
Abstract
Background:
Endovascular treatment of cerebral venous sinus thrombosis (CVST) includes pharmacological and mechanical thrombolysis.
Methods:
The authors searched the English literature on CVST from 1990 to 2012 for all case reports or case series of mechanical thrombectomy.
Results:
A total of 64 patients were treated in all published studies. The techniques for mechanical thrombectomy included rheolytic thrombectomy with an AngioJet device (46.9%), clot retraction with the Penumbra system (4.7%), clot retraction with a Fogarty catheter (1.6%), clot retraction with a microsnare (3.1%), balloon venoplasty without stenting (18.7%), balloon venoplasty with stenting (4.7%), and an amalgam of techniques (18.7%). Nine (16.1%) patients died. At the most recent follow-up, 40 (62.5%) patients had no disability or minor disability and 7 (10.9%) patients had major disability.
Conclusion:
Randomized multiinstitutional clinical trials with larger number of participants are needed to sufficiently compare the effect of intrasinus thrombolysis and mechanical thrombectomy to standard-of-care anticoagulation therapy.
Keywords
Introduction
Cerebral venous sinus thrombosis (CVST) has an “all or none” prognosis. If the patient is treated adequately and survives the acute phase, the long-term prognosis will generally be satisfactory. 1 Currently, the acute phase of CVST is usually treated with unfractioned or low-molecular-weight heparin. 2 In the early 1990s, some neurosurgeons delivered anticoagulants to the superior sagittal sinus through a catheter to the internal jugular vein. 3 Mechanical thrombolysis was initially assayed in animal studies. 4
The endovascular treatment of CVST includes pharmacological thrombolysis and mechanical thrombectomy. In pharmacological thrombolysis, under fluoroscopic guidance a microcatheter is advanced via a retrograde approach to the cerebral dural sinuses and thrombolytic agents such as tissue plasminogen activator or urokinase are administered as a bolus or with infusion over a period of time. Mechanical thrombectomy is done with different types of catheters, balloons, stents, or snares to disrupt acute phase versus acute over chronic thrombus. Pharmacological and mechanical thrombolysis can be performed simultaneously or successively. 5 –12
Lack of optimal efficacy of systemic anticoagulation as standard therapeutic regimen for CVST in some patients and paucity of the medical literature which critically appraise the advantage and shortcomings of mechanical thrombectomy made us to provide this review. The objective of this study is to systematically review the literature to identify published reports (case reports or case series) of mechanical thrombolysis with or without the use of thrombolytic agents in patients with CVST.
Thrombectomy Techniques
The different techniques that have been used to date and that were considered in this review are described briefly below.
Rheolytic Thrombectomy
Rheolytic thrombectomy is based upon Bernoulli principle, according to which increasing speed of a fluid in a conduit causes a decrease in pressure. This technique is applied via a rheolytic catheter by inducing a vacuum with the rapid infusion of saline solution. The most commonly used rheolytic system is the Angiojet system (Medrad Inc, Warrendale, Pennsylvania). An over-the-wire catheter with multiple outflow pores produces a saline jet of approximately 2500 to 9000 psi and a second inflow lumen is used for aspiration of the thrombus. 6,11 Old systems used a 5-F catheter or larger, but recently a 4-F catheter system was launched. The rheolytic catheter should be introduced over a 7-F or an 8-F guiding catheter. Clot fragmentation can be achieved both by to and fro movements of the microguide wire and by suction through the rheolytic catheter. 13
Balloon Angioplasty or Stenting
Balloon catheters can expand to macerate the venous thrombus 7 or be inflated distal to thrombus and pulled back to aspirate the thrombus. 12 Balloon angioplasty has also been utilized in pediatric CVST. 10 Angioplasty has the advantage over rheolytic thrombectomy in that the former method can dilate the stenotic lesions, which predisposes to venous thrombosis. 6 Stenting of the thrombus site can be done after angioplasty. 8
Microsnare
To the best of our knowledge, only one report has been published on the combined use of intrasinus infusion of urokinase and mechanical thrombectomy with a microsnare device. 5 Repeated pulling of the microsnare through the clot may increase the surface area of the thrombus exposed to the thrombolytic drug.
