
Abstract
To investigate the predictive role of the neutrophil-platelet ratio (NPR) before intravenous thrombolysis (IVT) on hemorrhagic transformation (HT) in patients with acute ischemic stroke (AIS). AIS patients treated with IVT without endovascular therapy between June 2019 and February 2023 were included. Patients were divided into high NPR (>35) and low NPR (≤35) groups according to the optimal threshold NPR value for identifying high-risk patients before IVT. The baseline data and the incidence of HT and symptomatic intracranial hemorrhage (sICH) were compared between the two groups. The predictive role of the NPR and other related factors on HT after IVT was analyzed by multivariate logistic regression. A total of 247 patients were included, with an average age of 67.5 ± 12.4 years. Post-thrombolytic HT was observed in 18.6% of the patients, and post-thrombolytic sICH was observed in 1.2% of the patients. There were 69 patients in the high NPR group and 178 patients in the low NPR group. The incidence of HT in the high NPR group was significantly higher than that in the low NPR group (30.4% vs 16.3%, P < .05). The incidence of sICH was significantly higher in the high NPR group than in the low NPR group (14.5% vs 1.7%, P < .001). Multivariate logistic regression analysis showed that NPR > 35 was positively correlated with HT (odds ratio (OR) = 3.236, 95% confidence interval (CI): 1.481-7.068, P = .003) and sICH (OR = 13.644, 95% CI: 2.392-77.833, P = .003). A high NPR (>35) before IVT may be a predictor of HT in AIS patients. This finding may help clinicians make clinical decisions before IVT in AIS patients.
Keywords
Introduction
Acute ischemic stroke (AIS) is the main cause of disability and death in China. At present, the key treatment for AIS is early reperfusion therapy. 1 Intravenous thrombolysis (IVT) can effectively improve the prognosis of patients and has become one of the most effective treatments for AIS. 2 It has been reported 3 that 20-30% of patients can achieve complete recalculation by IVT and that their nerve function deficits can resolve, but there are also some patients with no nerve function recovery after IVT or who even have aggravation of their symptoms. The NINDS study 4 showed that 39% of patients with IVT had a good prognosis (mRS 0-1 score) compared with 26% of the control group. The ECASSIII study 5 showed that the proportion of patients with IVT who had a good prognosis (mRS 0-1 score) was 52.4%, compared with 45.2% in the control group. The EXTEND study 6 showed that the proportion of patients with IVT who had a good prognosis (mRS 0-1 score) was 35.4%, compared with 29.5% in the control group. Thus, for patients with AIS, IVT can basically improve the 90-day good prognosis of patients by 10%. Apart from mechanical thrombectomy, this is the only effective treatment that truly benefits patients. However, the incidence rate of hemorrhagic transformation (HT) after IVT has been reported to be as high as 10%-48%, 7 the rate of symptomatic intracranial hemorrhage (sICH) is 2%-7%, 8 and sICH has become an important factor affecting the prognosis of AIS patients after IVT.9,10 Therefore, to better evaluate patients individually, reduce the occurrence of HT, and expand the beneficiary population of IVT, it is urgent to explore the predictors of HT in AIS patients.
It is well known that inflammation has been extensively studied in the pathogenesis of thrombosis and ischemic stroke.11,12 At the same time, increasing evidence shows that inflammation is related to the occurrence of HT, and the inflammatory response caused by reperfusion after IVT can lead to the occurrence of HT. 13 In the inflammatory response, a large number of inflammatory cytokines and oxygen free radicals are released, matrix metalloproteinases are activated to degrade the extracellular matrix, the tight connections between vascular endothelial cells are destroyed, vascular endothelial cells are damages, and the basement membrane is degraded, leading to the destruction of the blood‒brain–barrier (BBB) and thus leading to the occurrence of HT. 13 Platelets and neutrophils, both of which are markers of systemic inflammation, are involved in inflammatory responses, causing damage to blood vessels and brain tissue.14–16 The interaction of neutrophils with platelets can aggravate vascular damage and form complexes that increase the risk of stroke.14,17 As a new inflammatory marker, the neutrophil-platelet ratio (NPR) is more readily available and stable and can reflect the dynamic process of inflammation in stroke. Previous studies have found that patients with a high NPR have an increased risk of developing HT in AIS. 18 However, few studies have reported on the relationship between NPR and the occurrence of HT, sICH, and poor prognosis after IVT. The aim of this study was to investigate whether high NPR levels before IVT are associated with the early occurrence of HT and sICH after IVT.
