
Abstract
Cerebral venous sinus thrombosis (CVST) is a rare neurovascular condition that has been observed in individuals with coronavirus disease 2019 (COVID-19). This systematic review aimed to explore the sex differences and characteristics of concurrent COVID-19 and CVST cases. A total of 212 CVST patients were included in the study. Women with CVST had a slightly higher mean age compared to men (47.359 years vs 46.08 years). Women were more likely to report symptoms such as fever (56.1%) and decreased sense of smell or taste (71.4%), while men more frequently experienced nausea or vomiting (55.6%), headache (62.9%), and seizures (72%). Notably, current smokers, who were predominantly men, had a higher occurrence of CVST. On the other hand, women had a higher likelihood of CVST risk factors such as oral contraceptive pill (OCP) use and autoimmune diseases. Treatment approaches also showed sex-based differences. Unfractionated heparin was administered more often to women with CVST (63.2%). The in-hospital mortality rate for CVST patients was 21.3%, with men having a significantly higher mortality rate than women (65.2% vs 34.8%, P = .027). Survival analysis revealed that factors such as smoking history, diabetes mellitus, hypertension, OCP use, COVID-19 symptoms, CVST symptoms, and the need for intubation significantly influenced survival outcomes. Understanding these sex differences in COVID-19-related CVST is crucial for accurate diagnosis and effective management, ultimately leading to improved patient outcomes. Our findings highlight the importance of considering sex as a factor in the evaluation and treatment of individuals with COVID-19 and concurrent CVST.
Introduction
Cerebral venous sinus thrombosis (CVST) is a rare neurovascular condition with an approximate annual occurrence of 1.6 cases per 100 000 individuals. 1 However, the precise prevalence of CVST in individuals with coronavirus disease 2019 (COVID-19) remains unclear. 2 In certain cases of COVID-19, thromboembolic events affecting the nervous system leading to cerebrovascular stroke have been documented as an initial manifestation following mild flu-like symptoms. COVID-19, which is primarily characterized as an acute respiratory disease, is caused by a single-stranded RNA virus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 3 Neurological complications are frequently observed in individuals with COVID-19, especially among those who require hospitalization 4 ; the observed rates of these complications are higher in such patients than in those with milder disease. 5 COVID-19-associated complications reported in the literature include CVST and pulmonary embolism.6,7 The occurrence of CVST is significantly less common and is predominantly reported during the active phase of the COVID-19 infection. 8 However, the exact mechanism underlying the hypercoagulable state associated with COVID-19 is not well understood. Nonetheless, various hypotheses have been proposed to elucidate the potential pathophysiological mechanisms, including receptor binding, complement activation, cytokine storms, and direct viral endothelial damage.9–12
This study presents a literature review of all reported cases of CVST and COVID-19 since the emergence of COVID-19 in early 2019 to January 1, 2022. To improve the diagnosis and treatment of patients with CVST and COVID-19, we investigated the demographic, clinical, radiological, and prognostic characteristics of the association between the diseases. Our study aimed to provide insights into the variables that might play a role in the worsening of CVST and patient outcomes and to study the sex difference in clinical outcomes in patients with CVST and COVID-19.
Methods
Search Strategy
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Figure 1). A comprehensive literature search was performed using PubMed, the Web of Science, and Google Scholar on January 1, 2022. The search strategy comprised different combinations of the following terms: COVID, COVID-19, SARS-CoV-2, severe acute respiratory syndrome coronavirus 2, cerebral venous thrombosis, CVST, intracranial sinus thrombosis, CVT, and CVST. Reference lists of the selected studies were further reviewed to identify relevant studies.
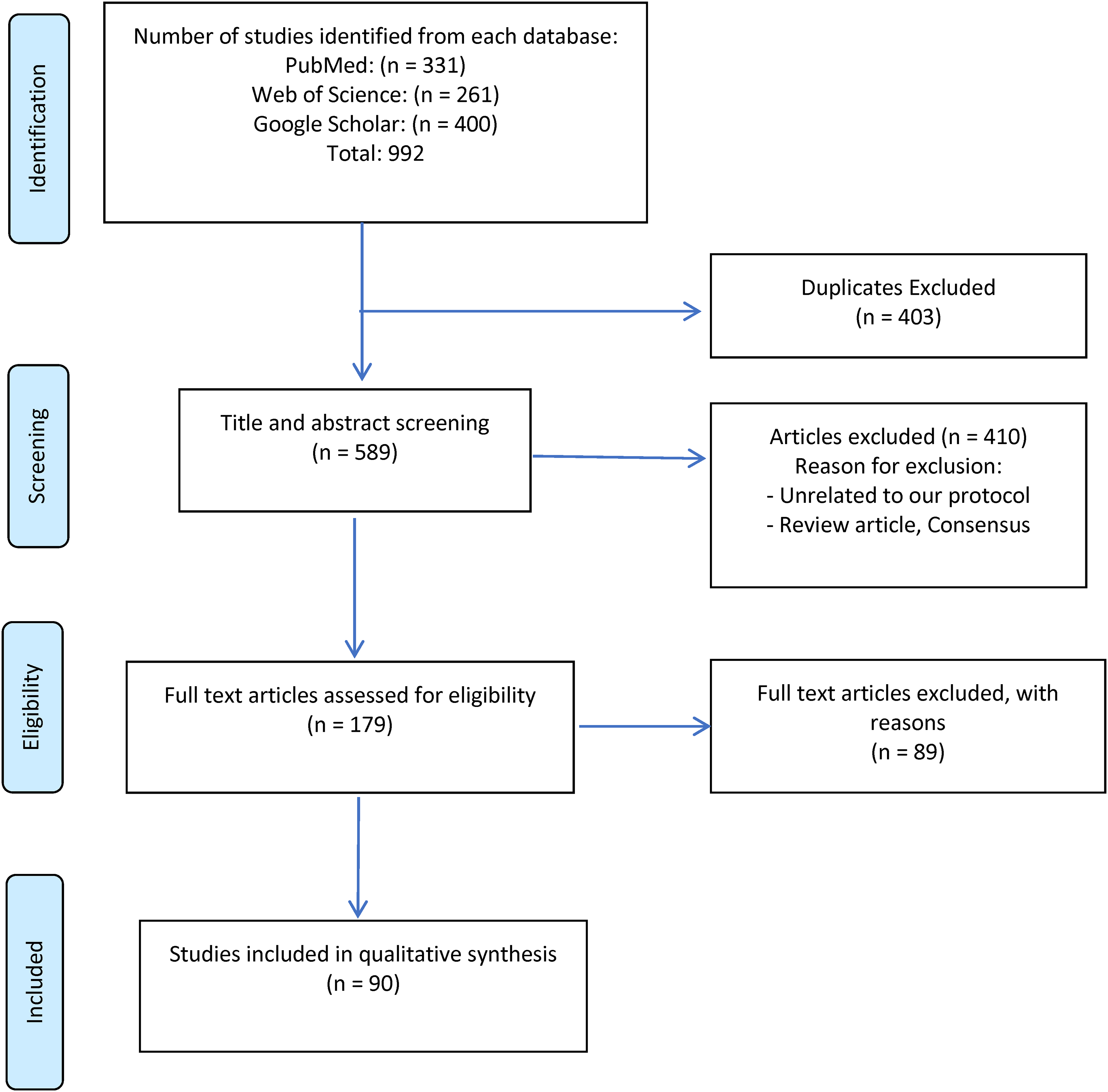
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the systemic review.