Penumbra System
The Penumbra system (Penumbra Inc, Alameda, California) has 2 main components, an aspirating catheter and a separator. Repeated to and fro movement of the separator is used to debulk the thrombus, and negative pressure produced by a vacuum system connected to the catheter is used for continuous aspiration. 14,15
Fogarty Embolectomy Catheter Balloon
The Fogarty percutaneous embolectomy catheter balloon (Edwards Lifesciences Corp, Irvine) is used to remove fresh soft arterial thrombus material. Older reports described successful clot retraction with a Fogarty balloon catheter after continuous urokinase infusion. 9 This procedure is associated with risk of pulmonary embolism. 9
Materials and Methods
Selection Criteria
The authors searched the Institute for Scientific Information (ISI) Web of Knowledge, MEDLINE (National Library of Medicine), and Scopus databases, as 3 major scientific search engines, from 1990 to 2012. They used the following MeSH keywords as search terms: “cerebral venous sinus thrombosis,” “cerebral venous thrombosis,” “thrombectomy,” “rheolytic,” “endovascular,” and “interventional.” We also searched the reference lists of articles identified by this search strategy and selected those we judged relevant. Only studies published in English were included.
Data Collection
The thrombectomy techniques in this review included rheolytic thrombectomy, clot retraction by Fogarty balloon catheter or microsnare, angioplasty with or without stenting, and suction thrombectomy (Penumbra system). Each article was read to extract data on demographic characteristics (age and sex), type of CVST (septic vs nonseptic), and predisposing factors. Clinical manifestations were recorded, particularly the time elapsed between the first neurological manifestations and thrombectomy, signs of herniation at the time of thrombectomy, and the administration of heparin at the time of thrombectomy. Radiological features such as the presence of infarction or hemorrhage in computed tomography scans or magnetic resonance imaging scans of the brain at the time of thrombectomy were noted. We also recorded whether the articles reported the sinuses involved according to angiographic findings.
The indications for thrombectomy were recorded in 4 main categories (1) deterioration of mental status or early coma, (2) progression of neurological deficits other than level of consciousness, (3) persistent thrombosis documented angiographically without clinical deterioration, and (4) mixed pattern. 2