Materials and Methods
Study Population
Patients with AIS who received IVT in the Department of Neurology, Sichuan Academy of Medical Sciences • Sichuan Provincial People's Hospital from June 2019 to February 2023 were prospectively analyzed. This study was approved by the Ethical Review Board. The inclusion/exclusion criteria of the study were as follows: (1) patients met the diagnostic criteria for AIS confirmed by head CT or MRI and complied with the guidelines for early management of patients with AIS; (2) the time from onset to IVT was less than 6 h; (3) National Institute of Health Stroke Scale (NIHSS) scores were obtained before IVT; (4) patients with neurological impairment due to intracranial tumors or craniocerebral trauma were excluded; (5) patients who received endovascular treatment were excluded; (6) patients with no NPR in the baseline data were excluded; and (7) patients with conditions that may affect blood counts (infection, recent surgery, medications, comorbidities, cancer, collagen vascular disease, COVID-19, etc) were excluded. (8) All patients signed their consent to join the study.
Thrombolytic Therapy
After excluding hemorrhagic stroke through NCCT, all patients were given intravenous thrombolytic therapy. In accordance with domestic and foreign guidelines,19,20 alteplase intravenous thrombolytic therapy was given to patients with AIS within 4.5 h of onset according to the physician's medical advice. The standard dose was 0.9 mg/kg, the maximum dose was 90 mg, 10% of the first dose was administered intravenously within 1 min, and the remaining 90% was administered intravenously and continuously within 60 min. For AIS patients within 4.5-6 h of onset, the urokinase intravenous thrombolytic infusion method was as follows: 1 million to 1.5 million U dissolved in 100 to 200 ml of normal saline as a continuous intravenous infusion for 30 min. Anti-aggregation drugs were not needed within 24 h of treatment. Head CT was reviewed 24 h after thrombolysis.
Data Collection
We recorded baseline characteristics, including demographics (age and sex), classical and nonclassical vascular risk factors (hypertension and diabetes, atrial fibrillation, cholesterol, triglycerides, low-density lipoprotein, coagulation factor function), comorbidities (heart failure, coronary heart disease, cancer, connective tissue disease), past or combination medications (aspirin, clopidogrel, anticoagulants), and other factors. Infarct area (anterior vs posterior circulation), extracranial/intracranial vessel stenosis, and NIHSS score data were collected. Precubital venous blood was taken when the patient was admitted to the emergency department of our hospital. Serum neutrophils, platelets, lymphocytes, hypersensitive C-reactive protein (hs-CRP), uric acid, and platelet counts were collected before IVT. The NPR ratio (neutrophil count [×109/L] × 1000/ platelet count [×109/L] was calculated. Diabetes mellitus was defined as diabetes that had been treated or that was presently diagnosed according to the 1999 World Health Organization criteria (fasting blood glucose of ≥ 7.0 mmol/L, or 2-h oral glucose tolerance test glucose of ≥ 11.1 mmol/L) or a history of hyperglycemia managed by insulin, oral hypoglycemic agents, or diet. We defined hypertension as persistent systolic blood pressure ≥ 140 mm Hg or diastolic blood pressure ≥ 90 mm Hg, a clear history of hypertension on medication, or both.