Selection Criteria, Bias Assessment, and Data Sharing
Studies were included based on the following criteria: (1) Reports of patients with COVID-19 who developed CVST; (2) CVST was not related to SARS-CoV-2 vaccine administration; (3) case reports, case series, case-control studies, and retrospective and prospective cohort studies. Studies in languages other than English and nonhuman studies were excluded. Reviews, editorials, and letters were excluded unless original data were provided. No restriction on the age of patients was imposed.
Two reviewers (S.A. and A.A.) independently screened the titles and abstracts and evaluated the full texts of the studies meeting the inclusion criteria.
Any discrepancies were resolved via discussion with the corresponding reviewer (N.G.). Data from each article were extracted using Microsoft Excel.
We assessed the quality of the included case reports and case series in accordance with the guidelines recommended by the Johanna Briggs Institute. For the case series, we evaluated the presence of clear inclusion criteria, reliable measurement of the condition, valid methods for identifying the condition, consecutive or complete inclusion, and reporting of patient demographics, clinical information, and outcomes. In the case of case reports, we scrutinized the description of patient demographics, medical history, clinical conditions, diagnostic tests, treatment, post-treatment clinical condition, adverse events, and take-home messages. Supplementary tables for both are provided.
Data Extraction, Qualitative, and Quantitative Synthesis
The relevant quantitative data were extracted by 2 authors (S.A. and A.A.). Where available, the data included patient demographics, COVID-19 and CVST symptoms, comorbidities, CVST risk factors, relevant laboratory results, treatment, and patient outcomes.
Statistical Analysis
Statistical analyses were performed using SPSS® statistical software package version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows® (Microsoft, Redmond, WA, USA). Continuous variables are presented as means and standard deviations, and categorical variables are presented as frequencies and percentages, and the differences were estimated using chi-square tests. This study focused on sex differences, considering various factors such as mean age (SD) in years, sex, CVST during COVID-19, CVST post-COVID-19 recovery, days from COVID-19 symptoms to CVST, prior antiplatelet/anticoagulation medication use, associated thrombotic events, intensive care unit/floor/home stay, intubation, and other variables such as comorbidities, CVST risk factors, and laboratory results. Survival analysis was performed with overall survival (OS) in days as the primary and secondary outcome. The patients were followed up until they experienced the outcome of interest or the date of death. Statistical significance was set at P < .05.
Results
The systematic literature search identified 992 relevant studies. Through a rigorous screening process based on the inclusion criteria, 90 studies were deemed suitable for inclusion. The selected studies, as depicted in the PRISMA flowchart (Figure 1), collectively involved 212 patients. The inclusion of these studies from the existing literature strengthened the comprehensiveness and validity of the analyses conducted herein.
Patients’ Baseline Characteristics and key Investigations
Table 1 shows that when the 212 patients diagnosed with CVST were divided based on their sex, the mean age was slightly higher in women (47.359 ± 1.514 years) than in men (46.08 ± 1.452 years). The difference in age between the 2 groups was statistically significant (p = .027).
