
Abstract
Background
Stroke significantly impacts global health, and IV thrombolytics such as tenecteplase and alteplase are time sensitive. While they show promise beyond 4.5 h, evidence is inconclusive. This meta-analysis assesses IVT's efficacy and safety past 4.5 h.
Methods
PubMed, Cochrane Central, and ScienceDirect were searched till August 2025. The risk ratios (RR) were pooled along with 95% confidence intervals under the random effect model using the Review Manager version 5.4.1.
Results
Thirteen randomized trials involving 3602 patients were analyzed. Compared to the control group, IVT significantly improved the rates of excellent (RR = 1.22; 95%CI: [1.13, 1.31];p < 0.00001; I2 = 0%) and good (RR = 1.11; 95%CI: [1.06, 1.18];p < 0.0001; I2 = 0%) functional outcomes. However, the risk of symptomatic (RR = 2.28; 95%CI:[1.35, 3.85];p = 0.002; I2 = 0%) and any (RR = 1.22; 95%CI:[1.01, 1.46];p = 0.04; I2 = 13%) intracranial hemorrhage (ICH) was also higher with IVT; mortality rates, however, showed no significant difference (RR = 1.10; 95%CI:[0.89, 1.36];p = 0.35). TNK at 0.25 mg/kg did not improve functional outcomes or increase the risk of ICH. Similarly, low-dose 0.60 mg/kg alteplase did not significantly enhance functional outcomes or raise the risk of ICH, while alteplase at 0.90 mg/kg showed results consistent with the overall IVT group.
Conclusion
IVT administered beyond the 4.5-h window in acute ischemic stroke significantly improved excellent and good functional outcomes. Although the use of IVT was associated with a higher risk of symptomatic and any ICH, the mortality rates remained comparable. Further high-quality randomized trials are necessary to confirm and reinforce these results.
Introduction
Strokes contribute highly to death and disability all over the world. It is also one of the leading causes of death globally. 1 Stroke refers to the sudden onset of functional neurological disturbances due to some form of ischemia or a hemorrhage, with a duration persisting for at least 24 h or until death occurs. 2 It is a complex condition with symptoms arising in sensory, cognitive, perceptual, behavioral, and motor domains. 3 The number of stroke victims has increased significantly in the last decade and a half. As of now, everyone has a 25% chance of suffering from a stroke in their lifetime. 3 The chance of stroke in individuals aged 55 and above is 20% for females and 16.6% for males. 4
Intravenous thrombolysis (IVT) is superior to medical treatment, as evident by multiple trials. 5 Thus, the mainstay treatment for ischemic stroke is thrombolysis via alteplase. 5 Tenecteplase (TNK) is another thrombolytic agent that has been studied as an alternative, with evidence suggesting that it is at least as effective as alteplase and perhaps more effective in lysing large-vessel clots. 6 However, these thrombolytics must be administered within the time window of 4.5 h or less. 7 Multiple pairwise and network meta-analyses have assessed the efficacy and safety of IVT in ischemic stroke within the 4.5-h window.8–13 Endovascular therapy (EVT) with mechanical thrombectomy (MT) is not limited by a strict time window, and several meta-analyses have assessed the effectiveness and safety of EVT across different ischemic conditions stroke.14–16 EVT has shown favorable results even up to 24 h from stroke onset. 17 Investigation on whether thrombectomy is beneficial in patients with distal vessel occlusions or patients with large ischemic core volume proximal vessel disease is still ongoing. 5
IVT is better than MT mainly due to its broader applicability and rapid administration. 18 However, only very few patients can meet the 4.5-h time window for IVT. 19 Recent studies in this regard show conflicting evidence. In an individual patient-level meta-analysis of four trials that selected patients for IV alteplase based on either DWI-FLAIR or perfusion mismatch imaging, it was found that alteplase infusion improved functional outcomes at 90 days, as compared to standard medical care. 20 The two newer agents, TNK and reteplase, may also offer potential advantages in comparison with alteplase. 21 TNK had indeed good functional outcomes in large-vessel occlusion (LVO) patients treated in the extended time window versus standard care in the TRACE-III trial. 21 Contrary to this, the TIMELESS trial found no difference with TNK in functional outcomes among patients with LVO. 22 In this trial, the median time from TNK treatment to thrombectomy was quite low, which might have impacted the outcomes. 22 Hence, while newer thrombolytics do seem to offer promise, their benefit in terms of the extended windows and diverse clinical scenarios still needs validation 23
The therapeutic window for IVT in acute ischemic stroke (AIS) is shifting, with new data emerging during that time to possibly consider applications at more than 4.5 h through advanced imaging. The newer agents, like TNK and reteplase, have contradicting evidence in their favor. Such differences demand robust evidence, thereby making this systematic review and meta-analysis imperative to understanding and informing the future utilization of these agents in the extended window. This systematic review aimed to evaluate and compare the efficacy and safety of IVT agents administered beyond 4.5 h after stroke onset.
