
Abstract
Objective
To systematically assess the risk prediction models for preoperative deep vein thrombosis in older patients with hip fractures.
Method
We searched four databases for literature through November 17, 2023. We included patients aged ≥60 with hip fractures and considered English-language case-control or cohort studies that focused on developing and/or validating risk prediction models for DVT in this population. Excluded were studies that solely analyzed risk factors without constructing a prediction model, had fewer than 2 predictive variables, or were not available in full-text or were duplicate publications. The Predictive Model Bias Risk Assessment tool was utilized to evaluate risk of bias. The area under the curve (AUC) values were meta-analyzed using R Studio software. The I2 index and Cochrane q test were employed to assess heterogeneity. Additionally, sensitivity analysis was performed by systematically removing individual studies to explore the sources of heterogeneity.
Results
A total of 1880 studies were gathered. Out of these, seven studies were included, encompassing 8 models. The most commonly utilized factors in the models were D-dimer and the time from injury to admission. The pooled AUC value for the validation of 8 models was 0.84 (95% confidence interval: 0.80-0.87), indicating robust model performance.
Conclusion
Current risk prediction models for preoperative DVT in elderly hip fracture patients are still in the developmental phase. Future research should focus on developing new models with larger sample sizes, robust study designs, and multicenter external validation.
Introduction
Hip fractures represent a prevalent orthopedic trauma in the elderly. 1 With the global population aging, the incidence of hip fractures in this demographic is steadily increasing. 2 Projections suggest that the global number of hip fractures will surge from 1.26 million in 1990 to 4.5 million in 2050, indicating a pressing global public health concern. 3 Prior to hip fracture surgery, patients often encounter deep vein thrombosis (DVT) as a complication. 4 According to relevant studies,5,6 the prevalence of DVT following hip trauma ranges from 11.1% to 32.8%. DVT not only contributes to pulmonary embolism (PE) and post-thrombotic syndrome (PTS), but is also significantly associated with the occurrence, recurrence risk, and mortality of pulmonary embolism. 7 Therefore, it is essential to accurately pinpoint DVT risk factors, promptly identify high-risk groups for DVT formation, and actively address reversible factors. Studies on DVT preceding hip fracture surgery in elderly individuals have been undertaken, and risk prediction models based on various risk factors have been developed.8,9 However, no comprehensive assessment of these models has been conducted, and the effectiveness of each model remains uncertain.
The study systematically analyzes and evaluates the risk prediction model for deep vein thrombosis in older patients with hip fractures. Its aim is to provide a reference for the construction of future models and a basis for the model's clinical application.
Methods
This study has been registered in PROSPERO with the registration number of CRD42024501481.
Search Strategy
A computer-based search was performed on PubMed, Web of Science, Embase, and Scopus databases to retrieve research on risk prediction models for deep vein thrombosis in elderly hip fracture patients. The search covered the period from the inception of the databases until December 3, 2023, and was limited to English language publications. The search criteria were developed by combining subject terms and free-text terms, encompassing keywords such as “hip fracture,” “femoral neck fracture,” “trochanteric fracture,” “thrombosis,” “embolism,” “thrombus,” “predict,” “identify,” and “model.” (Table S1)
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) Inclusion criteria: Patients aged 60 years or older with hip fractures, including femoral neck, femoral head, intertrochanteric/subtrochanteric, and trochanteric fractures, who underwent hip joint surgery, including both hip replacement and internal fixation. (2) Scope of research: Research focused on the creation and/or testing of risk prediction models for deep vein thrombosis in older patients with hip fractures. (3) Study design: Case-control studies and cohort studies. (4) Language: Publications in the English language.
Exclusion Criteria
(1) Studies that only examined risk factors without developing predictive models. (2) Paper written in a language other than English. (3) Models with less than 2 predictive variables. (4) Complete text not accessible. (5) Repetitive publication
Literature Screening and Data Extraction
Fangfang Deng and Kuankuan Xu, two researchers, independently conducted literature screening, data extraction, and cross-verification. In cases of discrepancies, Kun Zhang, Fangfang Deng, and Kuankuan Xu, all three authors, held discussions and made decisions jointly. EndNote software was used to eliminate duplicate publications. Titles and abstracts of the articles were initially reviewed to exclude obviously irrelevant articles. Subsequently, full texts were further scrutinized to select eligible articles. A standardized table was subsequently devised for data extraction, aligning with the principles of critical appraisal and data extraction for systematic reviews of prediction modeling studies (CHARMS). The extracted data primarily encompassed details such as author names, publication year, country, study design type, study subjects, data sources, study locations, primary outcomes, DVT incidence, DVT types, methods for handling missing values, approaches for continuous variable treatment, variable screening methods, model construction techniques, calibration procedures, validation methodologies, model factors, model performance, and presentation formats of prediction models.
Assessment of Bias Risk in the Included Articles
Fangfang Deng and Kuankuan Xu, two researchers, utilized the Prediction Model Risk of Bias Assessment Tool (PROBAST) 10 to evaluate the risk of bias and applicability of the included articles. They assessed the risk of bias within each article across four domains: study subjects, predictors, results, and statistical analysis. Additionally, they evaluated the applicability of prediction model research based on the first three domains, using a judgment process similar to that for bias risk but without specific problem items. The PROBAST checklist is an invaluable instrument for critically evaluating research related to the development, validation, or updating of predictive models for personalized predictions. It comprises 20 questions organized into four domains: participants, predictors, outcomes, and analysis. Each question can be answered with “Yes,” “Possibly Yes,” “No,” “Probably No,” or “Not Available.” A domain is considered to have a high risk of bias if at least one question within it is answered with “No” or “Probably No.” Overall bias is deemed as low risk only when all domains are assessed to have a low risk of bias.
