
Abstract
Cerebral venous sinus thrombosis (CVST) has become a rare but potentially life-threatening condition in perinatal women. Early and rapid identification of CVST in pregnant women is a challenge for frontline clinical workers. In this study, 40 perinatal patients with CVST in our hospital were included in the five-year period, and 120 normal perinatal pregnant women in the obstetrics and gynecology department of our hospital were randomly enrolled in the five-year period as the control group, including 60 cases in pregnancy and puerperium. 5 mL of fasting venous blood was collected from puerperal CVST patients in the acute phase of onset (within 72 h of onset) and the recovery phase (fourth week of treatment). In the control group, 5 mL of fasting venous blood was collected. Coagulation factors X, XI, and XII, plasma D-Dimer were analyzed and compared. Coagulation factors X, XI, and XII in plasma of CVST patients were significantly increased compared with controls. Plasma coagulation factors X, XI, and XII and their combined detection (Union Model = 0.056 * FX: C + 0.046 * FXI: C + 0.081 * FXII: C) have diagnostic values for perinatal CVST. Plasma coagulation factors X, XI, and XII were significantly positively correlated with plasma D-dimer levels in perinatal CVST patients. Plasma coagulation factors X, XI, and XII have diagnostic values for perinatal CVST.
Key Message
Plasma coagulation factors X, XI, and XII have diagnostic values for perinatal CVST.
Introduction
Cerebral venous sinus thrombosis (CVST) is a rare but potentially life-threatening condition that can occur in the perinatal state. 1 This condition is caused by the formation of a blood clot in the venous sinuses of the brain, which prevents the normal drainage of blood from the brain. 2 The most common symptom of CVST is a headache, but other signs and symptoms may include seizures, vomiting, altered mental status, and focal neurological deficits. 3 If left untreated, CVST can lead to serious complications, such as stroke, cerebral edema, and hydrocephalus.4,5
The exact cause of CVST is not known, but it is believed to be related to a combination of factors such as genetics, infection, and blood clotting disorders. 6 It has been hypothesized that the increased levels of hormones during pregnancy may contribute to increased clotting of the veins that drain blood from the brain, leading to clot formation. 7 The physiological mechanism of CVST during the perinatal period involves several factors that can lead to the formation of clots in the cerebral venous sinuses. 8 One of these factors is an imbalance in the hemostatic system, which is responsible for maintaining the balance between clotting and fibrinolysis.2,9 In this system, a balance between the production of clotting factors and plasminogen activator inhibitors (PAIs) is essential to prevent clot formation. 10 However, during the perinatal state, there is an increase in the production of clotting factors, such as Factor VIII, fibrinogen, and von Willebrand factor, which can lead to an imbalance in the hemostatic system and predispose to the formation of clots in the cerebral venous sinuses. 11
Early and rapid identification of CVST in pregnant women, correct diagnosis, and timely treatment are challenges faced by front-line clinical workers. 12 Therefore, this work aims to investigate the diagnostic value of coagulation factors X, XI, and XII for perinatal CVST, and the relationship between the 3 and the severity of the disease (D-D dimer level). We hope that our study can provide new theoretical evidence for early intervention of perinatal CVST.
Methods
Participants
This study included 40 perinatal CVST patients and 120 perinatal normal pregnant women (60 cases during pregnancy and 60 cases during puerperium) in our hospital. The study was approved by the ethics committee of Cangzhou Central Hospital.
Inclusion criteria for patients with CVST: Confirmed by diagnostic criteria for CVST; peripartum women. Exclusion criteria: patients with chronic hypertension, liver and kidney diseases, endocrine diseases, tumors; patients with nervous system diseases such as primary epilepsy and intracranial infection before pregnancy, and patients with organic diseases of the nervous system found by examination.
Diagnostic Criteria for CVST
The diagnostic criteria of CVST in this study were based on the 2011 American version of the AHA/ASA Stroke Association statement to medical professionals “Diagnosis and Management of Cerebral Venous Thrombosis.” Clinically, the patient had symptoms of high intracranial pressure such as headache, vomiting, blurred vision, and/or other neurological symptoms and signs. CVST findings were confirmed by digital subtraction angiography (DSA) or cranial magnetic resonance imaging (MRI) and magnetic resonance angiography (MRV). Imaging diagnosis was mainly based on the DSA examination showing that the intracranial venous sinuses and (or) veins were partially or completely absent, with or without the establishment of venous collateral circulation. For patients who had not undergone DSA examination, the diagnosis was based on the disappearance of venous sinus emptying phenomenon and thrombus signal on MRI examination combined with MRV.