Methods
We conducted this systematic review and meta-analysis in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 2020. 24 This review followed the guidelines by the Cochrane Handbook for Systematic Reviews of Interventions. 25 The protocol of this review was registered on PROSPERO under the ID: CRD420251111786.
Data Sources and Search Strategy
Two independent authors (D.G. and M.A.) conducted an electronic search on databases including PubMed, Cochrane Central, and ScienceDirect from inception to August 2025, using the following keywords and their associated MeSH terms: “Ischemic stroke,” “thrombolysis,” “tenecteplase,” “alteplase,” and “extended time window.” Additionally, we thoroughly reviewed the reference lists of all relevant articles to identify any studies that may have been overlooked during the initial search.
Study Selection and Inclusion Criteria
All retrieved articles were exported to EndNote Reference Library X7 software, where they underwent a screening process to remove duplicates. The remaining articles were first shortlisted by primary screening based on their titles and abstracts, followed by a secondary screening including a full-text review to ensure all included studies met the predefined eligibility criteria. This was performed by two independent authors (S.K. and F.S.). A Third author (M.H.W.) was brought in to resolve any conflicts. The study selection process is depicted in the PRISMA flowchart (Figure 1).

PRISMA flowchart of the study selection process.
Studies were included if they met the following criteria: 1) The study design was a randomized controlled trial (RCT) that included participants aged 18 years diagnosed with AIS, 2) The intervention group received IVT, either 0.25 mg/kg TNK, 0.90 mg/kg alteplase or low-dose 0.60 mg/kg alteplase, and 4) The study reported at least one primary outcome relevant to our analysis.
Our exclusion criteria included 1) Studies with non-human or animal subjects, 2) Study design other than RCTs, including editorials, reviews, case reports, letters, surveys, commentaries, and non-comparative studies.
Data Extraction and Outcome Definition
Two independent reviewers (Z.F. and M.W.A.) extracted the baseline characteristics, primary outcomes, and secondary outcomes from the selected studies. All data was entered on Excel sheets. The baseline characteristics extracted were study ID, study design, location, sample size, description of the intervention and control arms, imaging used, follow-up, age, gender, onset of stroke, baseline modified Rankin Scale (mRS), National Institute of Health Stroke Scale (NIHSS) score, and treatment time window. All outcomes were dichotomous. The endpoints extracted were 1) Excellent functional outcome at 90 days, 2) Good functional outcome at 90 days, 3) All-cause mortality within 90 days, 4) Symptomatic Intracranial hemorrhage (sICH), and 5) Any ICH.
The functional outcomes were determined using the mRS, a scale used to evaluate functional disability after a stroke, with higher scores indicating greater disability. An excellent functional outcome is defined as an mRS of 0-1. A good functional outcome is defined as an mRS of 0-2.
