
Abstract
Objective
We aimed to explore the performance of multimodal computed tomography (CT) quantitative analysis for predicting early neurological deterioration in acute ischemic stroke (AIS) patients undergoing intravenous thrombolysis.
Methods
Data from 100 AIS patients who underwent multimodal CT and intravenous thrombolysis between January 2020 and December 2023 were collected. An END group and a non-END group were set based on the presence and absence of END after treatment.
Results
Among the 100 AIS patients, 22 developed END after intravenous thrombolysis, accounting for 22.00%. Infarct core volume was positively associated with END (P < .05), whereas ischemic penumbra volume, ASPECTS, and rLMC score showed inverse associations with END (P < .05). In multivariable analysis, infarct core volume independently increased the odds of END, while higher ASPECTS, rLMC scores, and larger penumbra volumes were associated with lower odds of END. The areas under the receiver operating characteristic (ROC) curves of infarct core volume, ischemic penumbra volume, ASPECTS and rLMC score for predicting the occurrence of END in AIS patients receiving intravenous thrombolysis were 0.761, 0.710, 0.726, 0.715 and 0.846, respectively.
Conclusion
Multimodal CT quantitative indicators like infarct core volume, ischemic penumbra volume, ASPECTS, and rLMC score have independent predictive values for the occurrence of END in AIS patients receiving intravenous thrombolysis, and their combination exhibits the highest predictive value.
Keywords
Introduction
Acute ischemic stroke (AIS), a neurological dysfunction from disrupted brain blood supply, has high mortality and disability rates. As to the treatment of AIS, the key lies in relieving occluded blood vessels, restoring cerebral blood flow, and salvaging ischemic penumbra tissues as soon as possible, which can significantly improve the prognosis of patients. 1 Currently, intravenous thrombolytic therapy is adopted as an approach for early vascular opening of AIS, and its failure is mainly ascribed to post-thrombolysis early neurological deterioration . Hence, it is essential to accurately detect the occurrence of END. In the past, whether END occurs in AIS patients after intravenous thrombolysis was mainly assessed based on the clinical indicators and signs of such patients, the evaluation criteria were subjective in most cases, and the accuracy of the assessment needs to be enhanced. 2 The infarct core volume, ischemic penumbra, and collateral circulation are closely correlated with the occurrence of END in AIS patients receiving intravenous thrombolysis.3,4 At present, brain plain computed tomography (CT) scan, brain CT perfusion (CTP), dynamic CT angiography (CTA) of the head and neck and other “one-stop” multimodal CT imaging technologies can effectively and accurately provide such diagnostic information as stenosis or occlusion of large blood vessels, establishment of collateral circulation, core infarct area, and ischemic penumbra, which can quickly offer accurate therapeutic regimens for AIS and render a basis for follow-up visits and rehabilitation.5,6 However, the correlation between multimodal CT imaging technique and the outcome of END in AIS patients receiving intravenous thrombolysis has been rarely studied.
Given this, in the present study, an investigation was carried out on the effect of multimodal CT quantitative analysis on predicting END in AIS patients receiving intravenous thrombolysis.
Material and Methods
Subjects
This study was approved by the ethics committee of our hospital, and written informed consent was obtained from all subjects. Data from 100 AIS patients who underwent multimodal CT and intravenous thrombolysis between January 2020 and December 2023 were collected. There were 59 males and 41 females aged 40-75 years old, with a mean of (59.03 ± 3.28) years old. The body mass index was 19-24 kg/m2 and averaged at (21.53 ± 0.51) kg/m2. The systolic and diastolic blood pressures were 130-158 mm Hg and 85-102 mm Hg at admission, with an average of (141.20 ± 5.15) and (95.65 ± 3.03) mm Hg, respectively.
Inclusion and Exclusion Criteria
The undermentioned inclusion criteria were adopted: (1) patients meeting relevant criteria of AIS, 7 (2) those with a duration of ischemia <4.5 h, (3) those whose family members were aware of the content of this study and had signed the informed consent form, (4) those with complete clinical data, (5) those with normal cognitive and mental function and able to cooperate with treatment, and (6) those with the indications for intravenous thrombolytic therapy.
The exclusion criteria involved: (1) patients with brain tumors, brain traumas or other diseases, (2) those with severe dysfunction of such organs like the heart, liver and kidneys, or (3) those with organ dysfunction, severe infection, electrolyte disturbance, gastrointestinal hemorrhage, hyperpyrexia, secondary epilepsy or hemorrhagic transformation of infarct foci.