Outcomes
The main outcomes included the incidence of HT and sICH within 24 h. HT was defined as no bleeding found on the first head CT/MRI after cerebral infarction, and intracranial hemorrhage found on the second head CT/MRI examination. 21 According to the ECASSII study, 22 sICH was defined as clinical aggravation (such as sleepiness, hemiplegia aggravation) or an increase in NIHSS score of ≥4 points. The NIHSS score was judged by two experienced neurology clinicians.
Statistical Methods
SPSS 24.0 statistical software was used for data analysis. Data with a normal distribution are expressed as the mean ± standard deviation (X ± S), and Student's t test was used. Data with a nonnormal distribution are expressed as the median and interquartile range (IQR) [M (Q25, Q75)], and the Mann‒Whitney U test was used. The χ2 test or Fisher's exact test was used to compare categorical variables. Multivariate logistic regression was used to analyze the predictive effect of clinical and laboratory indicators (NPR, age, sex, hypertension, diabetes, atrial fibrillation, uric acid, baseline NIHSS score, smoking, triglycerides, cholesterol, low-density lipoprotein, infarct area, extracranial stenosis, previous medication) on HT and sICH after IVT. P < .05 was considered statistically significant.
Results
General Data of Patients
Between June 2019 and February 2023, a total of 310 patients diagnosed with AIS were treated with rtPA or urokinase within 6 h of stroke onset. Of these, 187 had treatment consisting of alteplase as a thrombolytic, and 60 had urokinase as a thrombolytic. Finally, 247 patients agreed to participate and were included in the study. The mean age was 67.5 ± 12.4 years, and the number of males was 156/247 (63.2%). A total of 69.2% (171/247) of patients had hypertension and 35.2% (87/247) of patients have diabetes. All patients with thrombolysis had normal coagulation function. A total of 21.1%(52/247) of patients smoked, 7.3% (18/247) had coronary heart disease, 19.4%(48/247) had atrial fibrillation, 2% (5/247) had heart failure, 2.4% (6/247) had tumors, and 0.4%(1/247) had connective tissue disease. 96% (237/247) had anterior circulation infarction, 4% (10/247) had posterior circulation infarction, 29.5% (73/247) had intracranial vascular stenosis, 20.6% (51/247) had extracranial vascular stenosis, and 13.4% (33/247) had both intracranial and extracranial vascular stenosis. A total of 36.4% (90/247) had no large vessel stenosis. Before thrombolysis, 29 people took aspirin, 16 took anticoagulants, and seven took clopidogrel. Post-thrombolytic HT occurred in 18.6% (87/247) of patients and post-thrombolytic sICH occurred in 1.2% (13/247) of patients. The median NIHSS score (IQR) was 4 (3-8) at baseline.
Comparisons Between the High and Low NPR Groups with IVT
According to the results of previous studies23 and the Youden index derived from the ROC curve analysis of our cohort, the optimal cut-off for the NPR was assumed to be 35, and all patients were divided into a high NPR group (>35) and a low NPR group (≤35). As shown in Table 1, there were 69 patients in the high NPR group and 178 patients in the low NPR group. There was no significant difference in age, sex, hypertension, diabetes, uric acid, atrial fibrillation, smoking, cholesterol, triglycerides, low-density lipoprotein, infarct area, intracranial and extracranial vascular stenosis, or hs-CRP between the high and low NPR groups (P < .05). The platelet count of the high NPR group was significantly lower than that of the low NPR group (145.5 [123-190.25] vs 204.5 [165.75-238.3], P < .001). Neutrophils in the high NPR group were significantly higher than those in the low NPR group (6.9 [5.07-8.55] vs 4.36 [3.5-5.63], P < .001). The incidence of HT (21 [30.4%]vs 25 [16.3%], P < .05) and sICH (10 [14.5%] vs 3 [1.7%], P < .05) 24 h after IVT in the high NPR group was significantly higher than that in the low NPR group. The baseline NIHSS score of the high NPR group was significantly higher than that of the low NPR group (5 [3-9] vs 4 [2-7.25], P < .05). The lymphocytes in the high NPR group were significantly lower than those in the high NPR group (1.43 [1.0-2.23] vs 1.84 [1.36-2.49], P < .05).