Sample Collection
5 mL of fasting venous blood was collected from puerperal CVST patients in the acute phase of onset (within 72 h of onset) and the recovery phase (fourth week of treatment). In the control group, 5 mL of fasting venous blood was collected.
Factor Analysis
The coagulation factors X, XI, and XII in plasma were analyzed by SYSMEX CA-7000 automatic coagulation. Plasma D-D was determined by immunoturbidimetric method (normal reference value 0-0.5 mg/L).
Statistical Analysis
SPSS 13.0 statistical software was used for statistical analysis, and the measurement data conforming to the normal distribution were expressed as mean ± SD and 2 independent samples t test was used. Enumeration data were expressed as frequency or frequency, and the χ2 test was used. Taking the incidence of CVST in puerperium as the dependent variable (yes = 1, no = 0) and D-dimer as the independent variable, multivariate Logistic regression analysis was carried out. P < .05 means the difference is statistically significant.
Results
Clinical Characteristics of the Participants
This trial included 40 eligible CVST patients from the Department of Obstetrics and Gynecology of our hospital during the 5 years. A 1:3 ratio was used to randomly recruit 120 normal pregnant women as the control group, including 60 cases during pregnancy and puerperium. As shown in Table 1, there was no significant difference between the 2 groups in terms of age, parity, and