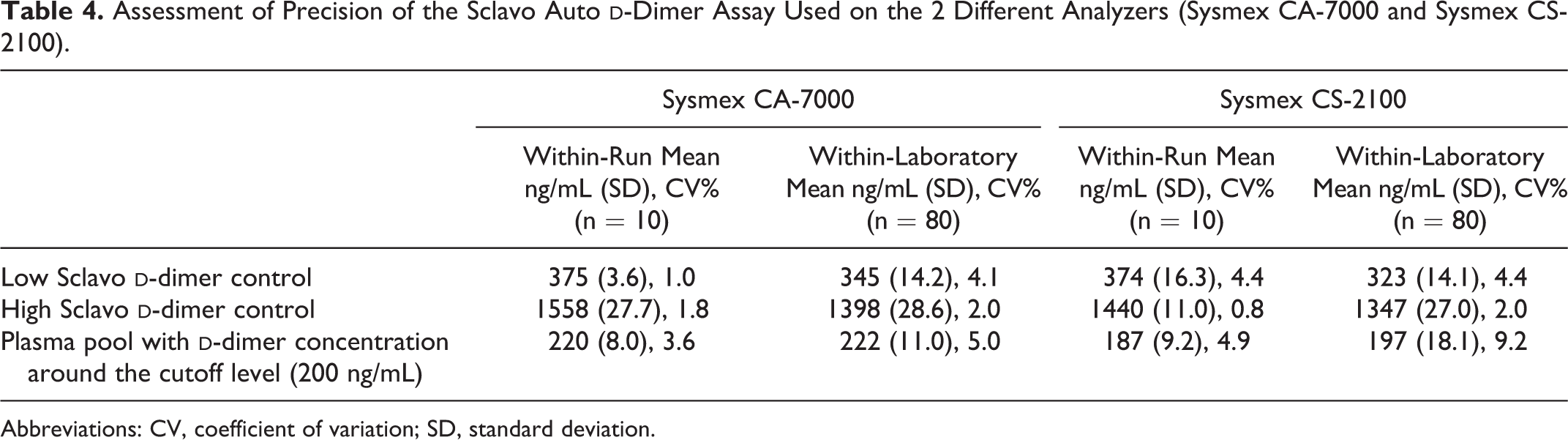
Table 4 shows the imprecision evaluation of the Sclavo Auto d-dimer assay, assessed using the results of the low- and high-lyophilized controls and the plasma pool locally prepared to obtain a d-dimer concentration around the clinical cutoff level (200 ng/mL). The within-run CV% was comprised between 1.0% and 3.6% on the CA-7000 and between 0.8% and 4.9% on the CS-2100. The within-laboratory imprecision varied from 2.0% to 5.0% and from 2.0% to 9.2%, on the CA-7000 and CS-2100, respectively.
Assessment of Precision of the Sclavo Auto d-Dimer Assay Used on the 2 Different Analyzers (Sysmex CA-7000 and Sysmex CS-2100).
Sysmex CA-7000
Sysmex CS-2100
Within-Run Mean ng/mL (SD), CV% (n = 10)
Within-Laboratory Mean ng/mL (SD), CV% (n = 80)
Within-Run Mean ng/mL (SD), CV% (n = 10)
Within-Laboratory Mean ng/mL (SD), CV% (n = 80)
Low Sclavo d-dimer control
375 (3.6), 1.0
345 (14.2), 4.1
374 (16.3), 4.4
323 (14.1), 4.4
High Sclavo d-dimer control
1558 (27.7), 1.8
1398 (28.6), 2.0
1440 (11.0), 0.8
1347 (27.0), 2.0
Plasma pool with d-dimer concentration around the cutoff level (200 ng/mL)
220 (8.0), 3.6
222 (11.0), 5.0
187 (9.2), 4.9
197 (18.1), 9.2
Abbreviations: CV, coefficient of variation; SD, standard deviation.
The Sclavo Auto d-dimer assay confirmed an excellent linearity on the CA-7000 in the measuring interval from 179 to 2691 ng/mL (y = 1.01x – 1.17; r = .999; bias range: from -1.8% to 2.1%). Similar results were obtained on the CS-2100 in the measuring interval from 191 to 2726 ng/mL (y = 1.03x – 10.45; r = .999; bias range: from –2.3% to 3.6%). At the highest concentration tested, exceeding the linearity limit, the bias of both analyzers was higher than ±5.0% (–8.5% at 3591 ng/mL and –9.1% at 3635 ng/mL for the CA7000 and CS2100, respectively).