Comparisons Between the High and Low NPR Groups.
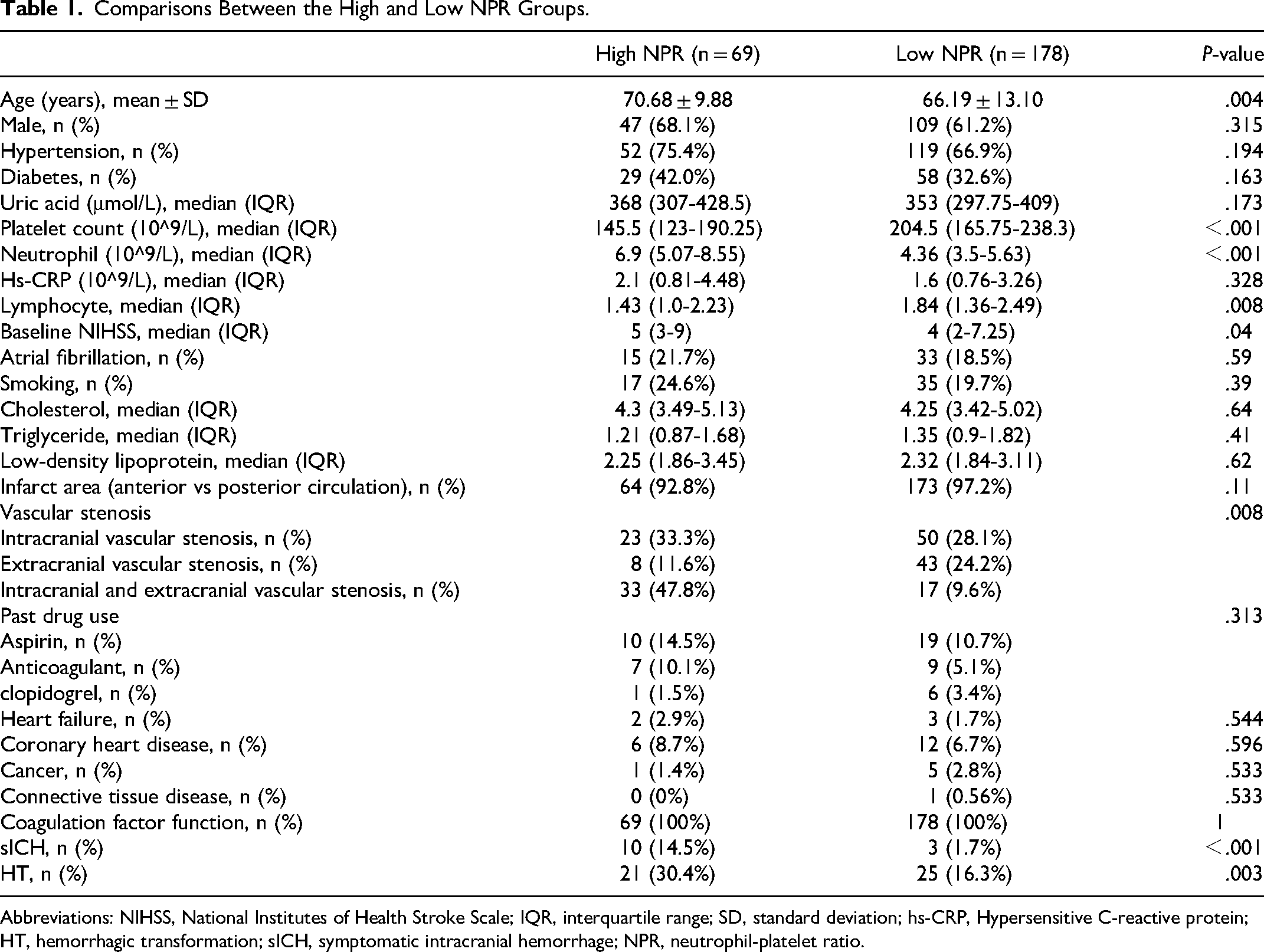
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; IQR, interquartile range; SD, standard deviation; hs-CRP, Hypersensitive C-reactive protein; HT, hemorrhagic transformation; sICH, symptomatic intracranial hemorrhage; NPR, neutrophil-platelet ratio.