presence of gestational diabetes, but there was a significant difference in the presence of preeclampsia between the 2 groups (P < .001). Among the 40 CVST patients, thrombus occurred in 21 cases in the transverse sinus, 14 cases in the superior sagittal sinus, 15 cases in the sigmoid sinus, and 7 cases in the straight sinus.
Clinical Characteristics of Women With Cerebral Venous Sinus Thrombosis (CVST) and Normal Controls (Control) During Perinatal State.
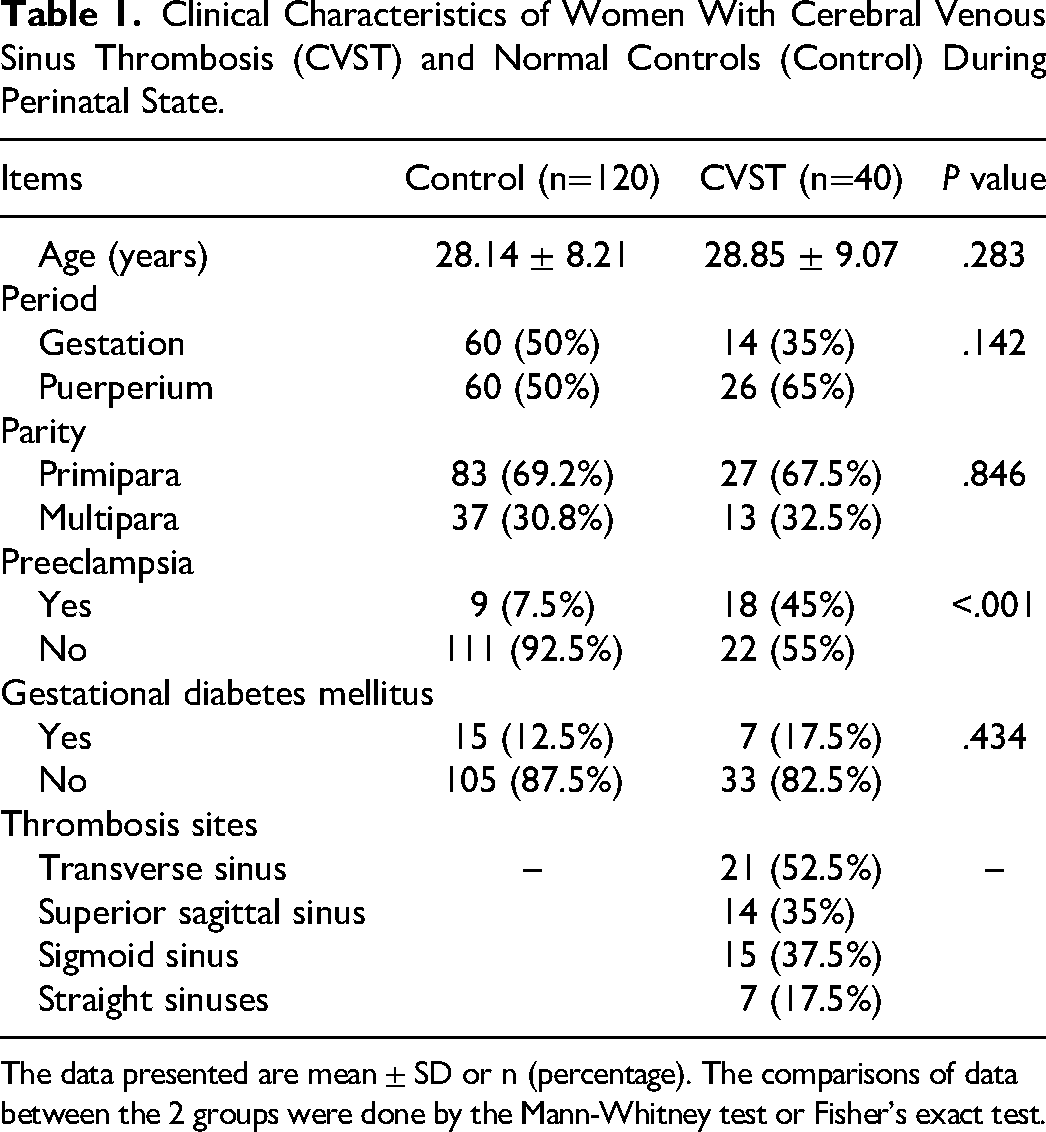
The data presented are mean ± SD or n (percentage). The comparisons of data between the 2 groups were done by the Mann-Whitney test or Fisher’s exact test.
Differences in Plasma Coagulation Factors X, XI, and XII
In order to explore the difference between CVST patients and normal parturients, we further compared the differences in plasma coagulation factors X, XI, and XII between the 2 groups. Our results showed that the plasma coagulation factors X (Figure 1A), XI (Figure 1B), and XII (Figure 1C) in CVST patients were significantly increased compared with the control group, with a significant difference (P < .001).
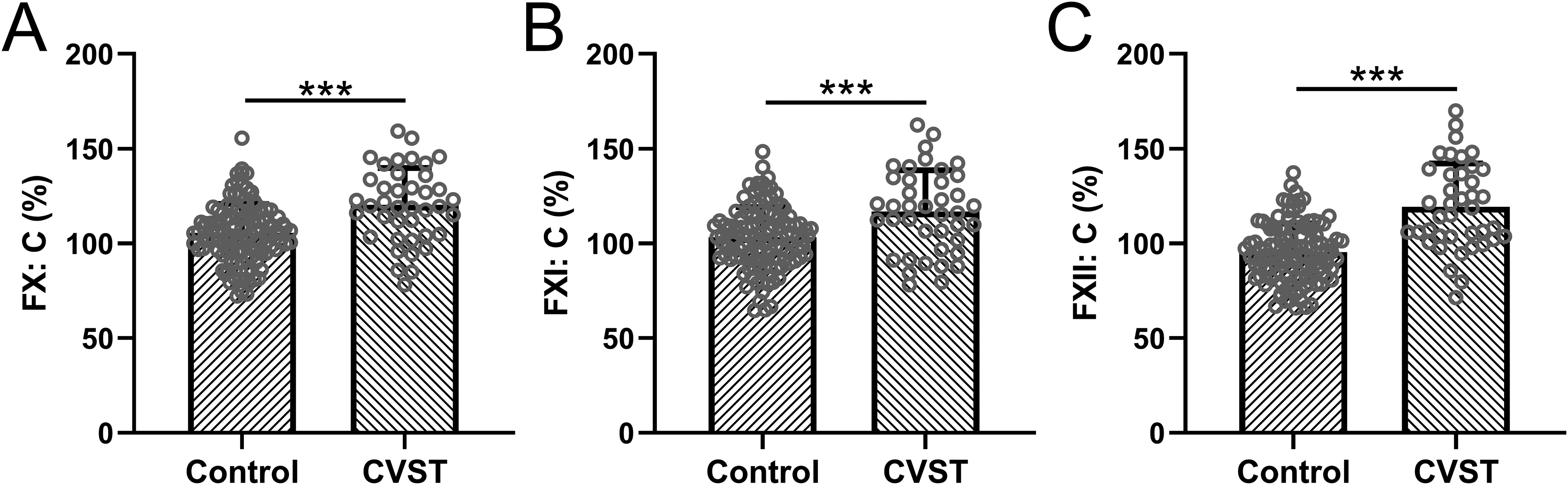
Comparisons of plasma coagulation factors X (A), XI (B), and XII (C) between women with cerebral venous sinus thrombosis (CVST, n = 40) and normal controls (control, n = 120) during perinatal state. Data were shown with mean ± SD. ***P < .001 from unpaired t test with Welch's correction.