Patient Characteristics According to Sex.
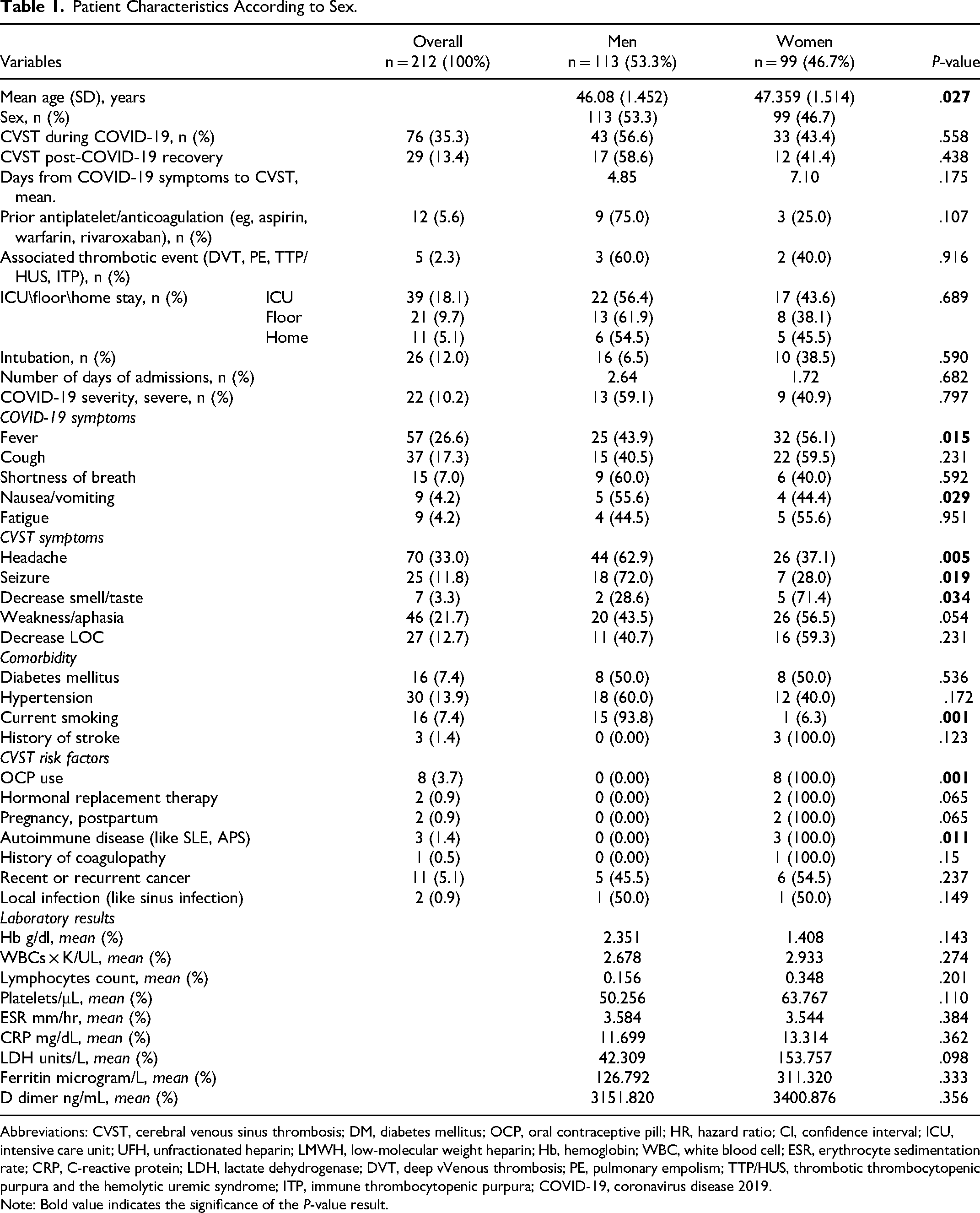
Abbreviations: CVST, cerebral venous sinus thrombosis; DM, diabetes mellitus; OCP, oral contraceptive pill; HR, hazard ratio; CI, confidence interval; ICU, intensive care unit; UFH, unfractionated heparin; LMWH, low-molecular weight heparin; Hb, hemoglobin; WBC, white blood cell; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; LDH, lactate dehydrogenase; DVT, deep vVenous thrombosis; PE, pulmonary empolism; TTP/HUS, thrombotic thrombocytopenic purpura and the hemolytic uremic syndrome; ITP, immune thrombocytopenic purpura; COVID-19, coronavirus disease 2019.
Note: Bold value indicates the significance of the P-value result.
In terms of COVID-19 and CVST symptoms, women were more likely to report certain symptoms such as fever (32/57; 56.1%; p = .015) and decreased sense of smell or taste (5/7; 71.4%; p = .034). In contrast, men more frequently experienced nausea or vomiting (5/9; 55.6%; p = .029), headache (44/70; 62.9%; p = .005), and seizures (18/25; 72%; p = .005).
Regarding comorbidities and risk factors, the occurrence of CVST was higher among current smokers, who were more frequently men (15/16; 93.8%; p = .001). In contrast, women had a significantly higher likelihood of the presence of CVST risk factors, such as oral contraceptive pill (OCP) use in 8 patients (100%) (p = .001) and autoimmune diseases in 3 patients (100%) (p = .011). No significant differences were observed between the groups in terms of laboratory results.
In-Hospital Treatments of CVST Patients
Table 2 highlights the treatment options utilized for patients diagnosed with CVST and their respective frequencies among men and women. The analysis revealed that unfractionated heparin was administered significantly more frequently to women than to men, with a utilization rate of 63.2% (24 of 38 women with CVST). In contrast, men had a relatively low frequency of unfractionated heparin administration. This disparity in the use of unfractionated heparin between the sexes was statistically significant (p = .021), suggesting a possibility of a sex-based difference in the treatment approach for CVST patients. However, when taking the overall number of men of 42 versus women of 41 who received either unfractionated heparin or low molecular weight heparin, we can see no significance in the treatment approach.
In-Hospital Treatments of Cerebral Venous Sinus Thrombosis (CVST) Patients.
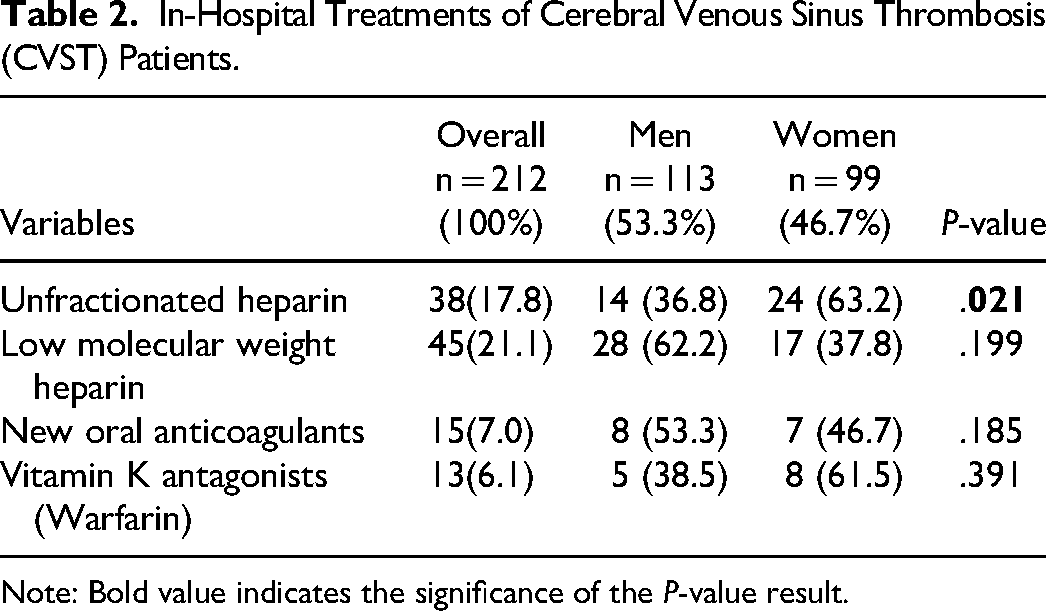
Note: Bold value indicates the significance of the P-value result.
In-Hospital Outcomes of CVST Patients
Table 3 presents the outcomes observed among the patients diagnosed with CVST, including mortality rates and measures of recovery. A full recovery was determined as a complete recovery with no residual deficit. Partial recovery was determined if the patient still had some deficit (sensory/motor/cognitive) but not a decreased level of consciousness. Poor recovery was determined for anyone who is bedbound or has a persistent decrease in LOC. Of all the patients with CVST (46 [21.3%]) experienced in-hospital mortality. Men had a significantly higher rate of in-hospital mortality than women, with 30 of 46 male patients (65.2%; p = .027) succumbing to the condition. However, among patients who recovered from CVST, no statistically significant sex differences were observed in terms of recovery outcomes.