Technical aspects that were taken into account were the site of catheter insertion (internal jugular vein vs common femoral vein), technical success in reaching the target vessel, and whether recanalization was total or partial. Any complications reported were also noted.
Any available follow-up data were extracted from the reviewed articles. Mortality and morbidity during the hospital stay and follow-up period were recorded. The patients’ scores on the modified Rankin scale (mRS) 16 on their most recent follow-up visits were recorded.
Statistical Analysis
Statistical analyses were done with SPSS software, version 16.0 (SPSS Inc, Chicago, Illinois). Chi-squared or Fisher exact tests were used to compare the frequencies of clinical and radiologic findings in alive and dead patients in order to find the poor prognostic factors. Data are reported as mean ± standard deviation or proportions as appropriate. A 2-tailed P value less than .05 was considered statistically significant.
Results
Information for 28 (43.8%) of the 64 patients included in this review came from case reports or case series that comprised fewer than 5 patients. The remaining 36 (56.2%) patients were treated at centers that had more experience with CVST and published case series comprising 5 or more patients. Table 1 and 2 summarizes the data extracted from all studies included in this review.
Articles Included in This Review (Part 1).a
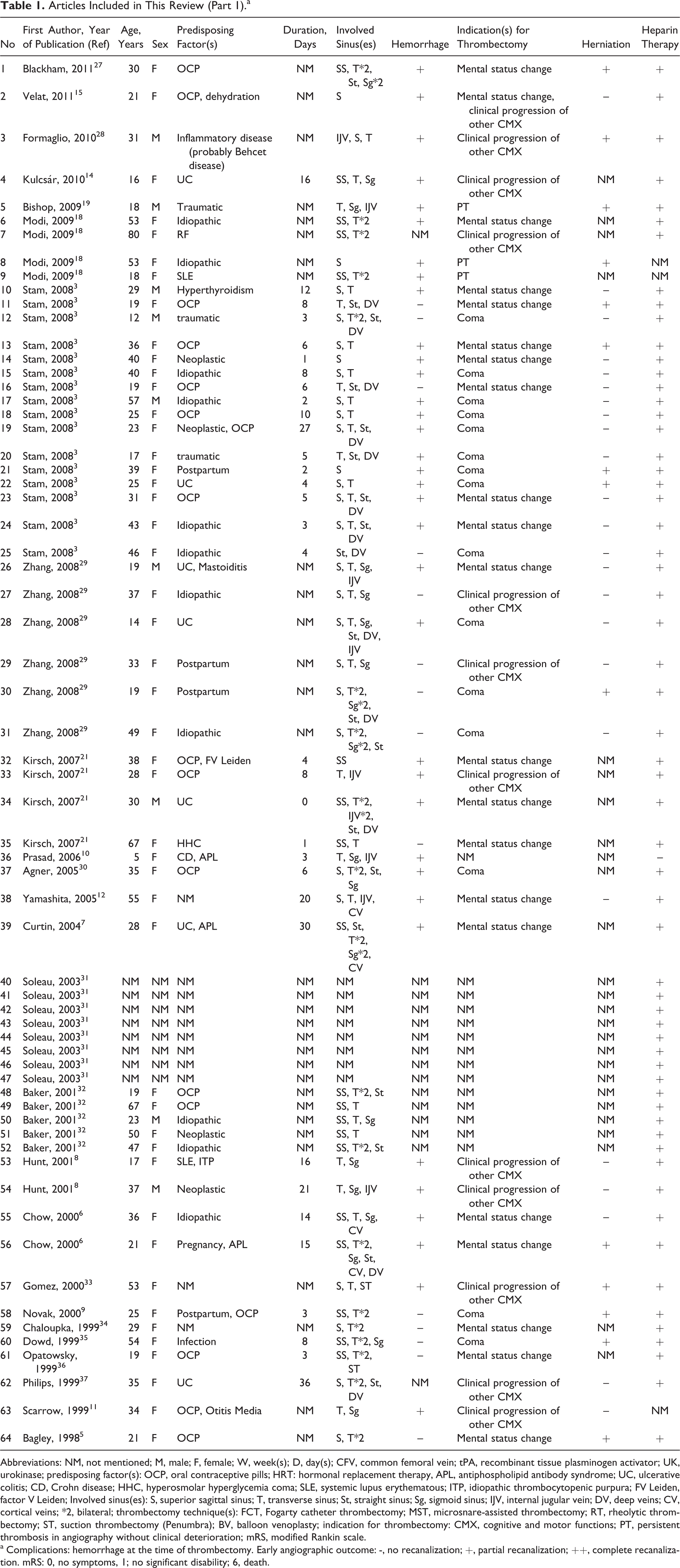
Abbreviations: NM, not mentioned; M, male; F, female; W, week(s); D, day(s); CFV, common femoral vein; tPA, recombinant tissue plasminogen activator; UK, urokinase; predisposing factor(s): OCP, oral contraceptive pills; HRT: hormonal replacement therapy, APL, antiphospholipid antibody syndrome; UC, ulcerative colitis; CD, Crohn disease; HHC, hyperosmolar hyperglycemia coma; SLE, systemic lupus erythematous; ITP, idiopathic thrombocytopenic purpura; FV Leiden, factor V Leiden; Involved sinus(es): S, superior sagittal sinus; T, transverse sinus; St, straight sinus; Sg, sigmoid sinus; IJV, internal jugular vein; DV, deep veins; CV, cortical veins; *2, bilateral; thrombectomy technique(s): FCT, Fogarty catheter thrombectomy; MST, microsnare-assisted thrombectomy; RT, rheolytic thrombectomy; ST, suction thrombectomy (Penumbra); BV, balloon venoplasty; indication for thrombectomy: CMX, cognitive and motor functions; PT, persistent thrombosis in angiography without clinical deterioration; mRS, modified Rankin scale.
a Complications: hemorrhage at the time of thrombectomy. Early angiographic outcome: -, no recanalization; +, partial recanalization; ++, complete recanalization. mRS: 0, no symptoms, 1; no significant disability; 6, death.