Diagnostic Value of Plasma Coagulation Factors X, XI, and XII and Their Combined Detection for Perinatal CVST
We further analyzed the diagnostic values of plasma coagulation factors X, XI, and XII and their combination test for cerebral venous sinus thrombosis during perinatal state by receiver operating characteristic (ROC) analysis (Figure 2). As shown in Table 2, factor X (95% CI 0.63-0.83; sensitivity 67.5%; specificity 75.0%; Youden index 0.43; AUC 0.73), factor XI (95% CI 0.58-0.79; sensitivity 67.5%; specificity 69.2%; Youden index 0.37; AUC 0.69), and factor XII (95% CI 0.58-0.79; sensitivity 67.5%; specificity 69.2%; Youden index 0.37; AUC 0.69) were statistically predictive for perinatal CVST. Moreover, we formulated the Union Model = 0.056 * FX: C + 0.046 * FXI: C + 0.081 * FXII: C through the Youden index cut-off value, sensitivity, and specificity. We showed that the union model (95% CI 0.83-0.96; sensitivity 77.5%; specificity 94.2%; Youden index 0.72; AUC 0.90) has a higher diagnostic value for CVST.

Receiver operating characteristic (ROC) analysis of diagnostic values of plasma coagulation factors X, XI, XII, and their combination test for cerebral venous sinus thrombosis during perinatal state.
Diagnostic Values in ROC Analysis.

Abbreviations: CI, confidence interval; ROC, receiver operating characteristic; AUC, area under the receiver operating characteristic curve.
Union Model = 0.056 *FX: C + 0.046 *FXI: C + 0.081 *FXII: C.
Relationship Between Plasma Coagulation Factors X, XI, and XII and Plasma D-Dimer in CVST Patients
D-dimer is a specific degradation product formed by plasmin acting on cross-linked fibrin. It can be specifically increased when the blood in the body is in a hypercoagulable state or secondary fibrinolytic hyperfunction. 13 Under the special physiological state of pregnant and lying-in women, D-dimers may have different degrees of changes in gestational hypertension, gestational diabetes, and heart, brain, and renal vascular diseases. D-dimer can reflect the severity of CVST in patients to a certain extent. 14 Therefore, we analyzed the correlation between plasma coagulation factors X, XI, and XII and D-dimer in patients with CVST, and found that plasma coagulation factors X (Figure 3A), XI (Figure 3B), and XII (Figure 3C) were all significantly positively correlated with plasma D-dimer levels.

Pearson correlation analysis of plasma D-Dimer with coagulation factors X (A), XI (B), and XII (C) in women with cerebral venous sinus thrombosis (CVST, n = 40) during perinatal state.
Changes of Plasma Coagulation Factors X, XI, and XII in CVST Patients
We further analyzed the changes of plasma coagulation factors X, XI, and XII in 40 patients with perinatal CVST in the acute phase (within 72 h of onset) and recovery phase (fourth week of treatment). It can be seen that the patients after treatment, plasma coagulation factors X (Figure 4A), XI (Figure 4B), and XII (Figure 4C) were significantly reduced.

Changes of plasma coagulation factors X (A), XI (B), and XII (C) in women with cerebral venous sinus thrombosis (CVST, n = 40) during perinatal state at the time of acute stage and recovery stage. ***P < .001 from paired t test.