Data Analysis
A meta-analysis was performed using R Studio software (version 1.1.463) to evaluate the area under the curve (AUC) values for the validation model. It is important to note that the C statistic is also referred to as AUC. The C statistic has a range from 0.5 to 1, where higher values signify improved discriminatory ability. A value of 0.5 denotes no discriminatory ability, while a value of 1 indicates perfect discriminatory ability. Assessment of heterogeneity was carried out using the I2 index and the Cochrane q test. The heterogeneity across studies was assessed using the I2 value. If I2 exceeds 50%, a random effects model is employed to signify high heterogeneity; if I2 is less than 50%, a fixed effects model is utilized. 11 The literature was sequentially excluded to investigate the origins of heterogeneity for sensitivity analysis. Apparent clinical heterogeneity was managed through subgroup analysis, sensitivity analysis, and other methodologies.
Results
Literature Search Process and Results
Initially, 1880 relevant articles were retrieved from the database. Following the removal of duplicates, 922 documents remained. Subsequent screening of titles and abstracts left 61 articles for further evaluation. These studies underwent additional scrutiny to ensure alignment with the study subject type and relevance to the theme, while excluding those that did not establish predictive models or focused solely on risk factors. Ultimately, 7 articles were included. The literature screening process, in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 reporting guidelines, 12 is depicted in Figure 1.
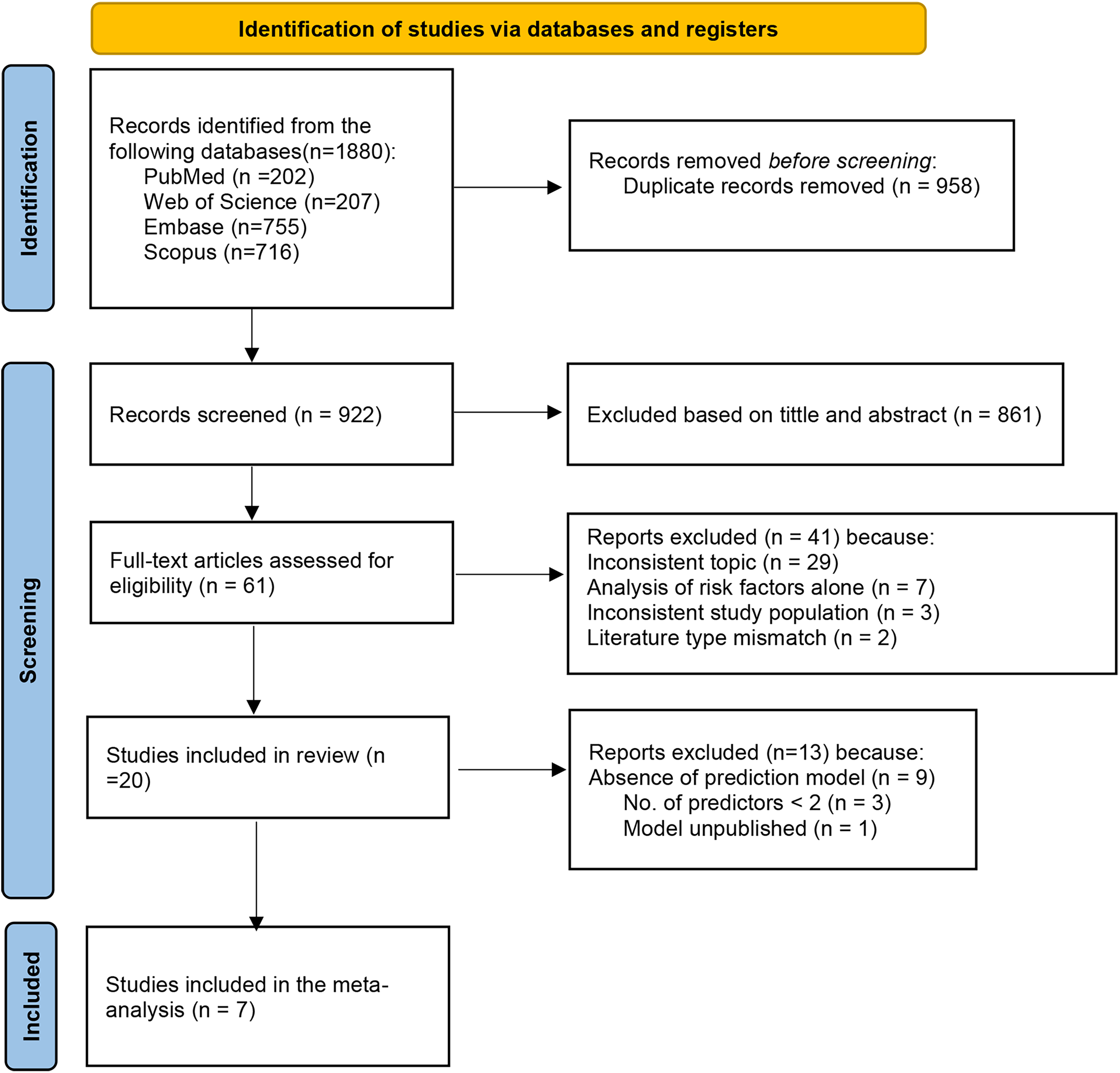
Preferred reporting items for systematic reviews and meta-analyses (PRISMIA) flowchart of literature search and selection.