Discussion
d-Dimer assay has been used in the management strategy for VTE exclusion for decades, and its usefulness has been well established. Due to its high sensitivity and NPV, it can be used as a stand-alone test in outpatients with non-high PTP to exclude the disease.22 One aspect that still diagnostically complicates the use of d-dimer assay is the lack of standardization between methods, necessitating proper clinical validation of each assay in the target population.5,6,23 Only d-dimer assays that have been appropriately validated in prospective outcome studies, or compared with stored plasma samples from outcome studies, should be used for clinical purpose.5
Our study evaluated an automated, immunoturbidimetric assay, the Sclavo Auto d-dimer on 2 different analyzers, the Sysmex CA-7000 and the Sysmex CS-2100, in outpatients with suspected DVT. Only patients with non-high PTP were included in the analysis. In our cohort, the prevalence of proximal DVT was 11.9%, which is comparable with that reported in similar outpatient population and higher than that recommended by the CLSI H59-A guideline.19 The test, performed on the 2 different analyzers, managed equally to discriminate DVT-positive and -negative patients as demonstrated by the ROC curve analysis. Using the a priori established cutoff of 200 ng/mL for all patients, we found that the sensitivity and NPV were 100%. Most importantly, the lower limits of the 95% CI were higher than 90% for sensitivity and higher than 95% for NPV as recommended by the CLSI H59-A guideline.19
When choosing a d-dimer assay to be used in diagnostic strategies for acute VTE, utmost attention should be paid to the sensitivity, as false-negative results can lead to potentially fatal consequences. Nevertheless, specificity is also important, since it determines the proportion of false-positive results and strongly influences the yield of the test. High specificity indeed increases the number of patients in whom further, more cost-intensive, imaging techniques can be avoided. Unexpectedly, the Sclavo Auto d-dimer showed a quite high specificity (65.4% and 69.2% for the CA-7000 and CS-2100, respectively) if compared with the local routine assay (Liatest D-Di; specificity = 56.9%, 95% CI: 50.8-63.0; sensitivity and NPV = 100%) included in the clinical algorithm used in our department for DVT diagnosis as well as with other similar immunoturbidimetric tests.17,24–27
Since d-dimer levels rise considerably with age, the diagnostic yield of d-dimer assay is quite low in the elderly patients.9–11 Recent studies have reported that the use of an age-adjusted cutoff for older patients with non-high PTP safely increases the specificity.12–16,25,26 When we used for the Sclavo Auto d-dimer, a higher cutoff value (234 ng/mL) for patients aged ≥60 years, there was an absolute increase in the proportion of patients in which DVT could be excluded, more evident in the older patient group. The use of the modified cutoff value in older patients allowed to further increase the specificity up to 73%. A useful index allowing comparison of the diagnostic yield of various d-dimer assay or of a specific assay in different clinical settings is the NNT, that is, the number of patients in whom d-dimer must be measured to rule out 1 VTE.28 In our study, when a higher cutoff was used for older patients, the NNT decreased from 4.2-11.0 to 1.3-3.6, confirming the findings of similar studies, showing that in a low-risk population, the strategy of using higher cutoff values in the elderly patients results in lower NNTs to rule out DVT.12–16,25 The increase in efficiency did not compromise the safety, and indeed no false-negative result was recorded (sensitivity and NPV remained 100%). Considering the total non-high PTP patients, the upper limit of the 95% CI of the false-negative rate was below 3% using both the convectional and the modified cutoff values, as recommended by the CLSI H59-A guideline.19
When d-dimer assays are used in diagnostic strategies for VTE exclusion, a critical point is the reproducibility at concentrations near the cutoff value.5,29 The precision of the Sclavo Auto d-dimer was found to be satisfactory when evaluated using a locally prepared plasma pool aiming to obtain a d-dimer concentration near the clinical cutoff value (within-run and within-laboratory CV%: CA-7000 = 3.6 and 5.0%; CS-2100 = 4.9 and 9.2%).