Discussion
CVST is a special type of cerebrovascular disease, which refers to the abnormal coagulation of blood in the intracranial venous sinus, resulting in partial or complete obstruction of the lumen. 15 The incidence of adult CVST is 0.5/100 000. However, the incidence of perinatal CVST is 20 to 900 times that of adults. The incidence of CVST during pregnancy and postpartum is about 11.6/100 000 in developed countries and 450/100 000 in developing countries. 11 Therefore, CVST is a common neurological emergency in pregnant women. 16 CVST has no specific clinical manifestations, which easily leads to delayed diagnosis and high mortality and disability rates. 17 With the popularity of MRI and the improvement of clinical awareness, the diagnosis rate of CVST is getting higher and higher. 18 However, there is still no reliable and simple biomarker to predict the occurrence of CVST, which brings some challenges to early diagnosis. 19
At present, the high-risk factors of CVST include thrombosis status (such as protein C deficiency, protein S deficiency, activated protein C resistance, and antithrombin III deficiency), antiphospholipid syndrome, hyperhomocysteinemia, pregnancy and puerperium, oral contraceptives, hormone replacement therapy, and tumors. 20 The existence of the above risk factors promotes vessel wall damage, hemodynamic abnormalities, and blood hypercoagulability as the main pathogenesis of CVST. 21 The pathogenesis and pathophysiology of pregnancy-associated CVST have not yet been fully elucidated. 22 It may be related to hypercoagulable state, blood stasis, vascular wall damage, and other factors. 23 Pregnancy and puerperium are special physiological stages for women, and corresponding pathophysiological changes occur in the blood coagulation system and anticoagulation system. 24 Due to changes in the internal environment of the human body before and after pregnancy, the risk of CVST increases during pregnancy and puerperium, and most of them occur in early pregnancy and 1 to 4 weeks after delivery. 25
Studies have found that patients with onset in early pregnancy are more susceptible to abnormal blood coagulation. 26 The increase of estrogen level and the increase of procoagulants such as von Willebrand factor, fibrinogen, and blood coagulation factors (I, VII, VIII, IX, X, and XII) make the blood hypercoagulable state. A study from Spain enrolled 240 female patients with cerebrovascular disease events during pregnancy, up to 136 cases (56.7%) developed CVST, of which 30% occurred during pregnancy and 64% occurred after delivery. CVST mostly occurs in the first trimester of pregnancy and 2 to 3 weeks after delivery. 27 They reported that the specific mechanism of the high incidence of CVST during pregnancy may be related to a large loss of body fluid, decreased circulating blood volume, blood stasis, hypercoagulable state, vascular endothelial injury, postpartum infection, vascular wall injury and changes in blood components. 27
In this study, we attempted to use coagulation factors X, XI, and XII and their combined prediction model to predict the occurrence of CVST early in the perinatal period. We analyzed 40 patients with perinatal CVST, and their thrombus occurred in 21 cases in the transverse sinus, 14 cases in the superior sagittal sinus, 15 cases in the sigmoid sinus, and 7 cases in the straight sinus. Compared with controls, more patients with perinatal CVST developed symptoms of preeclampsia before CVST diagnosis. We believe that the pathogenesis of preeclampsia involves abnormal blood coagulation and increased oxidative stress in pregnant women, which has some overlap with the pathology of CVST. However, due to time and number of patients, we did not analyze whether the occurrence of eclampsia was associated with the occurrence of perinatal CVST. We hope to analyze the relationship between these 2 diseases by including more patients in a multicenter study.
Consistent with many previous studies, we found that plasma coagulation factors X, XI, and XII were significantly elevated in patients with CVST, compared with controls. We further analyzed the early predictive value of coagulation factors X, XI, and XII for the onset of perinatal CVST by ROC analysis. Our results suggest that plasma coagulation factors X, XI, and XII have statistical value in the diagnosis of perinatal CVST. We further designed a joint detection model through Youden analysis and statistical software: Union Model = 0.056 * FX: C + 0.046 * FXI: C + 0.081 * FXII: C. We found that our CVST joint prediction model can effectively improve the prediction accuracy and specificity. Also, in CVST. D-dimer can reflect the disease severity of patients to a certain extent. Therefore, we further analyzed the correlation between plasma coagulation factors X, XI, and XII and D-dimer in CVST patients in this study. Plasma coagulation factors X, XI, and XII were significantly positively correlated with plasma D-dimer levels. To a certain extent, it shows that plasma coagulation factors X, XI, and XII are positively correlated with the severity of CVST disease.
Conclusions
In conclusion, we demonstrate that coagulation factors X, XI, and XII are of specific value for the diagnosis of perinatal CVST. We hope that our research can provide new auxiliary means for the early diagnosis of clinical CVST.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
The study was approved by the ethics committee of Cangzhou Central Hospital. The study was performed in strict accordance with the Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Cangzhou Science & Technology Project (222106096).
Informed Consent
All participants in this study were informed and gave written consent.