Multivariate Logistic Regression Analysis of Predictors for HT
HT is considered to be the dependent variable. Age, sex, hypertension, diabetes, atrial fibrillation, uric acid, baseline NIHSS score, smoking, triglycerides, cholesterol, low-density lipoprotein, infarct area, extracranial stenosis, previous medication (aspirin, clopidogrel, anticoagulants), and NPR were considered independent variables. As shown in Table 2, a high NPR was an independent risk factor for HT (OR = 3.236, 95% CI: 1.481-7.068, P = .003).
Multivariate Logistic Regression Analysis of Predictors for HT.
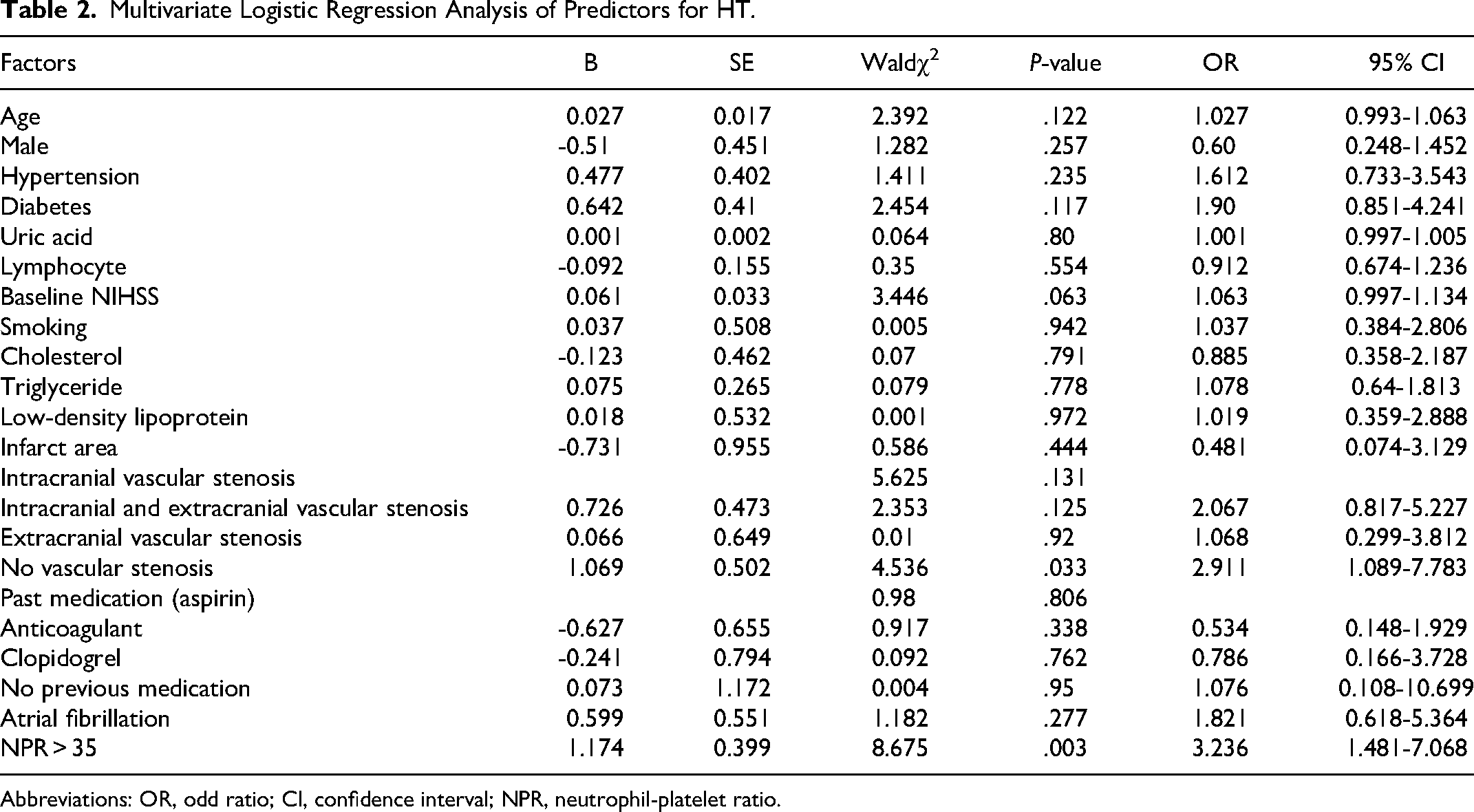
Abbreviations: OR, odd ratio; CI, confidence interval; NPR, neutrophil-platelet ratio.