Bias Assessment
All included RCTs underwent quality assessment using the Cochrane Risk of Bias (RoB 2.0) tool. 26 This was performed by two reviewers (R.A. and P.K.T.). Any discrepancies were resolved by a third reviewer (M.H.W.). RoB 2.0 has five domains: bias from randomization, deviations, missing data, outcome measurement, and selection of reported results. Publication bias was assessed visually with funnel plots. To determine evidence certainty, we performed the GRADE assessment of all the extracted outcomes through the GRADEpro GDT. 27
Statistical Analysis
The statistical analysis was conducted on Review Manager (RevMan, Version 5.4.1, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). All results were pooled using the Mantel-Haenszel random effects model and analyzed as risk ratios (RR) with 95% confidence intervals (CIs). Statistical heterogeneity was assessed using Cochrane Q tests and Higgins’ I2 statistics. 28 Outcomes with an I2 value below 50% were considered low heterogeneity. All outcomes with a p-value of less than 0.05 were reported as statistically significant. These results are shown using forest plots. We performed a subgroup analysis for all reported outcomes based on the types and dosages of IVT used (0.90 mg/kg alteplase, 0.60 mg/kg (low-dose) alteplase, and 0.25 mg/kg TNK), post-IVT usage of EVT, and imaging technique (Magnetic resonance imaging, diffusion-weighted imaging–fluid-attenuated inversion recovery (MRI DWI-FLAIR) mismatch, MRI or Computed tomography (CT) perfusion, and MRI and Noncontract CT (NCCT)). To check for publication bias, we used funnel plots.
Results
Study Selection and Characteristics
A search across various databases (PubMed: 737, Cochrane Central: 54, ScienceDirect: 339) identified 1130 articles. After removing 282 duplicates, 848 articles remained and were screened by title and abstract, resulting in 112 articles. These studies were further evaluated through a full-text screening process, resulting in the inclusion of 13 studies7,21,22,29–38 in this systematic review and meta-analysis. The selection process is detailed in the PRISMA flow diagram shown in Figure 1.
Thirteen RCTs7,21,22,29–38 pooling 3602 patients with publication years ranging from 2014 to 2025 were included in this meta-analysis. Six studies were exclusively conducted in China, one in Japan, and the remaining studies originated from various other countries. Six studies reported using 0.25 mg/kg TNK as IVT, while six others used the standard 0.90 mg/kg Alteplase for IVT. Only one study from Japan employed a lower dose of 0.60 mg/kg Alteplase as IVT. Most studies have a baseline mRS score of 0-1, except 4 that have a baseline mRS score of 0-2. The median baseline NIHSS score ranged from 3 to 12. The baseline characteristics of the included studies and patients are provided in Table 1a and b.
Baseline Characteristics of the Included Studies.

NOTE: RCT: Randomized controlled trial; MRI: Magnetic resonance imaging; NCCT: Non-Contrast Computed Tomography; CT: Computed Tomography; *: Standard medical care was defined as antiplatelets, statins, blood pressure and glucose management, and general supportive care according to European or national guidelines for acute cases stroke; **: The standard treatment group received antiplatelet therapy and other treatments following the Chinese Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke 2018; ***: No thrombectomy occurred before randomization. Rescue thrombectomy was performed in four patients in the IVT group and in five patients in the control group; NBP: Dl-3-n-Butylphthalide.
Baseline Characteristics of the Included Patients.

Note: mRS: Modified rankin scale; NIHSS: National Institutes of Health Stroke Scale.
Quality Assessment
The quality assessment of the included RCTs was done through the Cochrane RoB 2.0 tool. All the included RCTs have a low risk of bias, except for four, which raised some concerns, mainly due to deviations from the intended intervention (Figure 2).

The cochrane risk of bias 2.0 tool traffic light plot.
Outcome
The meta-analysis summary is presented in Table 2, while the GRADE summary of findings is shown in Table 3.
Summary of the Meta-Analysis.

Note: ICH: Intracranial hemorrhage; sICH: Symptomatic intracranial hemorrhage; TNK: Tenecteplase; IVT: Intravenous thrombolysis; RR: Risk ratio; CI: Confidence interval; df: degree of freedom.
GRADE Summary of Findings.