General Data Collection
The next-mentioned general data were collected: age, gender (male or female), smoking history (smoking cigarettes over 4 times every week for 6 consecutive or cumulative months, with >1 cigarette/day on average) (yes or no), drinking history (drinking for ≥5 years, with mean alcohol intake ≥40 g/day for males and ≥20 g/day for females) (yes or no), comorbidities (diabetes, coronary heart disease, or hypertension), education level (high school and above, or below high school), time from onset to thrombolysis, and National Institute of Health Stroke Scale (NIHSS) score (0-42 points, with higher scores suggesting more severe nerve damage). 8 Before intravenous thrombolytic therapy, Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification [cardioembolism, small-artery occlusion, large-artery atherosclerosis, other determined etiology (infection, immune hypercoagulable state, hematologic disease, hereditary vascular disease, etc), and undetermined etiology] were determined in accordance with clinical characteristics plus imaging and laboratory examination results. In addition, infarct size (lacunar infarct, moderate infarct, and large infarct) was determined through imaging examinations.
Multimodal CT Quantitative Analysis
The 256-row Revolution CT (GE, USA) was used for all imaging examinations. Non-contrast CT was performed first (120 kV, 0.625-mm slice thickness, 320 mA), followed by CTP (120 kV, automated tube current modulation, 0.5-mm slice thickness) after intravenous injection of 80 mL iohexol (37 g/100 mL, Beijing Beilu Pharmaceutical Co.) at 3-5 mL/s, with 40 mL saline flush. CTA was then conducted (100 kV, automated tube current, 0.75-mm slice thickness) with bolus-tracking triggered at 100 HU in the aortic arch.
RAPID software (version 5.3; iSchemaView, Menlo Park, CA, USA) was used for automated post-processing. Standard RAPID thresholds were applied, with infarct core defined as CBF <30% of the contralateral hemisphere, and ischemic penumbra defined as Tmax >6 s. These parameters were automatically quantified to obtain infarct core volume and ischemic penumbra volume. The Alberta Stroke Program Early CT Score (ASPECTS) [10 blood-supply areas of middle cerebral artery (MCA) are classified into nucleus mass level (M1-M6) and above (M4-M6), 9 each area is scored 1 point, which is deducted according to the degree of ischemia in the area, and the total score ranges from 0 points (extensive infarction of the blood-supply area) to 10 points (normal brain CT)] was calculated. Regional leptomeningeal collateral circulation (rLMC) was assessed using a semi-quantitative scoring method [The leptomeningeal collateral flow in ASPECTS area (MI-M6), 10 anterior cerebral artery area, and basal ganglia area are assessed based on CTA images, with 0 points for non-visualization of arteries, 1 point for arterial visualization area less than the contralateral side, and 2 points for arterial visualization area greater than or equal to the contralateral side. The leptomeningeal artery score in the lateral fissure area is doubled, which are 0, 2, and 4 points, respectively. The total score is 20 points]. All imaging data were independently interpreted by two experienced neuroradiologists, with discrepancies resolved by consensus.
Only the quantitative parameters routinely available from our clinical RAPID workflow (core and penumbra volumes) could be extracted. Advanced perfusion-derived metrics, such as hypoperfusion intensity ratio (HIR), CBV-based indices, core–penumbra mismatch ratios, or more granular collateral metrics, were not included in the exported datasets and therefore could not be analyzed.
Assessment of Large Vessel Occlusion (LVO) and Mechanical Thrombectomy (MT)
CTA images were evaluated for the presence and location of LVO, including intracranial internal carotid artery occlusion and occlusions involving the M1/M2 segments of the middle cerebral artery or the basilar artery. LVO status was documented for all patients. Although patients met institutional criteria for endovascular therapy based on imaging findings, mechanical thrombectomy was not routinely performed at our center during the study period due to resource and workflow limitations. Consequently, all patients received intravenous thrombolysis alone, minimizing treatment-related heterogeneity in the analysis.
Diagnosis of END
END was evaluated based on changes in the NIHSS score after intravenous thrombolysis. In accordance with our institutional stroke protocol, NIHSS assessments were performed at standardized time points, including baseline, 24 h, 72 h, and on day 7 (or immediately before discharge if earlier), ensuring consistent timing across patients. END was defined as an increase of ≥4 points in the NIHSS score within 7 days following treatment. This time window was chosen to capture neurological worsening occurring during the early clinical course of AIS, including infarct progression, edema evolution, or arterial re-occlusion, which may arise beyond the first 48-72 h of onset. This definition allowed comprehensive assessment of clinically relevant neurological changes throughout the acute post-thrombolysis phase.