In-Hospital Outcomes of Cerebral Venous Sinus Thrombosis (CVST) Patients.
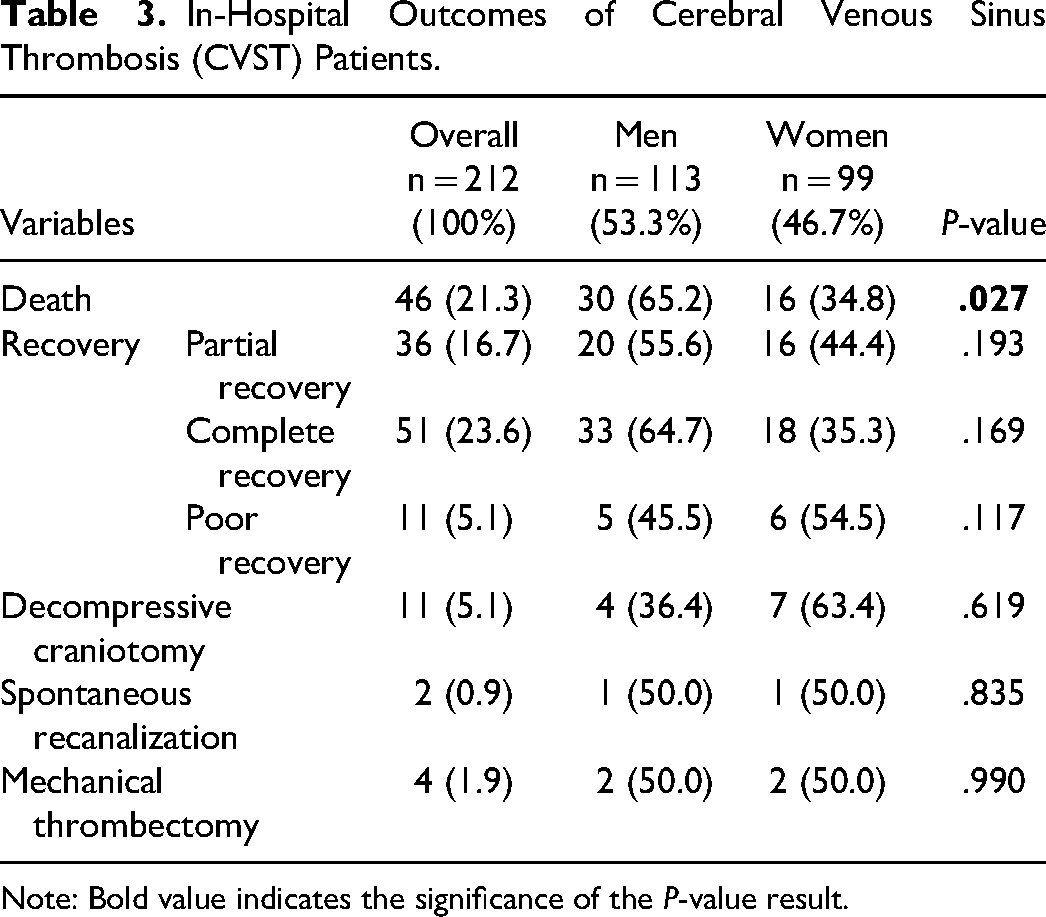
Note: Bold value indicates the significance of the P-value result.
Survival Analysis Using Kaplan–Meier Curves and the log-Rank Test
The survival outcomes of patients diagnosed with CVST were analyzed using Kaplan–Meier curves and log-rank tests (Figures 2, 3, and 4). Various variables were examined, including OS, sex, CVST during COVID, CVST after COVID, smoking history, diabetes mellitus, hypertension, OCP use, autoimmune disease, COVID-19 symptoms, CVST symptoms, intensive care unit setting, intubation, brain hemorrhage, brain imaging findings, and CVST treatment types.
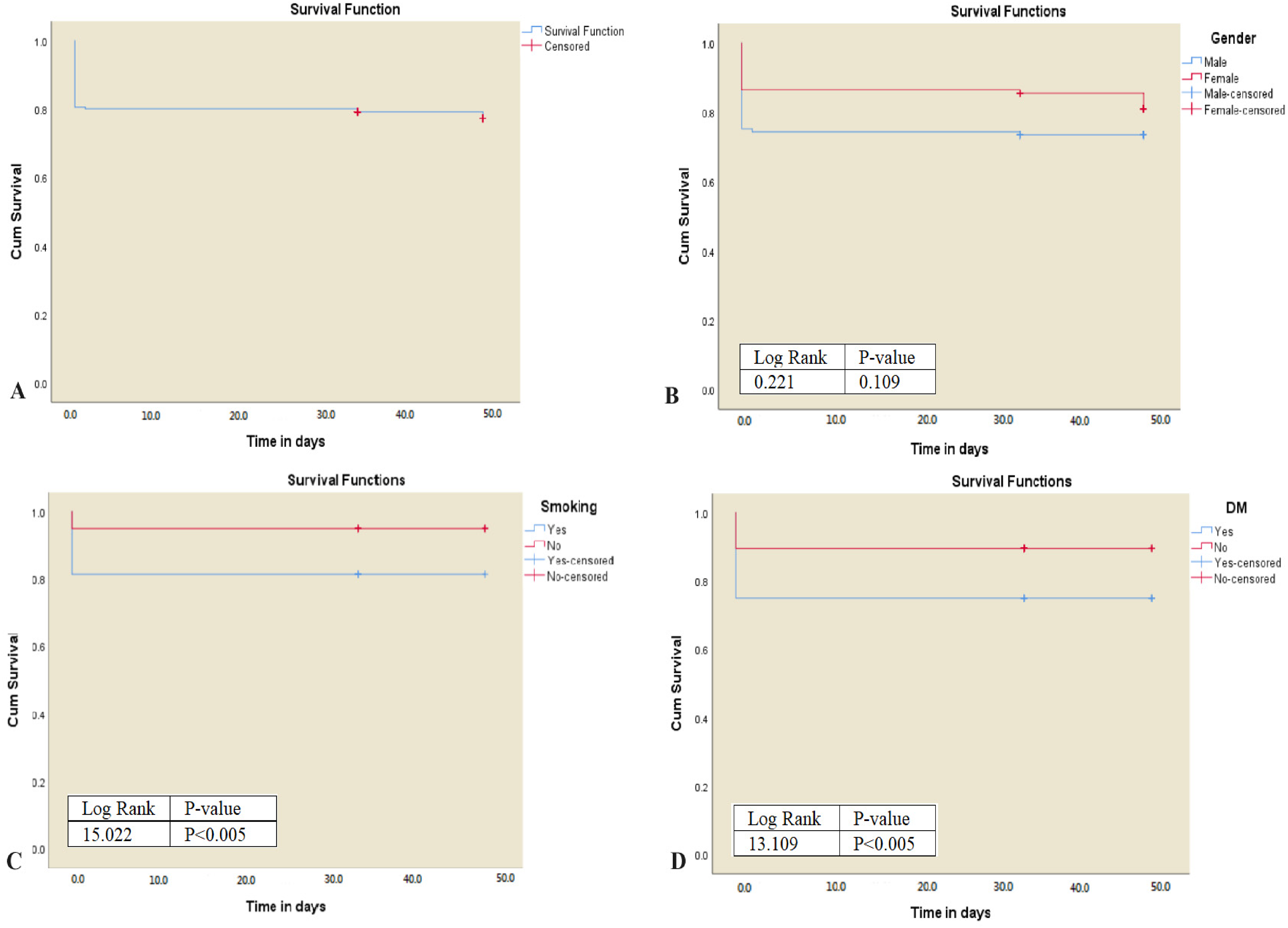
(A) Overall survival of patients with cerebral venous sinus thrombosis (CVST). (B) The log-rank test indicates that there is no difference in survival between