Basic Characteristics of the Included Studies
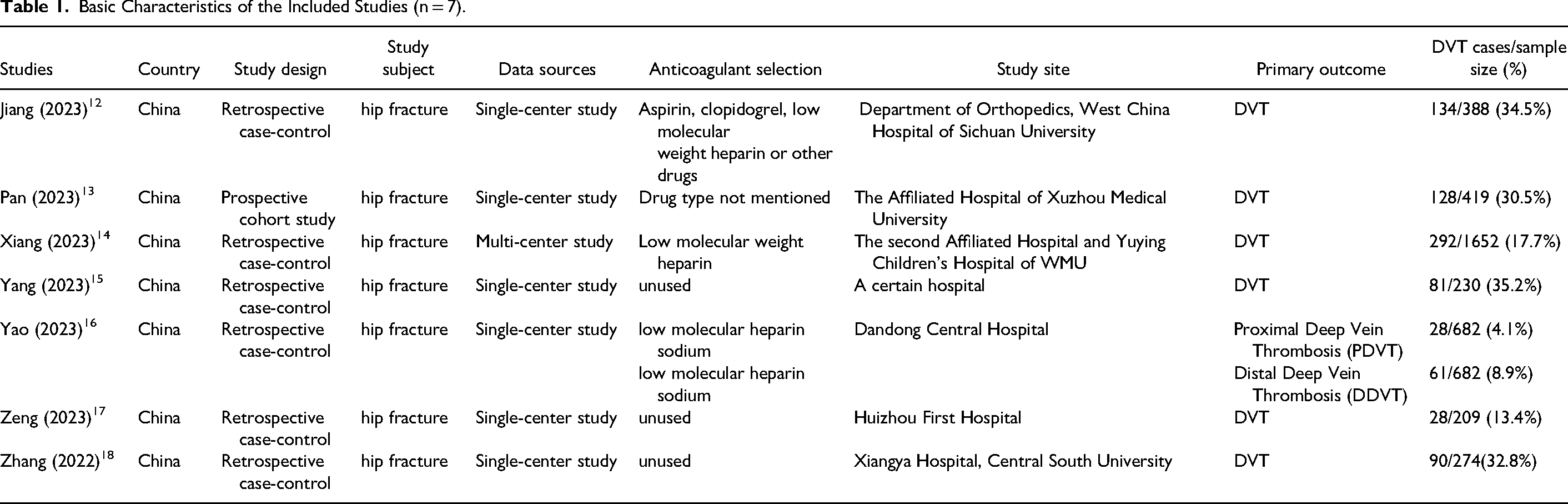
The analysis incorporated a total of 7 studies,13–19 all of which were published in China between 2022 and 2023. Among these, 6 were retrospective case-control studies, and 1 was a prospective cohort study. Additionally, six of the included articles were single-center studies, while one was a multicenter study. The basic characteristics of the included literature are shown in Table 1.
Basic Characteristics of the Included Studies (n = 7).
The analysis in the 7 studies involved the use of logistic regression to develop predictive models, with COX regression used in 1 study. Out of the 8 prediction models, 2 were derived from logistic regression coefficients or processed to create risk assessment formulas, while the remaining 6 were presented as risk prediction nomograms. The most frequently utilized factors across all models were D-dimer and time from injury to admission, which were used in 7 and 4 models, respectively. Other commonly employed factors included fibrinogen (FIB) and diabetes, each utilized in three separate models. In two of the included models, variables such as bed rest time, smoking, age, body mass index (BMI), and systemic immune inflammatory index (SII) were applied. The AUC values or C statistics for the included studies ranged from 0.750 to 0.912, indicating robust model performance. Of these studies, 5 conducted internal validation of their models, while the models by Jiang 13 and Zhang 19 were not validated. Among the validated models, 6 underwent calibration, with goodness-of-fit tests and calibration plots being the most frequently employed methods. Detailed information about the models in the included studies can be found in Table 2.
Overview of the Information of the Included Prediction Models.
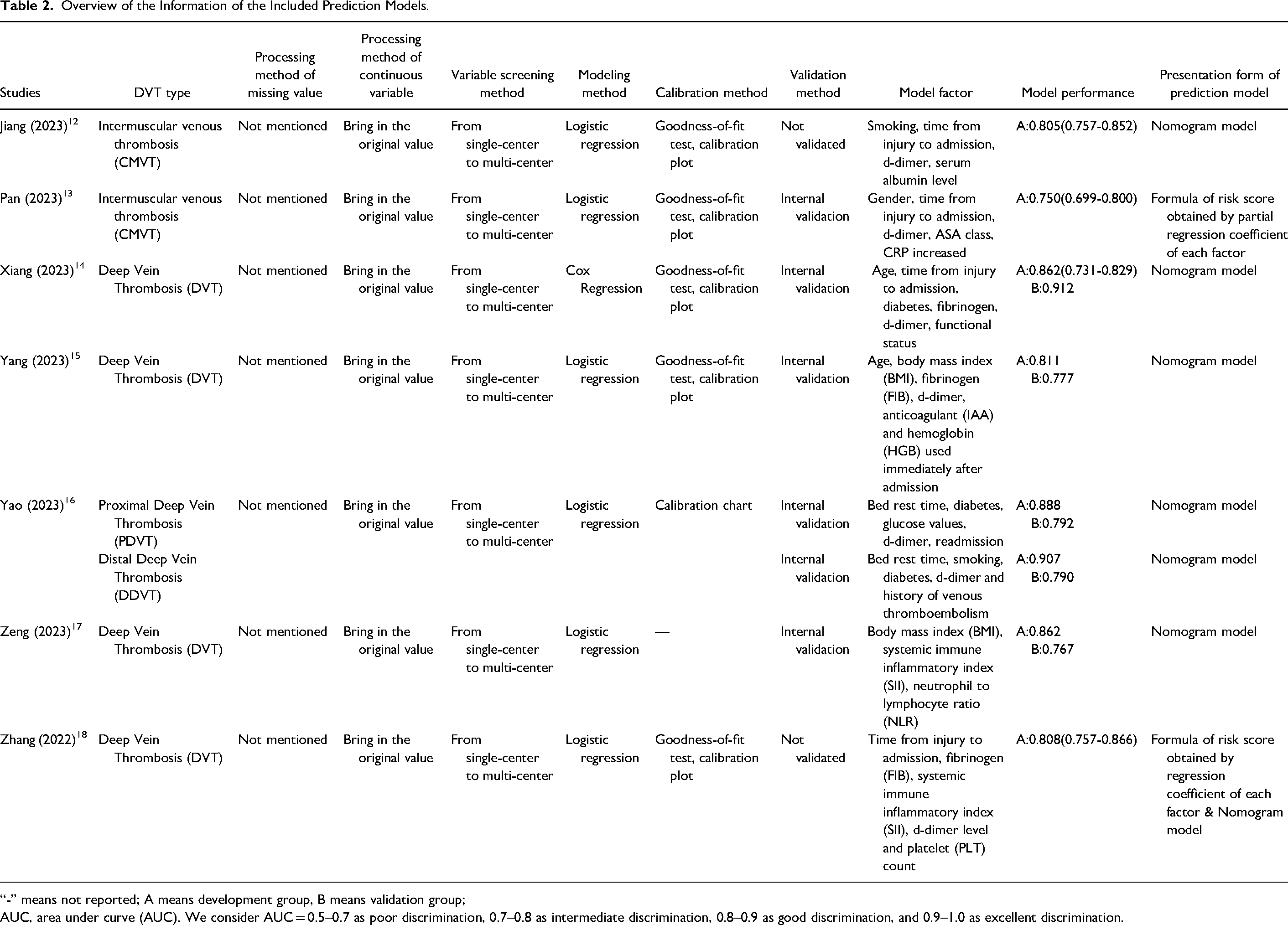
“-” means not reported; A means development group, B means validation group;
AUC, area under curve (AUC). We consider AUC = 0.5–0.7 as poor discrimination, 0.7–0.8 as intermediate discrimination, 0.8–0.9 as good discrimination, and 0.9–1.0 as excellent discrimination.