Multivariate Logistic Regression Analysis of Predictors for sICH
SICH is considered to be the dependent variable. Age, sex, hypertension, diabetes, uric acid, atrial fibrillation, baseline NIHSS score, smoking, triglycerides, cholesterol, low-density lipoprotein, infarct area, extracranial stenosis, previous medication (aspirin, clopidogrel, anticoagulants), and NPR were considered independent variables. As shown in Table 3, a high NPR was an independent risk factor for HT (OR = 13.644, 95% CI: 2.392-77.83, P = .003).
Multivariate Logistic Regression Analysis of Predictors for sICH.
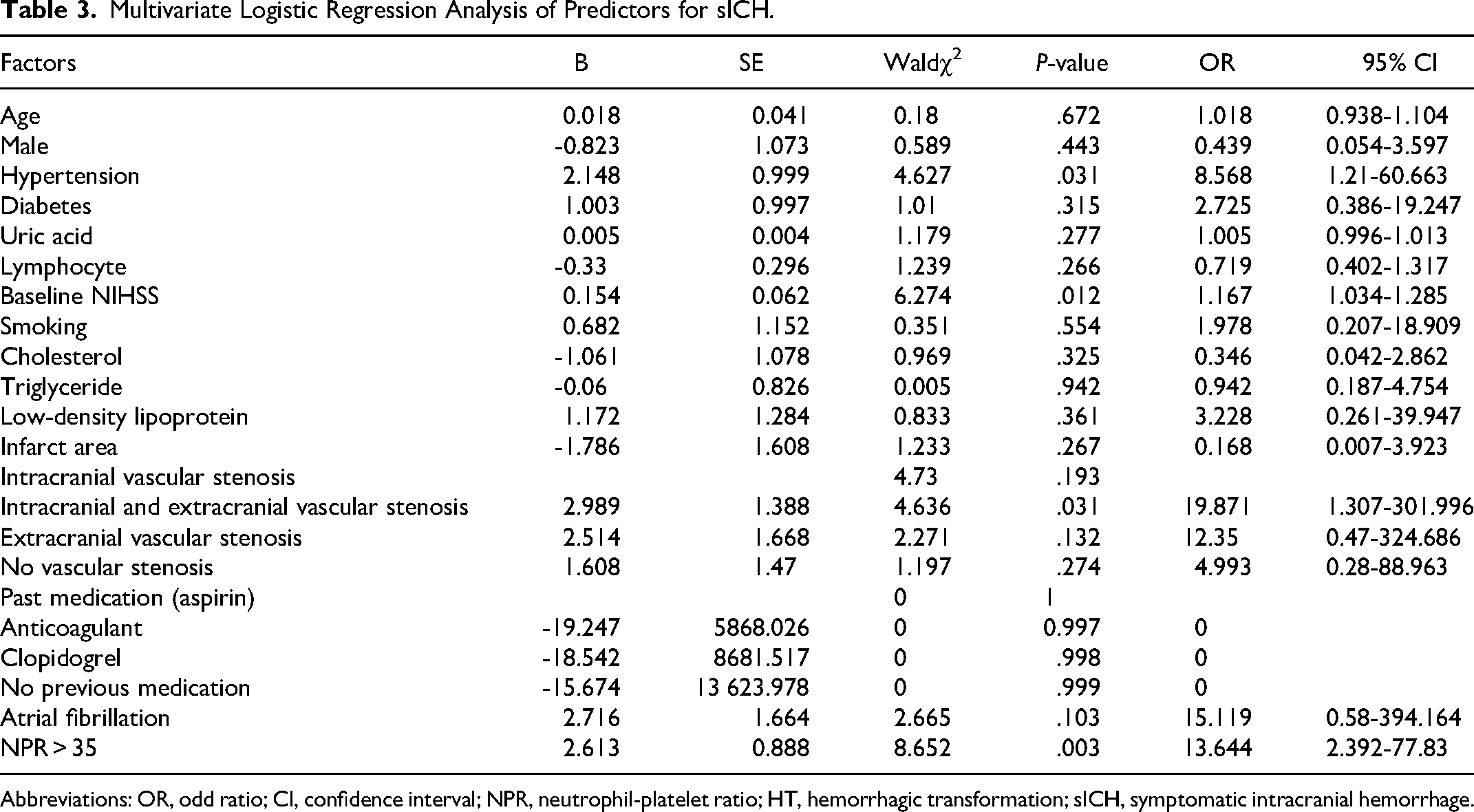
Abbreviations: OR, odd ratio; CI, confidence interval; NPR, neutrophil-platelet ratio; HT, hemorrhagic transformation; sICH, symptomatic intracranial hemorrhage.
Discussion
It has been noted in domestic and foreign guidelines19,20 that IVT is one of the most effective treatments for AIS patients. However, some patients still develop HT and sICH after IVT, leading to poor prognosis. In our study, the incidence of HT was 18.6% and the incidence of sICH was 1.2%. HT and sICH after IVT were significantly higher in the high NPR (>35) group than in the low NPR (≤35) group. Multivariate logistic regression analysis showed that a high NPR (>35) was significantly associated with HT and sICH after IVT. Our results suggest that a high NPR (>35) may be a new predictor of HT and sICH after IVT and has guiding significance for the treatment of patients with AIS.
Neutrophils are known to be involved in the body's response to infection and inflammation. When stroke occurs, neutrophils are the first to infiltrate and participate in the inflammatory response. 21 Studies have found that MMP-9 produced by neutrophils can cause the destruction of the BBB, aggravate brain tissue damage, and lead to HT. 24 In addition to neutrophils, another blood component is platelets. Platelets are a double-edged sword and play many roles in the process of stroke. Platelets have a hemostatic function and help protect the integrity of the BBB. 25 However, platelets also have proinflammatory effects. When stroke occurs, inflammatory cells can be recruited by platelets and interact with platelets, resulting in vascular inflammation and further brain tissue damage.15,26 The inflammatory response of the body usually results in a reduction in platelets, which may be related to immunity, continuous activation of platelets, and thrombosis. 27 The decrease in platelets and the increase in neutrophils caused by inflammation both cause an increase in the NPR. Our research also found this phenomenon. In our study, neutrophils in the high NPR group were significantly higher than those in the low NPR group, while platelets in the high NPR group were significantly lower than those in the NPR group.