different sexes at diagnosis (log-rank 0.221, p = .109). (C) There is a significant difference in the survival between participants who have CVST and a history of smoking or diabetes mellitus (D) than those who do not (log-rank 15.022, P = .005) and (log-rank 13.109, p = .005).
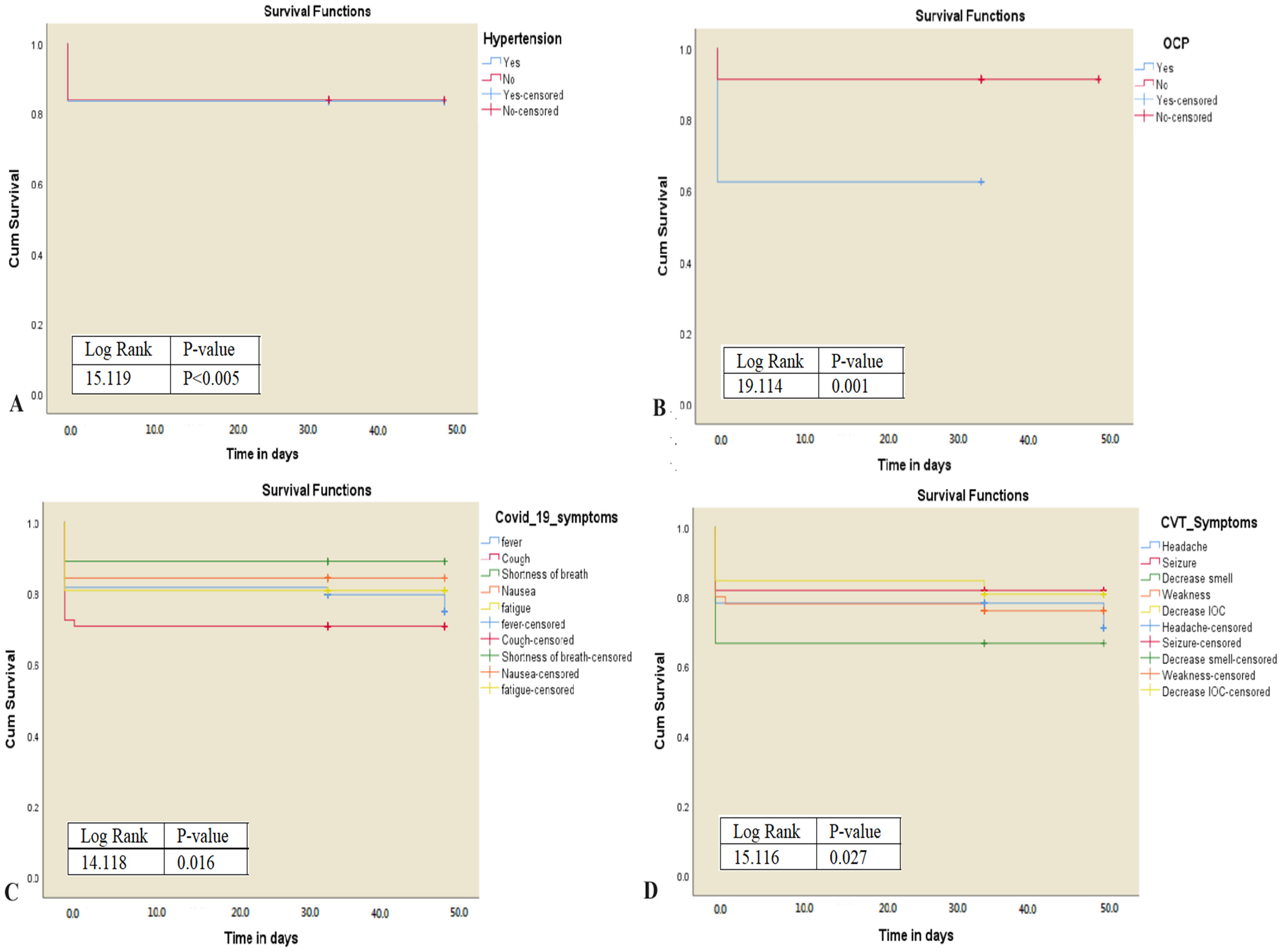
(A) and (B) The log-rank test indicates that there is a significant difference in survival of patients with hypertension (log-rank 15.119, p = .005) and a history of OCP use (log-rank 19.114, p = .005) compared with those without. (C) and (D) There is a significant difference in the survival between participants who have CVST and COVID-19 symptoms (log-rank 14.118, p = .016) or CVST symptoms (log-rank 15.126, p = .027) (D) than those who do not. Abbreviations: CVST, cerebral venous sinus thrombosis; COVID-19, coronavirus disease 2019; OCP, oral contraceptive pill.