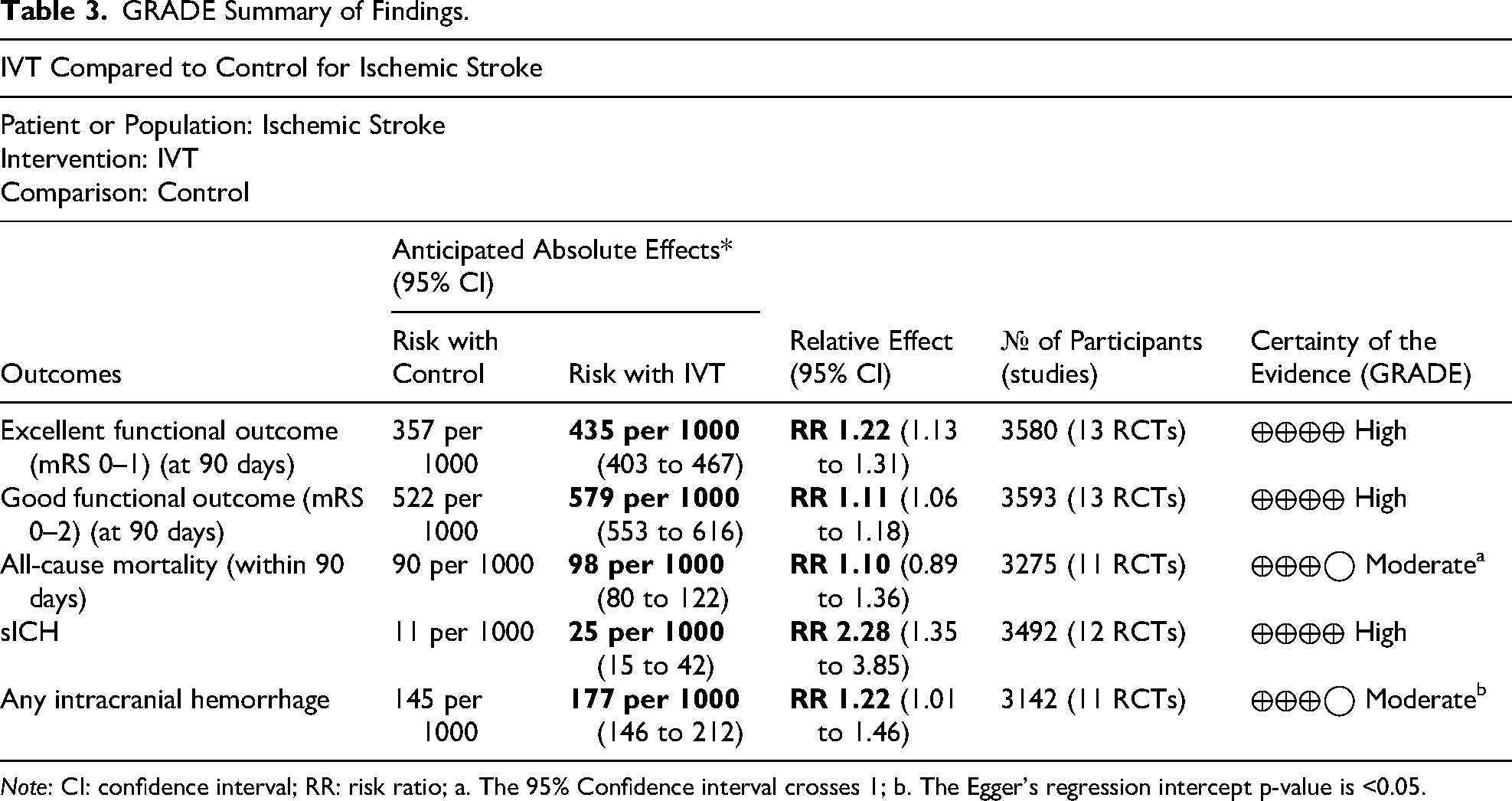
Note: CI: confidence interval; RR: risk ratio; a. The 95% Confidence interval crosses 1; b. The Egger's regression intercept p-value is <0.05.
Excellent Functional Outcome
Thirteen studies pooling a total of 3508 patients (1803 IVT vs 1777 Control) reported this outcome. The pooled evidence indicated a statistically significant increase in the likelihood of achieving excellent functional outcome with IVT as compared to control (RR = 1.22; 95% CI: 1.13 to 1.31; P < 0.00001; I2= 0%) (Figure 3).

Excellent functional outcome forest plot.
Good Functional Outcome
Thirteen studies pooling a total of 3593 patients (1811 IVT vs 1782 Control) reported good functional outcome. The pooled RR suggested a significant trend toward improved good functional outcome at 90 days with IVT when compared to control (RR = 1.11; 95% CI: 1.06 to 1.18; P < 0.0001; I2= 0%) (Figure 4).