The pathophysiological mechanism of HT after IVT is very complicated. At present, it is believed that severe ischemia and hypoxia occur in the brain tissue of patients with AIS, which stimulates the body to produce an inflammatory response, resulting in the destruction of the BBB and the occurrence of HT.28,29 Thrombolytic agents can promote the cleavage of fibrinogen to fibrin, leading to clotting disorders and thus the occurrence of HT. 30 After IVT, a series of inflammatory cascade reactions occur again in the process of restoring blood perfusion, leading to further destruction of the BBB and thus the occurrence of HT. 13 At present, many people are studying biomarkers related to HT. Xing et al31 showed that leukocyte increase was an independent predictor of HT after thrombolysis, and the leukocyte count in patients with HT was significantly higher than that in patients without HT. In recent years, it has also been found 32 that a higher neutrophil to lymphocyte ratio may be independently associated with the occurrence of HT and 3-month mortality in patients after IVT and can be used as a predictor of HT after IVT. The study of Tsai et al 33 showed that the level of intervascular endothelial cell adhesion molecules in the serum of patients with AIS after thrombolysis was significantly increased, suggesting that it was also correlated with HT after thrombolysis and could be used as a predictor of HT after thrombolysis. However, these indicators are not widely used in clinical practice. The NPR is a new inflammatory marker that represents the body's inflammatory response. The advantage of the NPR is that it may be more stable than individual serum markers and is more readily available clinically. It reflects the pathophysiological process of inflammation and thrombosis in stroke. Therefore, we speculated that a high NPR predicted more severe BBB destruction, leading to a higher risk of bleeding after thrombolysis.
Clinically, the NPR has been studied in other diseases. For example, many diseases in the cardiovascular system are associated with the NPR.34,35 Currently, the NPR has been tested in AIS. This study found that the NPR is a prognostic indicator of the 90-day prognosis of AIS. A high NPR is associated with an increased risk of HT in patients with AIS and an increased risk of hematoma dilatation in patients with cerebral hemorrhage.18,36,37 However, no one has studied whether the risk of HT after IVT is related. Our study showed that the incidence of HT and sICH in the high NPR group was significantly higher than that in the low NPR group. In multivariate logistic regression analysis, NPR was independently correlated with HT (OR = 3.236, 95% CI: 1.481-7.068, P = .003). This suggests that the high NPR group (>35) may have a 3.236-fold increased risk of HT after IVT compared to the low NPR group before IVT. The NPR was also independently related to sICH (OR = 13.644, 95% CI: 2.392-77.83, P = .003). This suggests that the high NPR group (>35) before thrombolysis may have a 13.644-fold increased risk of sICH after thrombolysis compared to the low NPR group.
The present study has some limitations. First, we only analyzed the NPR before IVT. The relationship between the dynamic changes in the NPR and HT before and after IVT should be studied. Second, the sample size was relatively small, which may have led to bias in the statistical results. Third, the parameters collected in this study were limited, and not all classical and nonclassical risk factors for AIS were collected.
In conclusion, this study suggests that a high NPR (>35) before IVT may be a predictor of HT after IVT in AIS patients. These findings may help clinicians identify high-risk stroke patients with HT after IVT and provide some assistance to clinicians in clinical decision-making before thrombolysis in AIS patients.
Footnotes
Acknowledgements
Throughout the writing of this study, I have received a great deal of support and assistance. I would first like to thank ZCX,YNW and LBH for their suggestions on the design of the experiment. Second, I would like to thank ZS and JLJ for collecting the data. ZQ and WLR explained the data, and WJH helped us analyse a large amount of data over time. Finally, I would like to thank the Sichuan Natural Science Foundation (Grant No. 2023NSFSC0582) and Sichuan Medical Research Project Plan (Grant No. S22075) for financial support.
Authors’ Contribution
YNW, ZCX and LBH were responsible for the conception and design of the study. WJH analyzed the data collected by JLJ and ZS. ZQ and WLR interpreted the data. CXD drafted the manuscript. All authors revised and approved the final manuscript and are accountable for the accuracy and integrity of the work.
Availability of Data and Materials
The datasets in this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sichuan Medical Research Project Plan, Natural Science Foundation of Sichuan Province, (grant number Grant No. S22075, Grant No. 2023NSFSC0582).