The overall technical and analytical performances lead us to conclude that the Sclavo Auto d-dimer is a suitable method for the rapid and accurate quantification of d-dimer in emergency situations. Indeed, linearity proved to be in the range declared by the manufacturer with both analyzers, the test can be performed in individual samples with a short turnaround time (<5 minutes), random access, and primary tube use.
Some limitation of the study should be pointed out. First of all, the Sclavo Auto d-dimer assay was evaluated retrospectively, and the test was performed on frozen samples. Many important studies have evaluated d-dimer in this way, since it has been shown that it is possible to freeze and thaw samples without affecting d-dimer results.30,31 It has to be noted that in our study, patients were treated and samples were collected prospectively (consecutive inclusion of all patients with defined clinical signs, standardized diagnostic work-up application, and 3-month follow-up). Second, although a high number of patients included in the present analysis, the age-group division reduced the number of participants in each group, possibly limiting the interpretation of results. Finally, this study was performed in outpatients with suspected DVT, so results may not be referred to different patient populations (eg for the diagnostic exclusion of PE).
In conclusion, the Sclavo Auto d-dimer proved to be an accurate and rapid method for the quantification of d-dimer in the DVT diagnostic workup. Based on its high sensitivity and NPV, it can be used as a stand-alone test in outpatients with non-high PTP. Given its high specificity, the number of patients in whom further, more cost-intensive, imaging techniques can be avoided is increased, improving the yield of the test. However, further prospective and multicenter studies are needed to confirm the present results.
Footnotes
Acknowledgments
The authors would like to thank Dasit for providing with the reagents used in the study.
Authors’ Note
C.L. designed the study and wrote the paper, M.C. analyzed the data, M.F. performed the analysis, G.R. managed the patients at inclusion, M.S. collected the patient follow-up data, and B.C. revised the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
1.
PerrierADesmaraisSMironMJ. Non-invasive diagnosis of venous thromboembolism in outpatients. Lancet1999;353(9148):190–195.
2.
SchutgensREAckermarkPHaasFJ. Combination of a normal D-dimer concentration and a non-high pretest clinical probability score is a safe strategy to exclude deep venous thrombosis. Circulation. 2003;107(4):593–597.
3.
BatesSMKearonCCrowtherM. A diagnostic strategy involving a quantitative latex D-dimer assay reliably excludes deep venous thrombosis. Ann Intern Med. 2003;138(10):787–794.
4.
van BelleABullerHRHuismanMV. Christopher Study Investigators. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295(2):172–179.
5.
RighiniMPerrierADe MoerloosePBounameauxH. D-Dimer for venous thromboembolism diagnosis: 20 years later. J Thromb Haemost. 2008;6(7):1059–1071.
6.
De MoerloosePBounameauxHWellsPH. D-dimer testing and venous thromboembolism: four view points. J Thromb Haemost. 2005;3(2):380–382.
7.
SteinPDHullRDPatelKC. D-dimer for the exclusion of acute venous thrombosis and pulmonary embolism: a systematic review. Ann Intern Med. 2004;140(8):589–602.
8.
Di NisioMSquizzatoARutjesAWBüllerHRZwindermanAHBossuytPM. Diagnostic accuracy of D-dimer test for exclusion of venous thromboembolism: a systematic review. J Thromb Haemost. 2007;5(2):296–304.
9.
HarperPLTheakstonEAhmedJOckelfordP. D-dimer concentration increases with age reducing the clinical value of the D-dimer assay in the elderly. Intern Med J. 2007;37(9):607–613.
10.
RighiniMNendazMLe GalGBounameauxHPerrierA. Influence of age on the cost-effectiveness of diagnostic strategies for suspected pulmonary embolism. J Thromb Haemost. 2007;5(9):1869–1877.
11.
RighiniMLe GalGPerrierABounameauxH. The challenge of diagnosing pulmonary embolism in elderly patients: influence of age on commonly used diagnostic tests and strategies. J Am Geriatr Soc. 2005;53(6):1039–1045.
12.
DoumaRAle GalGSohneM. Potential of an age adjusted D-dimer cut-off value to improve the exclusion of pulmonary embolism in older patients: a retrospective analysis of three large cohorts. BMJ. 2010;340:c1475.
13.