Good functional outcome forest plot.
All-Cause Mortality
Eleven studies pooling a total of 3275 patients (1655 IVT vs 1620 Control) reported this outcome. Overall, no statistically significant difference was observed between IVT and control groups (RR = 1.10; 95% CI: 0.89 to 1.36; P = 0.35; I2= 0%) (Figure 5).

All-cause mortality at 90 days forest plot.
Symptomatic Intracranial Hemorrhage
Twelve studies pooling a total of 3492 patients (1766 IVT vs 1726 Control) reported this endpoint. The pooled effect size showed a significantly increased risk of sICH with IVT compared to control (RR = 2.28; 95% CI: 1.35 to 3.85; P = 0.002; I2 = 0%) (Figure 6).

Symptomatic intracranial hemorrhage forest plot.
Any Intracranial Hemorrhage
Eleven studies pooling a total of 3142 patients (1582 IVT vs 1560 Control) reported this endpoint. Overall, IVT significantly increased the risk of any ICH compared to controls (RR = 1.22; 95% CI: 1.01-1.46; P = 0.04; I2 = 13%) (Figure 7).
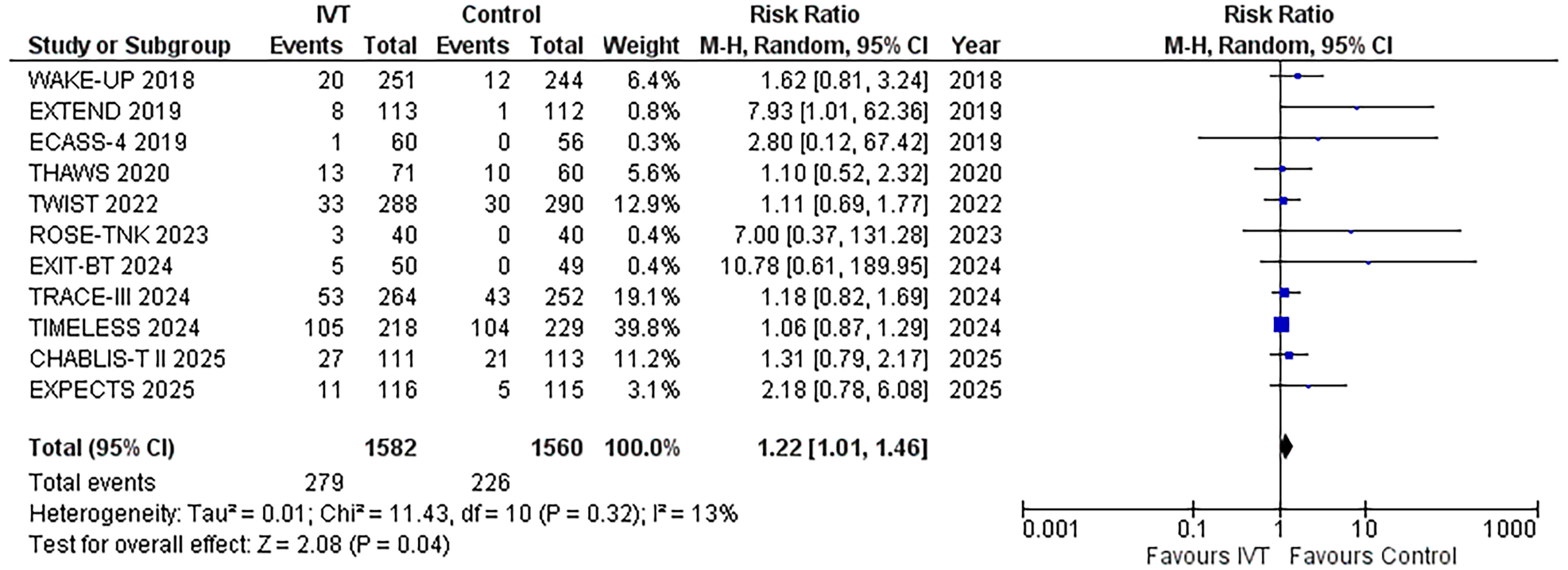
Any intracranial hemorrhage forest plot.