Risk of Bias and Applicability Evaluation
Table 3 summarizes the risk of bias and applicability for the studies included. Each study was found to have a high risk of bias, indicating methodological issues in either the development or validation process.
Risk of Bias and Applicability Evaluation for the Included Models (n = 7).
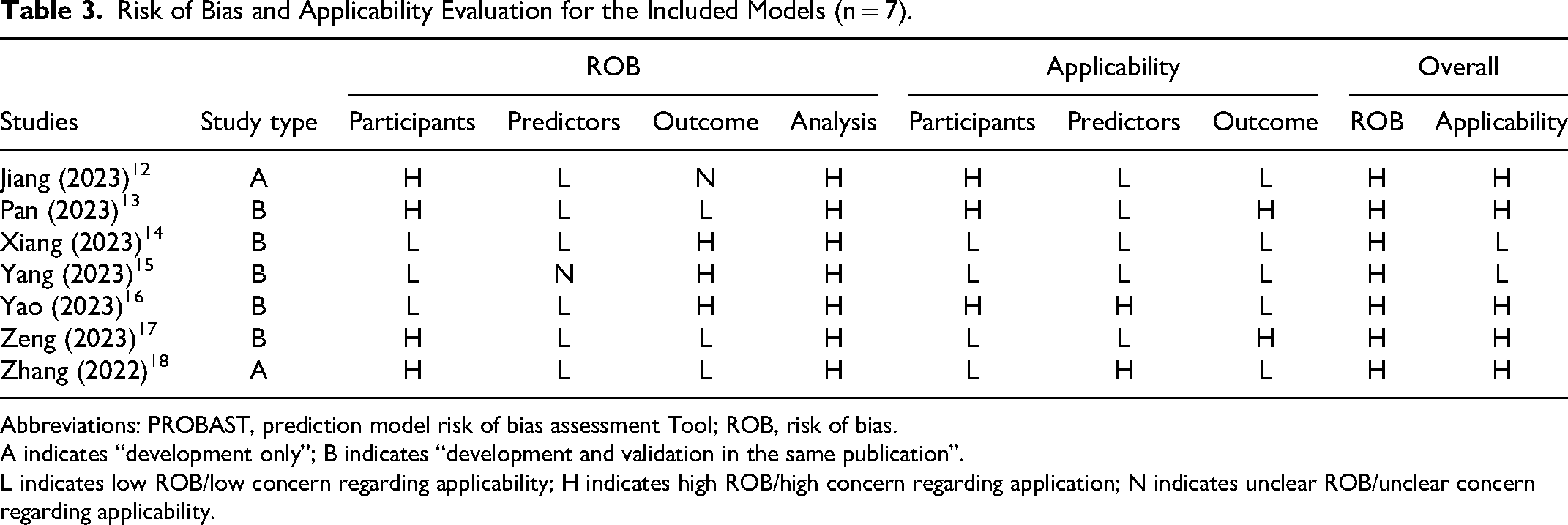
Abbreviations: PROBAST, prediction model risk of bias assessment Tool; ROB, risk of bias.
A indicates “development only”; B indicates “development and validation in the same publication”.
L indicates low ROB/low concern regarding applicability; H indicates high ROB/high concern regarding application; N indicates unclear ROB/unclear concern regarding applicability.
Due to the use of inappropriate data sources, four studies13,14,18,19 in the domain of study subjects displayed a high risk of bias. In the domain of predictor variables, one study 16 showed an unclear risk of bias and lacked quality control measures for predictor assessment. Regarding the outcomes domain, study 13 had an unclear risk of bias, while study 15 inconsistently defined and determined outcomes for all subjects. Additionally, study 16 excluded predictive variables from its outcomes, and study 17 determined outcomes without considering predictive variables, both demonstrating a high risk of bias. In the domain of statistical analysis, seven studies13–19 were identified as having a substantial level of bias. Among these, studies14,17,18 had inadequate sample sizes, failing to meet the recommended guideline of more than 20 events per variable (EPV). Additionally, all seven studies13–19 failed to address appropriate handling of missing values and refrained from screening predictors based on univariate analysis. Furthermore, study 18 did not evaluate the model performance of predictive models, and study 17 did not fully assess model performance. In their model performance evaluations, five studies13–16,19 did not consider issues related to model overfitting or underfitting. Finally, five studies13,15–18 omitted information regarding predictor coefficients in their multivariate regression models, and study 15 conducted internal validation using a single randomly segmented participant data set without appropriately addressing data complexity issues.