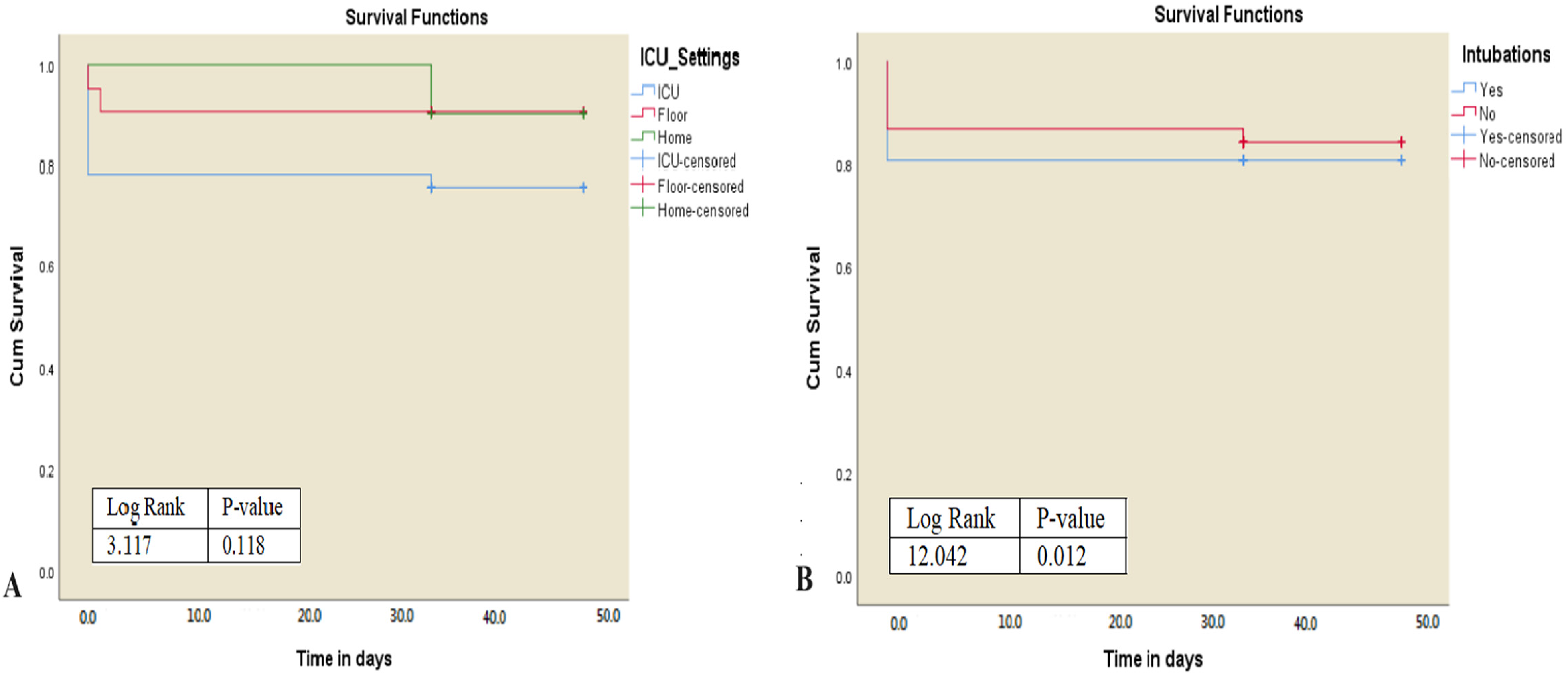
(A) The log-rank test indicates that there is no difference in survival of different settings at diagnosis (log-rank 3.1, p = .118). (B) There is a significant difference in survival between participants who have cerebral venous sinus thrombosis (CVST) and are intubated and those who do not (log-rank 12.042, p = .012).
A history of smoking (p = .005), diabetes mellitus (p = .005), hypertension (p = .005), and OCP use (p = 0.001), different COVID-19 symptoms (such as fever, cough, etc) (p = 0.016), different CVST symptoms (such as headache, seizure, etc) (p = 0.027), and the need for intubation (p = 0.012) had a significant influence on survival outcomes. Brain imaging findings and the CVST treatment type had no significant influence on survival outcomes.
Univariate and Multivariate Logistic Regression Analyses to Determine the Independent Predictor of CVST Development
A stepwise univariate and multivariate analysis approach was used for the analysis of different factors associated with CVST among COVID-19 patients (Table 4). The univariate analysis revealed that several variables showed significant associations with CVST development. These included smoking (HR = 15.51, 95% CI = 2.42-14.32, p = .005), diabetes mellitus (HR = 19.12, 95% CI = 2.13-8.13, p = .005), and hypertension (HR = 16.19, 95% CI = 2.13-10.17, p = .005). Additionally, OCP use (HR = 12.73, 95% CI = 1.35-11.93, p = .001) and COVID-19 symptoms (HR = 12.83, 95% CI = 2.16-11.79, p = .016) were also significantly associated with CVST.
Univariate and Multivariate Logistic Regression Analyses to Determine the Independent Predictor of Cerebral Venous Sinus Thrombosis (CVST) Development.