Articles Included in This Review (Part 2).a
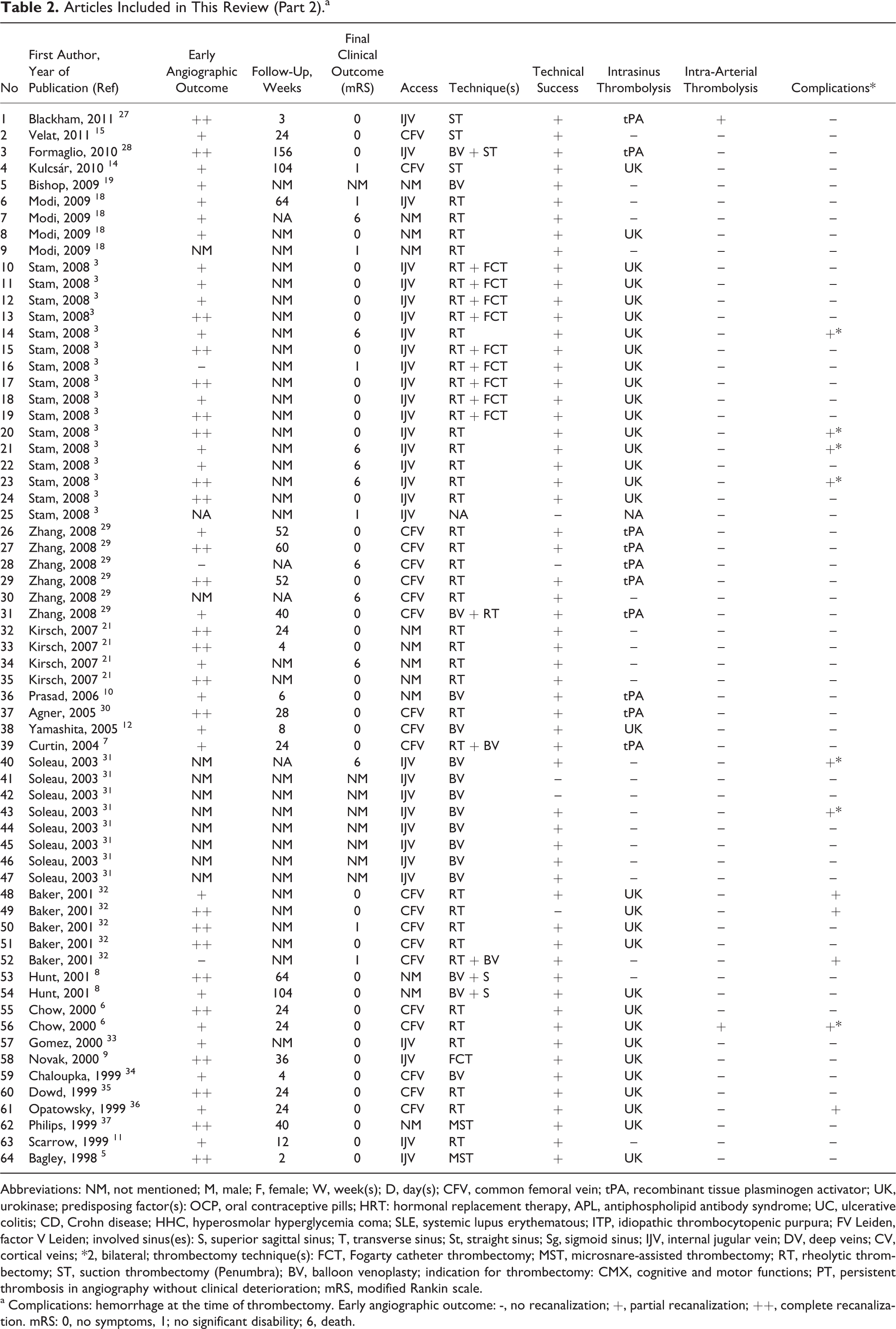
Abbreviations: NM, not mentioned; M, male; F, female; W, week(s); D, day(s); CFV, common femoral vein; tPA, recombinant tissue plasminogen activator; UK, urokinase; predisposing factor(s): OCP, oral contraceptive pills; HRT: hormonal replacement therapy, APL, antiphospholipid antibody syndrome; UC, ulcerative colitis; CD, Crohn disease; HHC, hyperosmolar hyperglycemia coma; SLE, systemic lupus erythematous; ITP, idiopathic thrombocytopenic purpura; FV Leiden, factor V Leiden; involved sinus(es): S, superior sagittal sinus; T, transverse sinus; St, straight sinus; Sg, sigmoid sinus; IJV, internal jugular vein; DV, deep veins; CV, cortical veins; *2, bilateral; thrombectomy technique(s): FCT, Fogarty catheter thrombectomy; MST, microsnare-assisted thrombectomy; RT, rheolytic thrombectomy; ST, suction thrombectomy (Penumbra); BV, balloon venoplasty; indication for thrombectomy: CMX, cognitive and motor functions; PT, persistent thrombosis in angiography without clinical deterioration; mRS, modified Rankin scale.
a Complications: hemorrhage at the time of thrombectomy. Early angiographic outcome: -, no recanalization; +, partial recanalization; ++, complete recanalization. mRS: 0, no symptoms, 1; no significant disability; 6, death.