Overall, the studies included exhibited a high risk of applicability. ①Regarding study subjects, 3 of the studies lacked relevant information, resulting in uncertainty in assessing bias risk. ②As for predictive factors, 2 studies focused on the definition, assessment methods, and timeline of unreported predictive factors in the included studies. ③Concerning study results, 2 studies addressed inconsistencies in diagnostic criteria for diagnosing elderly hip conditions in both the study and systematic review.
Meta-Analysis of Validation Models
The forest plot package in R Studio software (version 1.1.463) was employed to produce a forest plot of the quantitative indicator C statistic for summarizing model prediction performance. The combined AUC was computed using a random-effects model, resulting in a value of 0.84 (95% confidence interval: 0.80-0.87) (Figure 2). The I2 value is 79% (p < .001), suggesting significant heterogeneity among the studies.
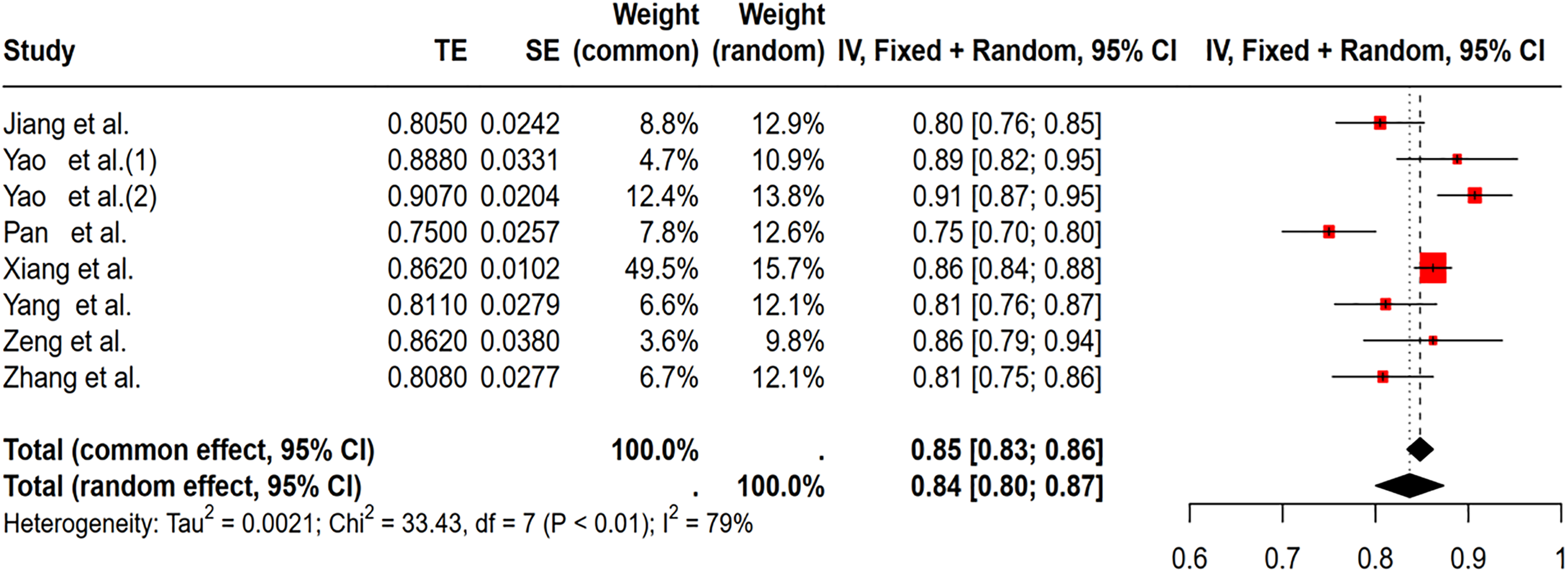
Forest plot for random-effects meta-analysis of AUC values of 8 models.
Subgroup Analysis
A subgroup analysis was performed to investigate the sources of heterogeneity, categorized by the use of anticoagulants. The findings revealed that the subgroup using anticoagulants exhibited a significant heterogeneity with P < .01 and I2 = 86%. The AUC value was 0.84 (95% confidence interval: 0.79-0.90), indicating a reasonable model performance. The sources of heterogeneity might be associated with the type of drug, drug concentration, dosage, dosing duration, and route of administration. 20 In contrast, the subgroup without the use of anticoagulants showed a non-significant result with P = .47, I2 = 0%. The AUC value was 0.82 (95% confidence interval: 0.79-0.85), demonstrating an acceptable model performance (Figure 3).