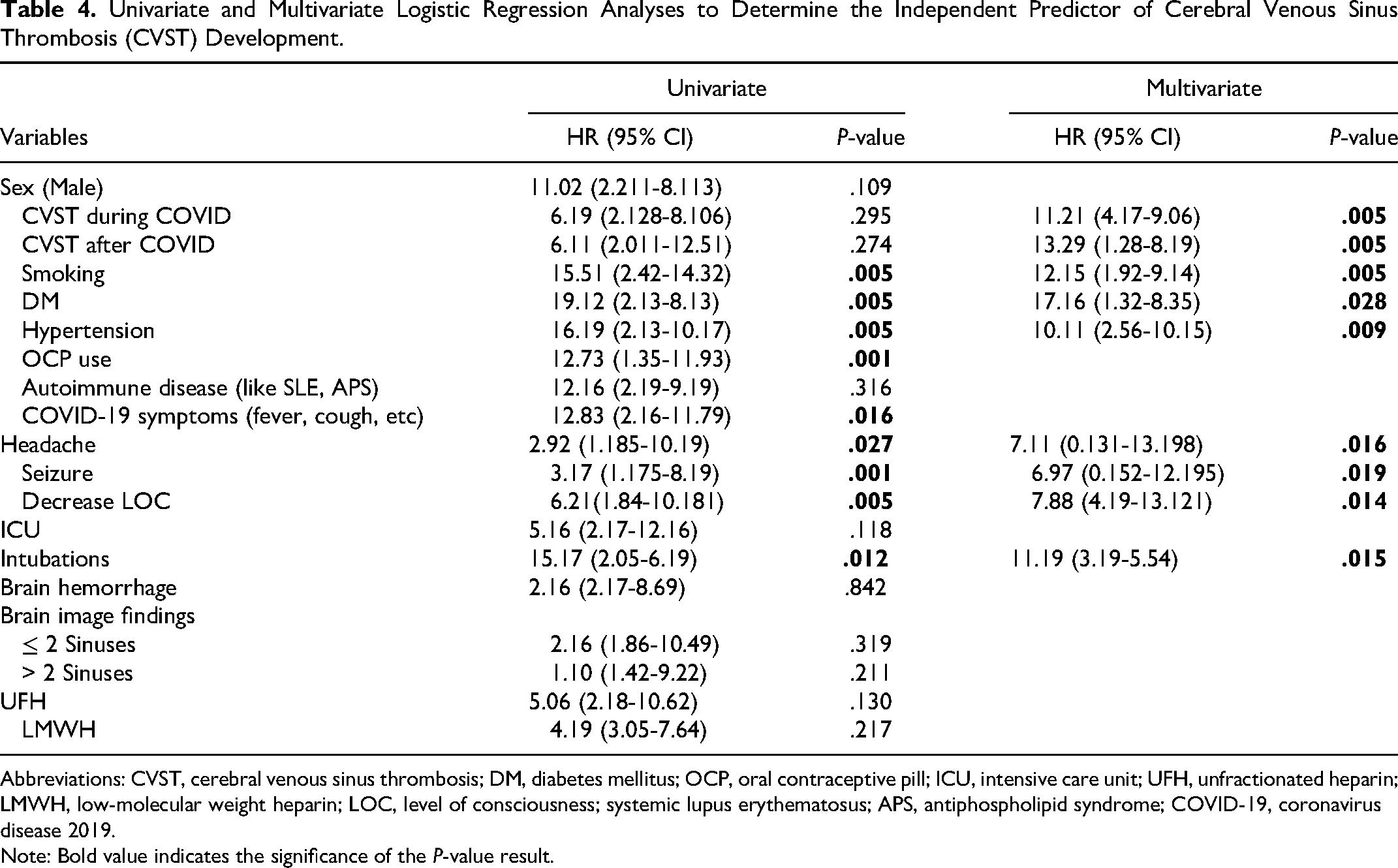
Abbreviations: CVST, cerebral venous sinus thrombosis; DM, diabetes mellitus; OCP, oral contraceptive pill; ICU, intensive care unit; UFH, unfractionated heparin; LMWH, low-molecular weight heparin; LOC, level of consciousness; systemic lupus erythematosus; APS, antiphospholipid syndrome; COVID-19, coronavirus disease 2019.
Note: Bold value indicates the significance of the P-value result.
In the multivariate analysis, after adjusting for other variables, smoking (HR = 11.21, 95% CI = 4.17-9.06, p = .005), diabetes mellitus (HR = 13.29, 95% CI = 1.28-8.19, p = 0.005), hypertension (HR = 12.15, 95% CI = 1.92-9.14, p = .005), OCP use (HR = 17.16, 95% CI = 1.32-8.35, p = .028), and COVID-19 symptoms (HR = 10.11, 95% CI = 2.56-10.15, p = .009) remained independent predictors of CVST development.
Furthermore, certain clinical factors were also found to be significant predictors of CVST. These included headache (HR = 2.92, 95% CI = 1.185-10.19, p = .027), seizures (HR = 3.17, 95% CI = 1.175-8.19, p = .001), and decreased level of consciousness (HR = 6.21, 95% CI = 1.84-10.181, p = .005). Intubation (HR = 11.19, 95% CI = 3.19-5.54, p = .015) was also identified as a significant predictor of CVST in both univariate and multivariate analyses.
Discussion
This study aimed to investigate the association between COVID-19 and CVST by analyzing data obtained through a comprehensive literature review. The analyses focused on understanding the sex differences and clinical outcomes in patients with both conditions. CVST in patients with COVID-19 involves a complex interplay of factors. It is associated with the hypercoagulable state induced by the virus, potentially leading to thrombosis in multiple body regions, including the cerebral venous system. The interaction between SARS-CoV-2 and the angiotensin-converting enzyme 2 (ACE2) receptor on the vascular wall plays a significant role in this process. This interaction triggers immunothrombosis, characterized by endothelial activation, cytokine storm, leukocyte and platelet recruitment, and the activation of the coagulation extrinsic pathway. Additionally, the rise in angiotensin II levels, which promotes inflammation, may contribute to the development of CVST12-16. The study included 212 patients with CVST, and interestingly, women had a slightly higher mean age than men, which was statistically significant. The mean age of the patients in our study was greater than that in previous reports on CVST unrelated to COVID-19 infection (46.08 years for men and 47.35 years for women herein vs 35 years in previous studies).17,18 Given that older individuals are generally more susceptible to COVID-19 infection, it is reasonable to expect that the mean age of patients with COVID-19-related CVST would be higher. 19
Regarding clinical presentation, headache, seizures, and decreased level of consciousness were observed to be independent predictors of CVST development in univariate and multivariate analyses. Interestingly, men with CVST showed a higher incidence of headaches and seizures, whereas women had a greater prevalence of prior COVID-19 symptoms, such as loss of taste and smell. This discrepancy in symptoms can potentially lead to delayed diagnosis and initiation of treatment for CVST in women because their symptoms may be attributed to the transient effects of COVID-19. This emphasizes the significance of maintaining vigilance and a thorough evaluation and consideration of CVST in patients with COVID-19, especially in women who do not exhibit classic cavernous sinus syndrome or encephalopathy.20,21
All COVID-19 severity measures were higher among men, despite not being statistically significant, which corroborates prior studies.19,22 This could add to the challenge when approaching cases of CVST in men, which is not as common as in women and who do not have common risk factors, such as OCP use or autoimmune conditions. Consequently, these challenges may adversely affect clinical outcomes.23,24
Precipitating and predisposing factors, such as OCP use and the presence of prior autoimmune conditions, are known to be associated with CVST.25,26 These findings were corroborated in our study, which may suggest some causality20,27-30.