Of the 64 patients, 47 (73.4%) were females and 9 (14.1%) were males. There were no data regarding age and sex for 8 (12.5%) patients. Mean age of the patients was 33.3 ± 15.6 years. One (1.6%) patient had septic CVST and all others (98.4%) had nonseptic CVST. Mechanical thrombectomy was done between 0 and 36 days (mean 9.3 ± 8.9) after the symptoms appeared. The most frequent etiology of CVST was oral contraceptive use and hormonal replacement therapy (12 patients, 18.8%) followed by inflammatory diseases (7 patients, 10.9%). Neoplastic disorders, postpartum status, injury, dehydration, and metabolic causes were reported in 3 (4.7%) patients each. In 10 (15.6%) patients, multiple predisposing factors were present, whereas in 11 (17.2%) patients no specific underlying cause was reported. There were no data on the etiology in 11 (17.2%) patients.
In most patients, multiple sinuses were involved (n = 51, 79.7%) and only 5 (7.8%) patients had single sinus involvement. In 8 (12.5%) patients the sinuses involved were not reported. The sites of involvement were the superior sagittal sinus (n = 46, 71.9%), transverse sinus (unilateral: n = 29, 45.3%, bilateral: n = 19, 29.7%), straight sinus (n = 23, 35.9%), sigmoid sinus (unilateral: n = 15, 23.4%, bilateral: n = 14, 21.9%), internal jugular vein (unilateral: n = 8, 12.5%, bilateral: n = 1, 1.6%), deep cerebral vein (n = 12, 18.8%), and cortical vein (n = 5, 7.8%).
In 31 (48.4%) patients, intraparenchymal hemorrhage was present at the time of thrombectomy. In 18 (28.1%) patients, there was no hemorrhage. In the rest of the patients (n = 15, 23.4%), no information was provided regarding the presence or absence of hemorrhage. In 14 (21.9%) patients, signs of cerebral herniation were present at the time of thrombectomy.
In all, 60 (93.8%) patients received intravenous heparin and heparin was not used in 1 (1.6%) patient. In 3 (4.7%) patients, no information was given concerning the heparin use.
The indications for thrombectomy had to be modified due to mental status (n = 14, 21.9%), coma (n = 14, 21.9%), progression of neurological deficits other than level of consciousness (n = 10, 15.6%), and persistent thrombosis on angiography without clinical deterioration (n = 3, 4.7%). Two or three of the above factors were present in 9 (14.1%) patients. In 14 (21.9%) patients no indication for mechanical thrombectomy was mentioned.
In 26 (40.6%) patients, the procedure was done via common femoral vein access and in 29 (45.3%) patients, the procedure was done via the internal jugular vein. In 9 (14.1%) patients, the site of access was not mentioned.
Regarding the method of thrombectomy, 30 (46.9%) patients had rheolytic thrombectomy with an Angiojet device and 3 (4.7%) patients underwent clot retraction with the Penumbra system. One (1.6%) patient underwent clot retraction with a Fogarty catheter. In 2 (3.1%) patients, microsnare clot retraction was done. Balloon venolplasty without stenting was used in 12 (18.7%) patients. Balloon venoplasty with stenting was done in 3 (4.7%) patients. In 12 (18.7%) patients, an amalgam of techniques was used, rheolytic thrombectomy with Fogarty clot retraction in 9 (14.1%) patients, and rheolytic thrombectomy with balloon venoplasty in 3 (4.7%) patients. In 1 (1.6%) patient, the technique of mechanical thrombectomy was not mentioned. For the entire patients included in this review, the overall rate of technical success was 92.2% (59 patients).
Concomitant intrasinus pharmacological thrombolysis was done in 41 (64.1%) patients. In 1 (1.6%) patient, concomitant intra-arterial thrombolysis was associated with thrombectomy.
After the thrombectomy procedure, partial angiographic recanalization was reported in 24 (37.5%) patients and complete recanalization in 26 (40.6%) patients. In 3 (4.7%) patients, recanalization was unsuccessful.
Complications were reported in 9 (14.1%) patients and 9 (14.1%) of the patients had died by the time the report was written. Mean follow-up time was 28.3 weeks. In their most recent follow-up, 40 (62.5%) patients had a mRS score of 0, 1, and 2 and 7 (10.9%) patients had a score of 3, 4, and 5. Data regarding the final clinical outcome were not available for 8 (12.5%) patients.
Poor prognostic factors mentioned in the articles we reviewed included stupor or coma at the time of admission (P < .001) and parenchymal hemorrhage with or without subarachnoid hemorrhage in the first computed tomography scan (P = .005).