Subgroup Analysis
We conducted a subgroup analysis for all reported outcomes, considering the types and dosages of IVT used (0.90 mg/kg alteplase, 0.60 mg/kg low-dose alteplase, and 0.25 mg/kg TNK), along with EVT usage post-IVT, and imaging technique (MRI DWI-FLAIR mismatch, MRI or CT perfusion, and MRI and NCCT).
When subgrouping by IVT type and dosage, results were consistent across endpoints (Supplemental Figure 3), except that 0.60 mg/kg low-dose alteplase did not significantly improve excellent functional outcomes (Supplemental Figure 1). Neither TNK 0.25 mg/kg nor low-dose alteplase 0.60 mg/kg showed a significant increase in good functional outcomes (Supplemental Figure 2). Additionally, TNK 0.25 mg/kg and low-dose alteplase 0.60 mg/kg did not raise the risk of sICH (Supplemental Figure 4) or any ICH (Supplemental Figure 5).
In the subgroup analysis comparing patients who received EVT after IVT with those who did not, the results were generally consistent across outcomes (Supplemental Figure 6 and Supplemental Figure 8). However, the pooled result for good functional outcome lost statistical significance in the EVT subgroup (Supplemental Figure 7), as did the pooled result for sICH (Supplemental Figure 9). Additionally, the pooled results for any ICH became insignificant in the EVT subgroup (Supplemental Figure 10).
When subgrouping by imaging technique, the results remained consistent across all endpoints (Supplementary Figures 11 and 13), except for the pooled results for good functional outcome. These became insignificant in the MRI DIW-FLAIR mismatch and MRI or CT perfusion imaging subgroups (Supplemental Figure 12). Similarly, the significant pooled effect sizes for sICH (Supplemental Figure 14) lost significance in the MRI DIW-FLAIR mismatch, and MRI or NCCT imaging subgroups. For any ICH (Supplemental Figure 15), the loss of significance occurred in the MRI DIW-FLAIR mismatch, MRI or CT perfusion, and MRI or NCCT imaging subgroups.
Publication Bias
Visual analysis of funnel plots indicated no notable publication bias overall. The funnel plots of the respective endpoints are shown in Supplemental Figures 16-20.
GRADE Assessment
All endpoints, such as excellent functional outcome, good functional outcome, and sICH, demonstrated high certainty of evidence. In contrast, all-cause mortality and any ICH showed moderate certainty of evidence.
Discussion
In this meta-analysis, we assessed the efficacy and safety of IVT agents administered beyond 4.5 h after stroke onset. Our findings suggest that extended-window thrombolysis may improve functional outcomes, including excellent and good functional outcomes at 90 days. However, these benefits were accompanied by a significantly increased risk of sICH and any ICH. The rate of 90-day mortality was comparable.
The findings of this meta-analysis are generally consistent with those of previous reviews that reported a benefit of IVT administered beyond the conventional 4.5-h window.22,23 The inclusion of newer trials, such as EXPECTS 2025, CHABLIS-T II, TIMELESS, and TWIST, adds important data on posterior circulation strokes and the use of non-contrast CT in patient selection, which were underrepresented or absent in earlier studies.22,30,35,38 While some studies, including EXPECTS 2025, demonstrated a clear benefit in functional outcomes, others reported no statistically significant effects,34,36 highlighting variability in treatment response across different patient populations and trial designs. This variability may be attributed to differences in imaging-based inclusion criteria (eg, perfusion imaging in TIMELESS vs non-contrast CT in TWIST), baseline stroke severity, and the use of different IVT agents and dosages.22,35 For example, alteplase was associated with a significant improvement in good functional outcomes,23,39 whereas TNK did not show a statistically significant benefit.35,40 Additionally, the presence of co-interventions such as thrombectomy, as seen in trials like TIMELESS, may have masked the benefits of IV thrombolytics in some patient groups. 22
The safety profile observed in this meta-analysis aligns with previous findings, showing a consistent increase in sICH among patients receiving IV thrombolysis beyond the 4.5-h window.39,41 A significant increase in both symptomatic and any ICH was observed in the thrombolysis group. Despite these bleeding complications, 90-day mortality was numerically higher but not statistically significant. This reflects the known hemorrhagic risks associated with thrombolytic agents, but the lack of a significant increase in mortality may be attributed to milder baseline stroke severity in some trials, improved management of complications, and the use of imaging-based selection criteria that help identify patients most likely to benefit while minimizing harm. 23
These results have important implications for clinical practice. Extended-window thrombolysis beyond the 4.5-h may offer functional benefits in patients carefully selected through imaging-based assessments of tissue viability rather than strict time cutoffs.22,23 This evolving paradigm could expand eligibility for IVT, especially in settings where mechanical thrombectomy (MT) might not be readily available or where TNK may offer advantages over alteplase. 42 However, the associated bleeding risks highlight the importance of precise patient selection and clinical judgment. The variability of findings across studies further underscores the need to identify which subgroups are most likely to benefit from treatment while minimizing potential harm. Future studies should aim to clarify the comparative roles of TNK and alteplase, optimize thrombolytic dosing, and evaluate outcomes across broader populations and healthcare settings, including low-resource settings where access to advanced imaging and MT is limited. Moreover, efforts should focus on standardizing imaging criteria and refining inclusion protocols to ensure consistent and safe application of extended-window thrombolysis.