Prior comorbid conditions such as diabetes mellitus, hypertension, or smoking, in addition to the known risk factors for developing severe COVID-19, were observed to be independent predictors of COVID-19-associated CVST in the univariate and multivariate analyses19,31-33. This is reasonable considering that CVST occurs in patients with severe COVID-194-7. This suggests the significance of maintaining vigilance for CVST to allow its early diagnosis and treatment in patients with COVID-19 who have pre-existing comorbidities or a history of smoking.
Regarding treatment options utilized for both sexes, unfractionated heparin was administered significantly more frequently to women than to men, with a rate of 63.2% (24 out of 38 patients). Some studies suggest sex-based treatment approach differences. A nationwide in-patient study from the United States on sex differences in the management of stroke patients found that alteplase treatment was administered significantly less often to women after adjusting for age, race, and other factors. 34 another nationwide in-patient sample database in the United States showed that for proximal deep venous thrombosis, catheter-directed thrombolysis was used less commonly in women than in men. 35 This showed that there might be some sex differences in the management of certain conditions, including CVST, which require further large-scale studies. In our study, when looking at either unfractionated heparin or low molecular weight heparin, they were received in total similarly (42 men vs 41 women), which could argue against any sex-based treatment approach differences. This further aligns with our daily practice, which is not associated with any differences when it comes to the choice of anticoagulation. This was studied using a step-wise approach in a prospective, national Australian Stroke Clinical Registry, which showed no difference between care provided to men and women. 36
Herein, the mortality rate was 21.3% (n = 46). This is higher than previous reports on CVST cases unrelated to COVID-19, which differ between studies; however, recent advances in treatment have decreased the mortality rate of CVST to below 5%24,37–40. This finding corroborates previous studies showing that CVST increases the risk of poor outcomes in patients with COVID-19. 20 The mortality rate observed in our study (21.3%) was lower compared with the findings reported in various prior studies, in which the mortality rate exceeded 35%.20,41–43 We believe that this is because of the higher number of cases included in this study; in addition, our study included patients with varying disease severity, ranging from mild to severe. This leads to a more representative population, as some studies only report severe COVID-19 cases that can potentially inflate the mortality rate. Mortality outcomes of patients with CVST and COVID-19 showed higher mortality rates among men (30 of 46 men; 65.2%). This can be attributed to the well-established risk of severe COVID-19 among men, which predisposes them to a higher likelihood of adverse outcomes. 19 Additionally, smoking, a known risk factor for developing severe COVID-19, was significantly more prevalent among men in our study. 31 Furthermore, previous reports of CVST without COVID-19 have shown that male sex is associated with a poorer prognosis.38,44 Furthermore, the presence of seizures, as demonstrated by Korathanakhun et al, 45 was identified as an independent predictor of mortality and was more prevalent among men here.
By analyzing survival outcomes using Kaplan–Meier curves and log-rank tests, several variables, including smoking, diabetes mellitus, hypertension, OCP use, different COVID-19 symptoms (such as fever and cough), different CVST symptoms (such as headache and seizure), and the need for intubation, were identified as significant predictors of poorer survival outcomes. These findings provide valuable insights into the factors influencing the survival of patients with CVST and may be useful for clinical decision-making. Additionally, our results further support the findings of prior studies that examined the association between various factors in COVID-19 and survival outcomes.31,46
This study has some limitations. As in any retrospective study, inherent bias may have been introduced. Additionally, there could have been variations in the accuracy, completeness, and reliability of the data owing to a reliance on available published data. Furthermore, although this study established an association between sex differences and different risk factors for COVID-19 and CVST, it did not establish a causal relationship. Future prospective studies or controlled trials are needed to explore causality and temporal dynamics.
Conclusion
This study examined the association between COVID-19 and CVST. Notable findings included sex differences in symptoms and outcomes, the impact of risk factors on CVST development, and a higher mortality rate among patients with CVST and COVID-19, especially in association with other risk factors. This study underscores the need to diagnose CVST early in patients with COVID-19, taking into consideration atypical presentations and risk factors, which can enhance the management of COVID-19-related CVST.
Supplemental Material
sj-docx-1-cat-10.1177_10760296241240748 - Supplemental material for Sex Differences and Clinical Outcomes of Patients with Coronavirus Disease 2019 Infection and Cerebral Venous Sinus Thrombosis: A Systematic Review
Supplemental material, sj-docx-1-cat-10.1177_10760296241240748 for Sex Differences and Clinical Outcomes of Patients with Coronavirus Disease 2019 Infection and Cerebral Venous Sinus Thrombosis: A Systematic Review by Saleh A. Algarni, Naif S. ALGhasab, Mohammed S. Alharbi, Anas Albarrak, Ahmad A. Alanezi and Hamdan M. Al Shehri in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-2-cat-10.1177_10760296241240748 - Supplemental material for Sex Differences and Clinical Outcomes of Patients with Coronavirus Disease 2019 Infection and Cerebral Venous Sinus Thrombosis: A Systematic Review
Supplemental material, sj-docx-2-cat-10.1177_10760296241240748 for Sex Differences and Clinical Outcomes of Patients with Coronavirus Disease 2019 Infection and Cerebral Venous Sinus Thrombosis: A Systematic Review by Saleh A. Algarni, Naif S. ALGhasab, Mohammed S. Alharbi, Anas Albarrak, Ahmad A. Alanezi and Hamdan M. Al Shehri in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
The authors acknowledged the effort and assistance of medical graduates, including Rahaf H. Almutairi, Abdullah Zaki Al-Fahd, Ahood Ahmad A Mahjari, and Hasan Mohammed Daghriri, College of Medicine, Imam Mohammad Ibn Saud Islamic University (IMSIU), Riyadh, Saudi Arabia.
Contributorship
Conceptualization was done by SA. Data curation was done by SA, MA, AA, HA, AAb, AAL, and NA. Methodology and data analysis were done by SA, MA, and NG. Writing—original draft was done by SA, NG, AA, MA, and AA. Writing—review and editing by SA and NA. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Decalaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable. The study did not involve any therapeutic intervention and was conducted following the Declaration of Helsinki after reviewing all other study approvals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor:
Saleh A. Algarni.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.