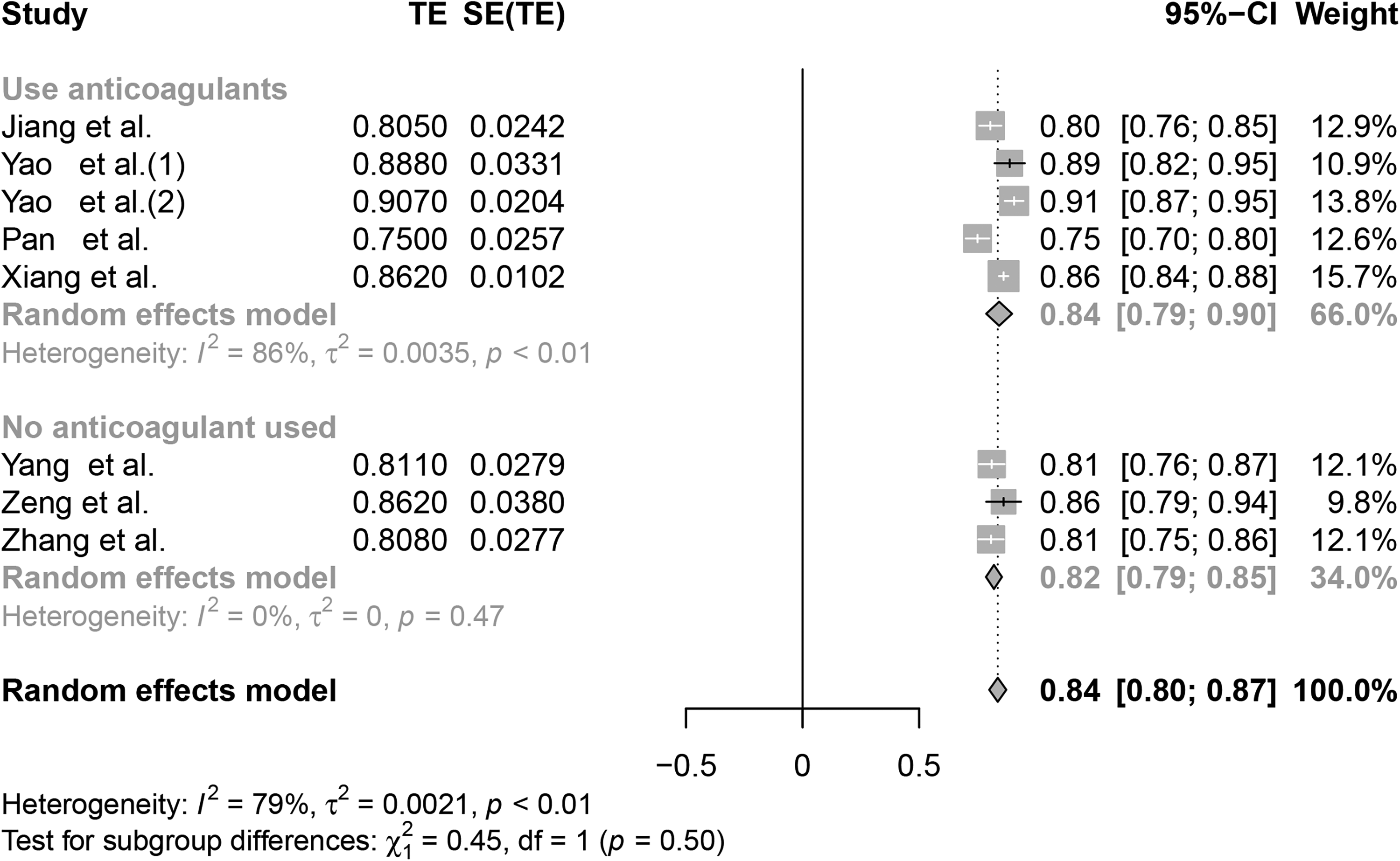
The subgroup analysis of the C-statistic for the risk prediction model of preoperative deep vein thrombosis in elderly patients with hip fractures.
Sensitivity Analysis
After systematically removing individual studies, the combined effect size varied between 0.80 and 0.87, with an I2 of 79% and P < .05. The meta-analysis findings indicated that significant changes were not observed, suggesting the stability of the study results. (Figure 4)
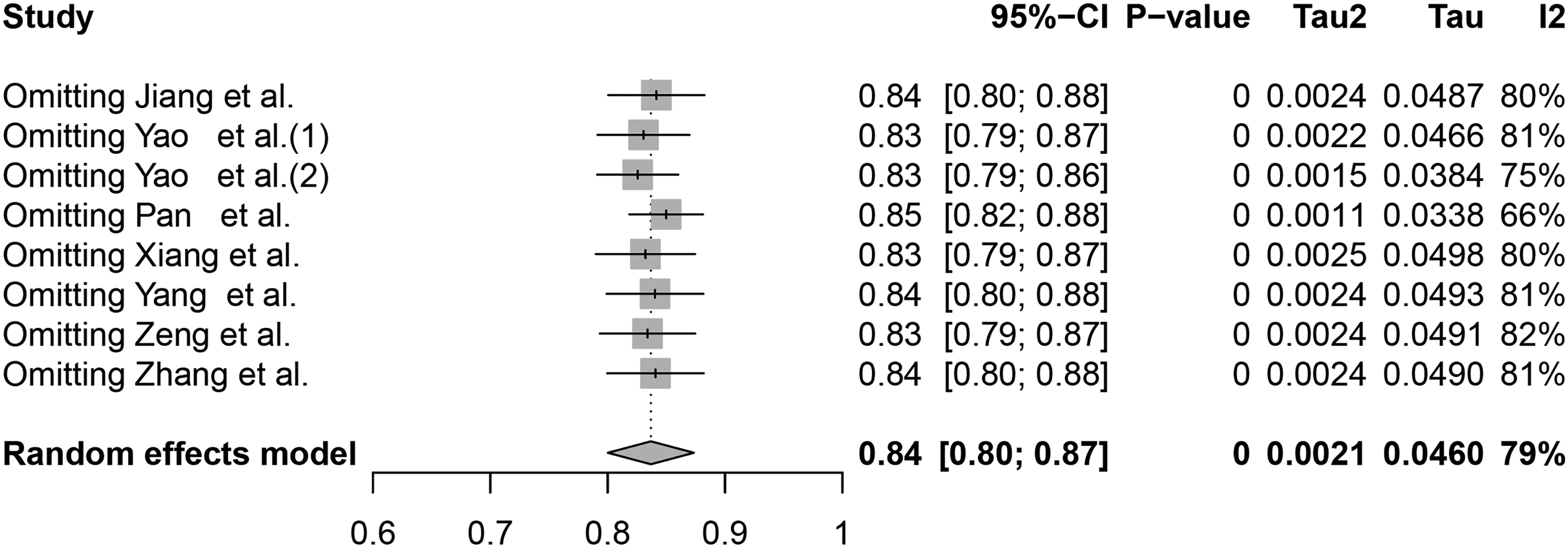
Sensitivity analysis.