Assessment of post-thrombolysis intracerebral hemorrhage
Hemorrhagic complications were assessed according to ECASS II criteria. Symptomatic intracranial hemorrhage (sICH) was defined as any intracranial hemorrhage associated with a ≥ 4-point increase in NIHSS score. Asymptomatic hemorrhagic transformation (HI1/HI2, PH1) was also recorded. No sICH occurred in this cohort, and asymptomatic hemorrhagic transformation was infrequent and comparable between END and non-END groups.
Statistical analysis
SPSS 23.0 software was employed. Measurement data were described in the format of (
Results
Occurrence of END
END was observed in 22 (22.00%) out of the 100 AIS patients undergoing intravenous thrombolysis, and the remaining 78 patients did not develop END, accounting for 78.00%.
General data and multimodal CT quantitative indicators of patients in END and non-END groups
No significant differences were found in gender, age, education level, smoking history, drinking history, comorbidities, time from onset to thrombolysis, infarct size, NIHSS score, and TOAST classification between the END group and the non-END group (P > .05). The infarct core volume, ischemic penumbra volume, ASPECTS and rLMC score were of significant differences between the END group and the non-END group (P < .05) (Table 1). LVO was identified in 28 patients (28.0%), including occlusions of the ICA, M1/M2 segments of the MCA, or the basilar artery. The distribution of LVO did not differ significantly between the END group (6/22, 27.27%) and the non-END group (22/78, 28.21%) (P = .855). Besides, no cases of sICH occurred after intravenous thrombolysis in this cohort, based on ECASS II criteria. Mild asymptomatic hemorrhagic transformation (HI1/HI2 or PH1) was observed in 6 patients (6.0%), with no significant difference between the END group (2/22, 9.09%) and the non-END group (4/78, 5.13%) (P = .877). None of the hemorrhagic events contributed to END, and all END cases were attributed to ischemic progression rather than hemorrhagic complications.
General Data and Multimodal CT Quantitative Indicators of Patients in END and non-END Groups [

Correlations of multimodal CT quantitative indicators with occurrence of END in AIS patients receiving intravenous thrombolysis
According to Spearman's rank correlation analysis, the ASPECTS, ischemic penumbra volume, and rLMC score were negatively correlated with the occurrence of END in AIS patients receiving intravenous thrombolysis (r < 0, P < .05), while the infarct core volume showed a positive correlation with the occurrence of END in such patients (r > 0, P < .05) (Table 2).
Correlations of Multimodal CT Quantitative Indicators with the Occurrence of END in AIS Patients Receiving Intravenous Thrombolysis.

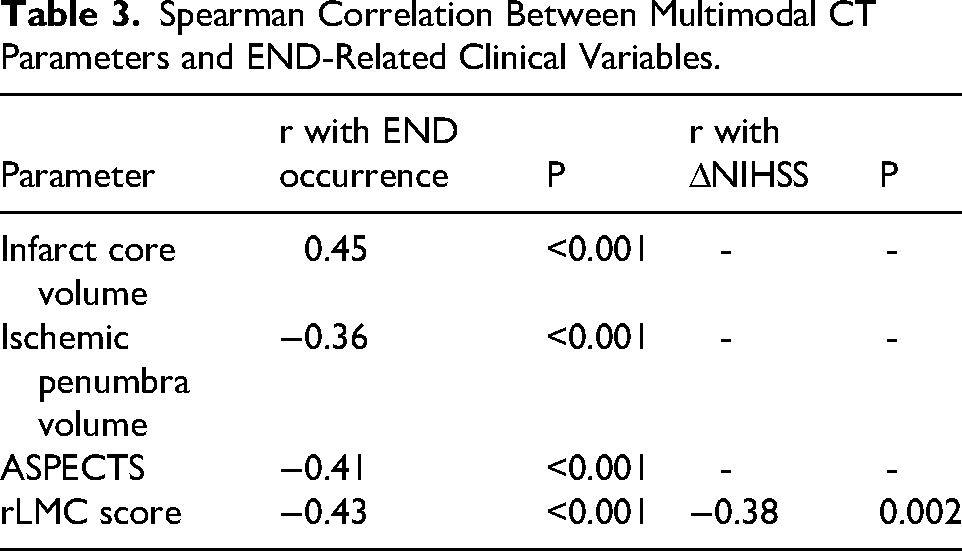
Exploratory correlation between rLMC score and neurological change
To further clarify the relationship between collateral status and neurological evolution, an exploratory analysis was performed to assess the correlation between the rLMC score and the change in NIHSS from baseline to day 7 (ΔNIHSS). A moderate negative correlation was observed (Spearman r = −0.38, P = .002), indicating that better collateral circulation was associated with less neurological worsening following intravenous thrombolysis (Table 3).