This study has some limitations that must be acknowledged. There was variability in the trial protocols and inclusion criteria across the studies, including differences in thrombolytic agents, dosages, thrombectomy use, and imaging modalities. These factors contributed to clinical heterogeneity, limiting the generalizability of the findings. Therefore, future research is needed to evaluate the safety and effectiveness of IVT in AIS patients outside the 4.5-h window within a more generalized patient population. The generalizability of our meta-analysis might be limited because it primarily includes trials conducted in regions where EVT was not available in the recommended time frame. Outcomes can vary between patients who receive EVT after IVT and those who receive only IVT. Future research should include patients who undergo both EVT and IVT to better evaluate their combined safety and improve the applicability of the results. Another potential limitation of this meta-analysis is the selection of patients based on imaging criteria, which may have excluded those with very mild or very severe strokes, while potentially including patients with stroke mimics. The lack of standardized post-stroke care across the trials may also have influenced the 90-day outcomes. The included trials differed in their choice of control groups, with some studies using a placebo and others using standard medical therapies as the control. In addition, the small sample size of the 0.60 mg/kg low-dose Alteplase subgroup decreases the statistical power of the pooled findings for this subgroup. Consequently, the limited sample size and regional variations in treatment practices may influence the applicability of these results outside Asia. While we used both tenecteplase and alteplase to evaluate the overall efficacy and safety of IVT beyond the 4.5-h window, we recognize that the absence of an alteplase arm in some trials limits our ability to draw conclusions specifically for alteplase.
Conclusion
This meta-analysis offers updated evidence supporting the potential effectiveness of IVT beyond the standard 4.5-h window. Administering IVT after this period in AIS significantly increased the excellent and good functional outcomes. Although IVT use is linked to an increased risk of symptomatic and any ICH, mortality rates remain comparable. While properly selected patients may experience better functional outcomes, the elevated risk of ICH underscores the importance of careful patient selection and treatment. More rigorous research is required to inform clinical decisions and improve outcomes for patients presenting with AIS beyond the 4.5-h window.
Supplemental Material
sj-docx-1-cat-10.1177_10760296251414133 - Supplemental material for Efficacy and Safety of Intravenous Thrombolytics in Ischemic Stroke Beyond the 4.5-Hour Time Window: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296251414133 for Efficacy and Safety of Intravenous Thrombolytics in Ischemic Stroke Beyond the 4.5-Hour Time Window: A Systematic Review and Meta-Analysis by Muhammad Hassan Waseem, Zain ul Abideen, Dua Ghori, Faizan Shahzad, Shamama Kaleem, Misha Ahmed, Muhammad Wajih Ansari, Rowaid Ahmad, Zara Fahim, Pawan Kumar Thada and Brandon Lucke-Wold in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Ethical Approval
Not applicable
Patient Consent
Not applicable
Authors’ Contributions CRediT Roles
Study concept and design: MHW and ZUA; acquisition of data: ZUA, DG, and MA; analysis and interpretation of data: ZUA and SK; drafting of the manuscript: RA, ZF, WA, and PKT; critical revision of the manuscript: MHW and BLW
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data will be made available upon reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.