DoumaRATanMSchutgensRE. Using an age-dependent D-dimer cut-off value increases the number of older patients in whom deep vein thrombosis can be safely excluded. Haematologica. 2012;97(10):1507–1513.
14.
SchoutenHJKoekHLOudegaR. Validation of two age dependent D-dimer cut-off values for exclusion of deep vein thrombosis in suspected elderly patients in primary care: retrospective, cross sectional, diagnostic analysis. BMJ. 2012;344:e2985.
15.
RighiniMVan EsJDen ExterPL. Age-adjusted D-dimer cutoff levels to rule out pulmonary embolism: the ADJUST-PE study. JAMA. 2014;311(11):1117–1124.
16.
SchoutenHJGeersingGJKoekHL. Diagnostic accuracy of conventional or age adjusted D-dimer cut-off values in older patients with suspected venous thromboembolism: systematic review and meta-analysis. BMJ. 2013;346:f2492.
17.
LegnaniCCiniMScarvelisDToulonPWuJRPalaretiG. Multicenter evaluation of a new quantitative highly sensitive D-dimer assay, the Hemosil D-dimer HS 500, in patients with clinically suspected venous thromboembolism. Thromb Res. 2010;125(5):398–401.
18.
WellsPSAndersonDRRodgerM. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003;349(13):1227–1235.
19.
Clinical and Laboratory Standards Institute. Quantitative D-Dimer for the Exclusion of Venous Thromboembolic Disease; Approved Guideline. CLSI document H59-A. Wayne, PA: Clinical and Laboratory Standards Institute; 2011.
20.
Clinical and Laboratory Standards Institute. Evaluation of Precision Performance of Quantitative Measurement Methods. CLSI Document EP05-A2. Wayne, PA: Clinical and Laboratory Standards Institute; 2004.
21.
Clinical and Laboratory Standards Institute. Evaluation of the Linearity of Quantitative Measurement Procedures: A Statistical Approach; Approved Guideline. CLSI document EP06-A. Wayne, PA: Clinical and Laboratory Standards Institute; 2003.
22.
AdamSSKeyNSGreenbergCS. D-dimer antigen: current concepts and future prospects. Blood. 2009;113(13):2878–2887.
23.
RodgerMALe GalGWellsP. Clinical decision rules and D-Dimer in venous thromboembolism: current controversies and future research priorities. Thromb Res. 2014;134(4):763–768.
24.
de MoerloosePPalaretiGAguilarCLegnaniCReberGPeetzD. A multicenter evaluation of a new quantitative highly sensitive D-dimer assay for exclusion of venous thromboembolism. Thromb Haemost. 2008;100(3):505–512.
25.
CiniMLegnaniCFrascaroMSartoriMCosmiBPalaretiG. D-dimer use for deep venous thrombosis exclusion in elderly patients: a comparative analysis of three different approaches to establish cut-off values for an assay with results expressed in D-dimer units. Int J Lab Hematol. 2014;36(5):541–547.
26.
CiniMLegnaniCFrascaroMCappelliCSartoriMCosmiB. Evaluation of a chemiluminescent immunoassay, the HemosIL AcuStar D-Dimer, in outpatients with clinically suspected deep venous thrombosis. Int J Lab Hematol. 2015;37(6):e172–e174.
27.
Oude ElferinkRFLootAEVan De KlashorstCGHulsebos-HuygenMPiersma-WichersMOudegaR. Clinical evaluation of eight different D-dimer tests for the exclusion of deep venous thrombosis in primary care patients. Scand J Clin Lab Invest. 2015;75(3):230–238.
28.
PerrierA. D-dimer for suspected pulmonary embolism: whom should we test?Chest. 2004;125(3):807–809.
29.
ReberGde MoerlooseP. D-dimer assays for the exclusion of venous thromboembolism. Semin Thromb Hemost. 2000;26(6):619–624.
30.
WoodhamsBGirardotOBlancoMJColesseGGourmelinY. Stability of coagulation proteins in frozen plasma. Blood Coagul Fibrinolysis. 2001;12(4):229–236.
31.
LewisMRCallasPWJennyNSTracyRP. Longitudinal stability of coagulation, fibrinolysis, and inflammation factors in stored plasma samples. Thromb Haemost. 2001;86(6):1495–1500.