Discussion
Deep vein thrombosis is a condition resulting from abnormal coagulation of venous blood and is categorized as a peripheral vascular disease. It is the most common and severe complication associated with hip fractures. 21 Patients diagnosed with deep vein thrombosis are at risk of developing complications such as pulmonary embolism and post-thrombotic syndrome. Additionally, the dislodgement of thrombi can have fatal consequences. 22 Due to the insidious onset of DVT symptoms in most cases, early prevention, accurate diagnosis, and timely treatment are of significant importance in reducing occurrence, delaying progression, and improving the prognosis of deep venous thrombosis in the lower limbs.
Researchers can use a systematic review to comprehensively and objectively evaluate risk prediction models for deep vein thrombosis in patients with hip fractures by employing evidence-based methods. This approach also allows for an assessment of the overall quality of these models, thus laying a solid foundation for their construction and application. Guidelines suggest the utilization of the PROBAST risk assessment tool to evaluate predictive models included in systematic reviews and meta-analyses, in order to clarify their potential applicability and generalizability, as well as to standardize their development. 23 During our evaluation of the eight models included, their AUC values varied from 0.750 to 0.912. The combined AUC value was 0.84 (95% CI: 0.80-0.87), suggesting robust predictive performance of these models. The I2 value of 79% (p < .001) indicates high heterogeneity among the studies. According to the guideline, the standard treatment for deep vein thrombosis (DVT) is anticoagulation, which aims to dilute the blood and reduce further thrombosis. 24 Additionally, it is crucial to evaluate the relative clinical value of anticoagulants from the perspective of healthcare providers and payers. Consequently, a subgroup analysis based on the use of anticoagulants was conducted to investigate the sources of heterogeneity. Guidelines 24 recommend apixaban, dabigatran, edoxaban, or rivaroxaban as alternatives to vitamin K antagonists (VKA) for the initial 3 months of anticoagulant therapy for patients with venous thromboembolism (DVT in the leg or PE) (strong recommendation, moderate certainty evidence). A systematic review and meta-analysis of a randomized controlled trial by Abatzis et al 25 revealed that direct oral anticoagulants (DOACs) demonstrate equivalent efficacy and safety compared to low molecular weight heparin (LMWH). Wells et al 4 observed that patients with DVT should receive anticoagulants for a period of 3 months, which may include LMWH, vitamin K antagonists, or direct factor Xa or direct factor IIa inhibitors. The conclusions concerning the use of anticoagulants align with the findings of our analysis. It is important to note that the studies still carry a significant risk of bias. This elevated risk of bias is mainly attributed to several factors, such as data sources (cohort or case-control studies), time intervals between predictor assessment and outcome determination, the number of events, handling of continuous variables, methods of predictor selection, data complexity, and concerns related to model calibration and overfitting.
This systematic review generally demonstrates a high overall risk of bias in the seven included studies. Differences in study areas, subjects, and predictive factors may be the main reasons for the variations in the final prediction model. Despite the increasing popularity and application of predictive models, there is still no widely applicable model for this population in clinical practice. It is imperative for future studies to adhere to strict model development methods and processes in order to mitigate various potential risks of bias and enhance the predictive power of models. (1) Six studies within the field of study subjects utilized a retrospective cohort study design, which introduces the potential for memory bias or misclassification of outcome events to a certain extent. This uncertainty can affect the relationship between predictors and outcomes. Therefore, it is recommended that future systematic reviews include prospective studies. (2) In the field of predictor factors, risk factors were assessed in a non-blinded manner or in a disparate manner. (3) In the realm of results, the quantity of outcome occurrences did not align with the suggested standard of having over 20 occurrences for each variable, and the definitions and determinations of outcomes were inconsistent. (4) Many statistical studies have failed to effectively address the issue of missing data, which has led to model overfitting. As a consequence, there can be notable discrepancies between the subjects who were excluded and those included in the statistical analysis, thereby introducing bias into the prediction results and model performance. The risk factors have not been appropriately evaluated, potentially resulting in the exclusion of variables with predictive potential. Therefore, it is recommended to consider integrating all variables into multivariate logistic analysis, or adopting alternative variable screening methods such as lasso and random forest. (5) The field of suitability risk assessment revealed a high risk of bias in five studies, while two studies indicated a low risk of bias. Regarding participants, three studies13,14,17 faced a high risk of bias as they limited their participants to the subgroup of deep vein thrombosis (DVT). In terms of predictive variables, two studies17,19 were at high risk of bias primarily due to inaccurate assessment of predictive variables. Moreover, two studies14,18 demonstrated a high risk of bias as their outcome measures encompassed not only DVT but also pulmonary embolism. (6) The internal validation of the models was performed in five studies,14–18 but unfortunately, external validation was lacking, which limited their generalizability. It is recommended that future research should include external validation in hospitals of different regions and levels in China. Geographical and temporal validation approaches can be utilized to enhance the performance of the model and improve its clinical predictability.