Spearman Correlation Between Multimodal CT Parameters and END-Related Clinical Variables.
Results of multivariate analysis on occurrence of END in AIS patients receiving intravenous thrombolysis
The results of Logistic regression analysis revealed that larger infarct core volume was independently associated with a higher risk of END in AIS patients undergoing intravenous thrombolysis (OR > 1, 95% CI: 1.010-1.096, P < .05). In contrast, higher ASPECTS, higher rLMC score, and larger ischemic penumbra volume were each associated with a lower likelihood of END (OR < 1, P < .05). Their corresponding 95% CIs were as follows: ischemic penumbra volume (0.851-0.968), ASPECTS (0.536-0.888), and rLMC score (0.807-0.994) (Table 4 and Figure 1). These associations likely reflect the more favorable baseline perfusion status, characterized by smaller infarct cores and better collateral circulation, observed in patients with higher ASPECTS, higher rLMC, and larger penumbra volumes.

Forest plot of clinical characteristics based on multivariate logistic regression analysis.
Results of Multivariate Analysis on Occurrence of END in AIS Patients Receiving Intravenous Thrombolysis.

Predictive value of multimodal CT quantitative indicators for occurrence of END in AIS patients receiving intravenous thrombolysis
ROC curves were plotted with the occurrence of END (0 = absence, 1 = presence) in AIS patients undergoing intravenous thrombolysis as the state variables and the infarct core volume, ischemic penumbra volume, ASPECTS, and rLMC score as the test variables. It was uncovered that the areas under curves (AUCs) of infarct core volume [95% CI: 0.630-0.892], ischemic penumbra volume [95% CI: 0.589-0.831], ASPECTS [95% CI: 0.596-0.855], rLMC score [95% CI: 0.573-0.857] and their combination for predicting the occurrence of END in AIS patients receiving intravenous thrombolysis were 0.761, 0.710, 0.726, 0.715, and 0.846, respectively (Table 5 and Figure 2).

ROC curves of multimodal CT quantitative indicators predicting the occurrence of END in AIS patients receiving intravenous thrombolysis.
Predictive Value of Multimodal CT Quantitative Indicators for Occurrence of END in AIS Patients Receiving Intravenous Thrombolysis.

Discussion
AIS remains a significant cause of disability and death, endangering the health of people. Early vascular recanalization is the key to improving the neurological function and prognosis of patients. Massive clinical practices and studies have proved that intravenous thrombolysis is not only still an effective approach for the treatment of AIS within the time window, but also the preferred therapy recommended by guidelines worldwide, which is capable of effectively relieving neurological deficits and improving the prognosis of AIS patients.11,12 Due to a short treatment window and contraindications, intravenous thrombolysis is infrequently used and sometimes ineffective in AIS patients. An important cause of a failure of intravenous thrombolytic therapy in AIS patients is the occurrence of END. 13
Therefore, assessing the risk of END in AIS patients receiving intravenous thrombolysis by effective measures and preventing and treating END through early measures are of positive significance for reducing the incidence of AIS. Currently, multimodal CT (including plain CT scan, CTA, and CTP) and other imaging technologies enable comprehensive assessment of the condition of cerebral blood vessels, rendering an imaging basis for the clinical diagnosis and treatment as well as prognosis evaluation of AIS patients. Among multimodal CT techniques, plain CT scan can help to check for intracerebral hemorrhage and determine infarct core volume. CTA is able to clearly display artery blood vessels in the head and neck of patients, identify blood vessels contributing to the infarction, and fully evaluate the existence and patency of cerebral collateral circulation in patients. CTP is capable of clearly indicating the presence or absence of ischemic penumbra (brain tissues able to restore neurological function after reperfusion).14,15 For AIS patients with small- to medium-sized core infarction, good collateral circulation, and ischemic penumbra, intravenous thrombolytic therapy enables them to have a good prognosis and satisfactory neurological recovery after treatment. 16 The above studies signify that the infarct core volume, collateral circulation, and ischemic penumbra may serve as predictors for the occurrence of END in AIS patients receiving intravenous thrombolysis.