Discussion
Although anticoagulation therapy is the most widely accepted therapeutic option for CVST, some researchers believe it may not be the best choice for all patients and each patient needs to be individualized based on their presentation. 17 Theoretically, mechanical thrombectomy appears to be an ideal treatment option for CVST. One reason is that the diameter of the cerebral dural sinuses is larger and consequently the venous thrombi are also larger. 6 Thus, intrasinus thrombolysis is considerably more time-consuming when compared to intra-arterial thrombolysis. 6,18 In contrast, mechanical thrombectomy has an immediate effect and can decrease intracranial pressure much more promptly. 19 Moreover, vessel dissection risks are minimal when dealing with thicker dural wall sinuses. It is also noted that intrasinus thrombolysis may trigger or aggravate hemorrhagic transformation in CVST-induced infarctions. 20
These factors favor mechanical thrombectomy over intrasinus thrombolysis alone. In combined pharmacological and mechanical thrombectomy, the dose of the thrombolytic drug and duration of infusion can be decreased because of the increased surface area of the thrombus exposed to the drug. 5,10
The limitations and disadvantages of mechanical thrombectomy should nonetheless be kept in mind. For example, the higher cost of mechanical thrombectomy equipment needs to be considered, especially in developing countries where CVST is prevalent. Technically, utilizing this modality is more demanding to operating surgeons thus more training and over sight becomes necessary. The danger of perforating the vessel remains a concern. Hemorrhagic transformation when thrombolytic therapy and thrombectomy are used together can be a life-threatening complication. Fluid overload can be a complication with the Angiojet system. 21 The inherent thrombogenic activity of mechanical devices should also be kept in mind. 4 Decreasing the diameter and increasing the torquability of thrombectomy devices may improve their function in the future. 6,11 Let us not to forget that access site complications including hematoma, soft tissue infections, iatrogenic arteriovenous fistula formation, peripheral nerve injuries, and perioperative anesthesia risks are added to this technique as any other endovascular modality.
According to our review of all published cases, the different mechanical thrombectomy techniques used to date were feasible and safe. Most patients showed good radiological recanalization and a satisfactory final clinical outcome. However, these results should be interpreted with caution because of the potential confounding effect of publication bias. Publication bias should be carefully considered, especially when new techniques become widespread quickly. 22 Researchers and clinicians tend to publish positive-outcome reports, and journal editors’ preference for positive findings can also exaggerate the real efficacy under some circumstances. 22 In this review, in addition to a single report of failed treatment, 23 we also considered a variety of different techniques for mechanical thrombectomy instead of focusing on 1 technique. This should increase the reliability of our conclusions. However, because of the limited number of patients treated with each technique, head-to-head comparisons between different techniques were impossible. Also, optimal follow-up methods and how long patients have to consume oral anticoagulants need to be investigated further.
Although comparison of the results of the current collection of the case studies with prospective observational studies such as International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT) is impossible, to put results of current series and ISCVT together could be helpful. In all, 94% of the patients in the current series and 83% in the ISCVT received anticoagulation, and 62.5% of the patients in the current series and 87% in the ISCVT had no or minor impairment (mRS: 0-2). Meanwhile, 14% of the patients in current series and 8.3% in the ISCVT died. 1 It should be kept in mind that the patients included in the current series had more dismal conditions at the time of the mechanical thrombectomy which naturally deviate their final outcomes to more grave states. Our results were in accordance with the results of ISCVT which distinguished coma and hemorrhage on admission computed tomography scans as the predictors of poor clinical outcome. 1 Although 12 (18.8%) patients had the involvement of the deep cerebral veins in the current series, it was not statistically significant for predicting mortality probably due to small number of patients.
Recommendations and Future Direction
The variable natural history of CVST poses a substantial obstacle to the development of optimal user-friendly guidelines for initiating intrasinus thrombolysis or mechanical clot disruption. To the best of our knowledge, there have been no randomized clinical trials designed to compare the effect of intrasinus thrombolysis or mechanical thrombectomy to standard-of-care anticoagulation. 24 Randomized, prospective, and multi-institutional clinical trials with larger number of participants are needed to sufficiently compare the effect of intrasinus thrombolysis and mechanical thrombectomy to standard-of-care anticoagulation therapy.
Until such research is available, mechanical thrombectomy with or without thrombolysis should be done as an off-label option for patients with CVST who deteriorate despite heparin therapy or patients with expectable poor prognosis. 25,26
This policy should be limited to the centers with optimal standards of logistics and interventional expertise.
Footnotes
Acknowledgments
We thank K. Shashok (Author AID in the Eastern Mediterranean) for improving the use of English in the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.