Common features were identified among the predictors, which could be classified into four groups: D-dimer, time from injury to admission, fibrinogen, and diabetes. D-dimer, a biomarker originating from cross-linked fibrin clots dissolved by plasmin, primarily indicates fibrinolytic function and holds a crucial role in the clinical identification of disseminated intravascular coagulation (DIC) in adults. 25 The diagnostic efficacy of D-dimer in the detection of deep vein thrombosis (DVT) and pulmonary embolism (PE) has been thoroughly investigated.26–28 A decrease in D-dimer levels may potentially serve to rule out acute thrombosis. 29 Yang et al employed hematology test findings, focusing on D-dimer and fibrinogen (FIB), as risk factors in the prediction of DVT in hip fracture patients. 30 Studies has suggested that 19.5%–32% of hip fracture patients should undergo expedited surgery with reduced waiting times from admission.22,31 In a systematic review and meta-analysis of predictive factors for preoperative deep vein thrombosis in hip fractures, Kobayashi et al 32 also discovered that a prolonged period from injury to admission was correlated with an increased risk of DVT. The high incidence of DVT in clinical practice is often attributed to prolonged ultrasound appointments, extended preoperative preparation times, and overall length of hospital stays. 33 Song et al conducted ascending venography and confirmed that patients awaiting elective surgery for femoral neck fractures had a higher incidence of preoperative deep vein thrombosis, at 29.4%. 34 In addition, additional research35,36 has shown that patients with hip fractures who experience delayed admission of more than 48 h have an approximately 54.5% to 62% increase in the incidence of DVT. Fibrinogen, a protein synthesized in the liver and involved in blood clotting that accelerates clot formation, has been recognized as a dependable predictor of thrombosis after lower limb fracture surgery in a retrospective study. 37 In a meta-analysis of risk factors for preoperative DVT in hip fracture patients, Wang et al 7 discovered that fibrinogen was associated with preoperative DVT, which aligns with our findings on predictive factors. Research in epidemiology has shown that increased levels of circulating particles in individuals with diabetes suggest the presence of systemic inflammation and conditions that promote blood clot formation, thereby increasing the likelihood of thrombosis. It is recommended that in the future, a systematic and comprehensive approach be taken to integrate these identified risk factors in order to pinpoint the high-risk population vulnerable to deep vein thrombosis. Xu et al 38 discovered a linear correlation between MCV and preoperative DVT in elderly patients with hip fractures, suggesting MCV as an indicator for predicting DVT risk. The use of MCV may aid in evaluating and mitigating adverse outcomes in older individuals. Nonetheless, there are inconsistencies in the predictive factors identified in this study, highlighting the need for further research to enhance understanding of MCV's role in the future.
Universal DVT prediction models commonly utilized in clinical settings include the Caprini risk assessment model, the Wells scale, and the Autar scale. The Caprini Scale, 39 originally created for hospitalized patients in the United States, is valuable for assessing venous thrombosis risk factors in this population. However, it demonstrates a lack of sensitivity when applied to hip fracture patients and adds to the workload for clinical staff due to its complexity and time-consuming nature. The Well Scale40,41 primarily focuses on a patient's medical history and clinical presentation. When used for hip fracture patients, it tends to classify nearly all patients as high risk, which limits its accuracy in evaluating DVT within this specific patient population. The Autar Scale, 42 tailored for orthopedic patients, exhibits limited specificity in predicting venous thrombosis in patients undergoing major orthopedic surgery. In summary, these models assess a wide range of variables but lack specificity. Furthermore, they are rarely integrated into routine clinical examination data for screening purposes. 43 However, Chinese scholars have developed a specific risk prediction model for DVT targeting older patients with hip fractures, utilizing simplified variables. This model even incorporates specific fracture types (femoral neck fracture, intertrochanteric fracture, and subtrochanteric fracture) and various perioperative time periods. As a result, the high-quality risk prediction model discussed in this article shows promise for practical clinical application following appropriate adjustments.
It is important to highlight that, with the exception of the Xiang et al, 15 study, which utilized the COX regression method, all other studies employed logistic regression to develop models, with limited utilization of machine learning methods. A study 44 indicated that machine learning methods tend to achieve higher accuracy compared to traditional logistic regression and COX regression. Many of the studies included in the analysis encountered challenges related to sample size, treatment of continuous variables, and predictor selection. The incorporation of machine learning methods into model development has the potential to address some of these issues. For instance, Jang et al utilized machine learning to accurately predict the risk of hip replacement surgery over a period of 10 years. 45 It is important to recognize, however, that a limitation of machine learning models is the current absence of suitable visualization tools. Additionally, the fact that all the study sites included are in China somewhat restricts the generalizability of the study results to Western populations. Proper adjustments are necessary when applying these models in different regions. The small number of included studies, with only 7 relevant articles, may lead to the existence of publication bias. In addition, the studies included were predominantly written in English, and publications in other languages were excluded due to language barriers. Quantitative meta-analysis was not conducted due to heterogeneity in the definitions and measurement methods of predictive outcomes, as well as the assessment of predictive model performance in the included studies. Future researchers are encouraged to refer to PROBAST during the model-building process and adhere to reporting guidelines for multivariate forecasting models to minimize bias and ensure scientific rigor in model development. Furthermore, it is advisable to extensively utilize machine learning techniques in future research. There is a need for multi-center and large-sample studies to further validate the applicability of contentious predictors and models.
Conclusion
A systematic review was carried out on the 7 studies included in this study. The results indicate a growing emphasis on research concerning risk prediction models for deep vein thrombosis prior to hip fracture surgery. Nevertheless, it is apparent that these models exhibit a high risk of bias and are still in the developmental phase. Subsequent research efforts should conform to recognized standards for model development and reporting. Researchers should also take into account aligning their work with clinical practice and endeavor to choose or develop risk prediction models that display outstanding predictive performance, minimal bias, and are user-friendly in the Chinese healthcare setting.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241285565 - Supplemental material for Risk Prediction Models for Preoperative Deep Vein Thrombosis in Older Patients with Hip Fracture: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-cat-10.1177_10760296241285565 for Risk Prediction Models for Preoperative Deep Vein Thrombosis in Older Patients with Hip Fracture: A Systematic Review and Meta-Analysis by Huali Guo, Kuankuan Xu, Fangfang Deng, Qingqing Chen, Jie Liang and Kun Zhang in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Yichang city-level project: Construction of a model for predicting the frailty risk of brittle fractures in the elderly, (grant number A23-1-031).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.