In this study, significant differences in infarct core volume, ischemic penumbra volume, ASPECTS, and rLMC score were observed between the END and non-END groups. Correlation analysis showed that larger core volumes were associated with higher END risk, whereas higher ASPECTS, greater penumbra volume, and better collateral scores were associated with lower END risk. Logistic regression confirmed these associations, identifying infarct core as a risk factor and the other three parameters as inverse predictors of END. Importantly, no symptomatic intracerebral hemorrhage occurred, and asymptomatic hemorrhagic transformation was infrequent, suggesting that END in this cohort was mainly driven by ischemic mechanisms rather than hemorrhagic complications. In addition, an exploratory correlation analysis demonstrated a modest association between higher rLMC scores and greater NIHSS improvement, further supporting the stabilizing influence of collateral circulation on early neurological outcomes.
It is essential to clarify that the inverse association between penumbra volume and END does not imply that a larger penumbra is inherently protective. In this cohort, patients with larger penumbra volumes typically had smaller infarct cores, more favorable collateral circulation, and milder early ischemia, reflecting a more favorable physiological baseline rather than less tissue at risk. Thus, the observed inverse association likely reflects underlying perfusion status rather than a direct biological protective effect, which aligns with prior pathophysiological understanding.
The mechanisms underlying these associations are consistent with established stroke biology. A larger infarct core reflects more extensive irreversible injury and is strongly associated with neurological worsening.17,18 In contrast, the ischemic penumbra represents hypoperfused yet viable tissue that may recover if reperfusion occurs.19–20 Accordingly, a smaller penumbra suggests limited salvageable tissue and a higher likelihood of progression to completed infarction, contributing to END. Likewise, better leptomeningeal collaterals (higher rLMC score) maintain perfusion to at-risk regions and reduce ischemic expansion, whereas poor collaterals portend worse outcomes. 21 Finally, lower ASPECTS denotes more extensive early ischemia, which correlates with higher risk of deterioration and hemorrhagic transformation. 22
Notably, although a proportion of patients presented with LVO, MT was not routinely performed at our institution during the study period, and all patients were treated with intravenous thrombolysis alone. This uniform treatment approach minimizes confounding related to reperfusion strategy and allows clearer interpretation of associations between multimodal CT parameters and END risk.
The ROC curve analysis demonstrates that core volume, penumbra volume, ASPECTS, and rLMC score each have predictive value, and their combined use provides the highest accuracy, supporting the utility of multimodal CT as an integrated prognostic tool.
This study has several limitations. First, the sample size was modest, with only 22 END events, which may reduce statistical power and the stability of multivariable analyses. The single-center retrospective design further limits generalizability. Second, although LVO status was documented, MT was not performed during the study period, reducing comparability with current reperfusion practices. Third, END was defined within a 7-day window rather than the commonly used 24-72 h, which may affect cross-study consistency. Fourth, although RAPID was used, only core and penumbra volumes were available; important multimodal CT parameter, such as recanalization status, reperfusion degree, clot burden, hypoperfusion intensity ratio, CBV-based markers, detailed collateral grading, and mismatch ratios, were not consistently accessible and could not be included. Fifth, no symptomatic intracerebral hemorrhage occurred, limiting evaluation of hemorrhagic mechanisms. Sixth, representative multimodal CT images could not be provided because complete publishable imaging datasets were not uniformly available, limiting visual demonstration of imaging differences. Finally, the retrospective design may introduce selection and information bias. Prospective multicenter studies with standardized END definitions and comprehensive imaging datasets are needed.
Conclusion
Multimodal CT parameters like ischemic penumbra volume, ASPECTS, infarct core volume, and rLMC score effectively predict END risk in AIS patients, with combined use offering better prediction.
Footnotes
Acknowledgments
None.
Ethical Approval and Informed Consent Statements
This study was approved by the ethics committee of The Second Affiliated Hospital of Xuzhou Medical University, and written informed consent was obtained from all subjects.
Author Contribution Statement
Mo Chen: Data curation, Writing-original draft. Yujia Zhai: Formal analysis, Writing-original draft. Liangqun Rong: Investigation, Methodology. Xiue Wei: Project administration, Software. Haiyan Liu: Conceptualization, Writing-review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All original data are available upon reasonable request from the corresponding author.