
Abstract
Cerebral venous sinus thrombosis (CVST) is an uncommon disease in childhood. In the largest study carried out so far, the incidence was 0.67 case per 100 000 children per year. A number of etiologies and risk factors have been so far identified for CVST in childhood, including head trauma, local and systemic infectious diseases, malignancies, and autoimmune diseases. Celiac disease (CD) is a disease of the small intestine caused by an immune response to ingested gluten. Epilepsy, bilateral occipital calcification, cerebellar ataxia, degenerative central nervous system disease, peripheric neuropathy, myopathy, and rarely stroke were defined as neurologic disorders. In this presentation, we report 2 cases (16-year-old boy and 2-year-old boy) with CD and CVST. We emphasized that CD can be investigated in patients with CVST even with the absence of gastrointestinal symptoms. Finally, we suggest that algorithm of CVST can be involved in the investigation of CD.
Introduction
Cerebral venous sinus thrombosis (CVST) is an uncommon disease in childhood. In the largest study carried out so far, the incidence was 0.67 case per 100 000 children per year. 1 Nowadays diagnosis is more rapid and precise than in the past because of magnetic resonance imaging (MRI) or MR angiography, and treatment may benefit from anticoagulant therapy. A number of etiologies and risk factors have been so far identified for CVST in childhood, including head trauma, local and systemic infectious diseases, malignancies, and autoimmune diseases. 1
Celiac disease (CD) is a disease of the small intestine caused by an immune response to ingested gluten. This response results in characteristic damage to the villi, leading to malabsorption. 2 Neurological symptoms without malabsorption signs have been defined for a long time in CD. Epilepsy, bilateral occipital calcification, cerebellar ataxia, degenerative central nervous system disease, peripherial neuropathy, myopathy, and rarely stroke were defined as neurologic disorders. 2 In this article, we report 2 cases of CVST in whom CD was diagnosed as the underlying disease because of unusual presentation. To the best of our knowledge, the association between CVST and CD has never been reported in children.
Case Reports
Case 1
A 16-year-old boy was admitted with headache and vomiting lasting for 3 days. Personal and family history was unremarkable. Both body weight and height were between 25 and 50 percentile. Vital signs were normal except for borderline hypertension. On physical examination, lethargy, brisk deep tendon reflexes, and positive meningeal irritation signs were noted. On laboratory analysis, complete blood count (CBC) was normal. Serum electrolytes, serum glucose, liver and renal function tests, cholesterol and triglyceride levels, and thyroid hormone values were within normal ranges. C-reactive protein was negative and erythrocyte sedimentation rate was 17 mm/h. Serum vitamin B12, folate, prothrombin time (PT), activated partial thromboplastin time (aPTT), fibrinogen, proteins C and S, factors V, VII, VIII, XII, and antithrombin III were within normal ranges. Serologic tests for brucella, salmonella, lupus anticoagulants, antinuclear antibody, anticardiolipin antibodies IgG and IgM were negative. Factor V Leiden and prothrombin GA20210 mutations were not detected. Tandem mass spectrophotometry and detailed blood carnitine profile were normal. Homocysteine level was 9.66 µmol/L (normal: 5-12 µmol/L). While anti-tissue transglutaminase IgA and IgG, anti-endomysium IgA were positive, pathologic examinations of intestinal tissue were consisted with CD. Intestinal biopsy showed villous atrophy with hyperplasia of the crypts and lympho-plasmocyter cells infiltration in lamina propria and increased intraepithelial lymphocyte count (above 40%; Marsh type 3c). Cardiac MRI and transthoracic echocardiographic examinations were normal. Ultrasonographic examinations of abdomen and urinary systems were normal. On cerebral MR venography, thromboses on superior and inferior sagittal sinuses, left transverse and sigmoid sinuses were seen (Figure 1 ). Additionally, common vascular collaterals were determined on cerebrum. Cerebrospinal fluid (CSF) examinations were normal except elevated CSF pressure (20 cm H2O). Cerebrospinal fluid and blood cultures were unremarkable. On fundoscopic examination, papilledema was also observed.
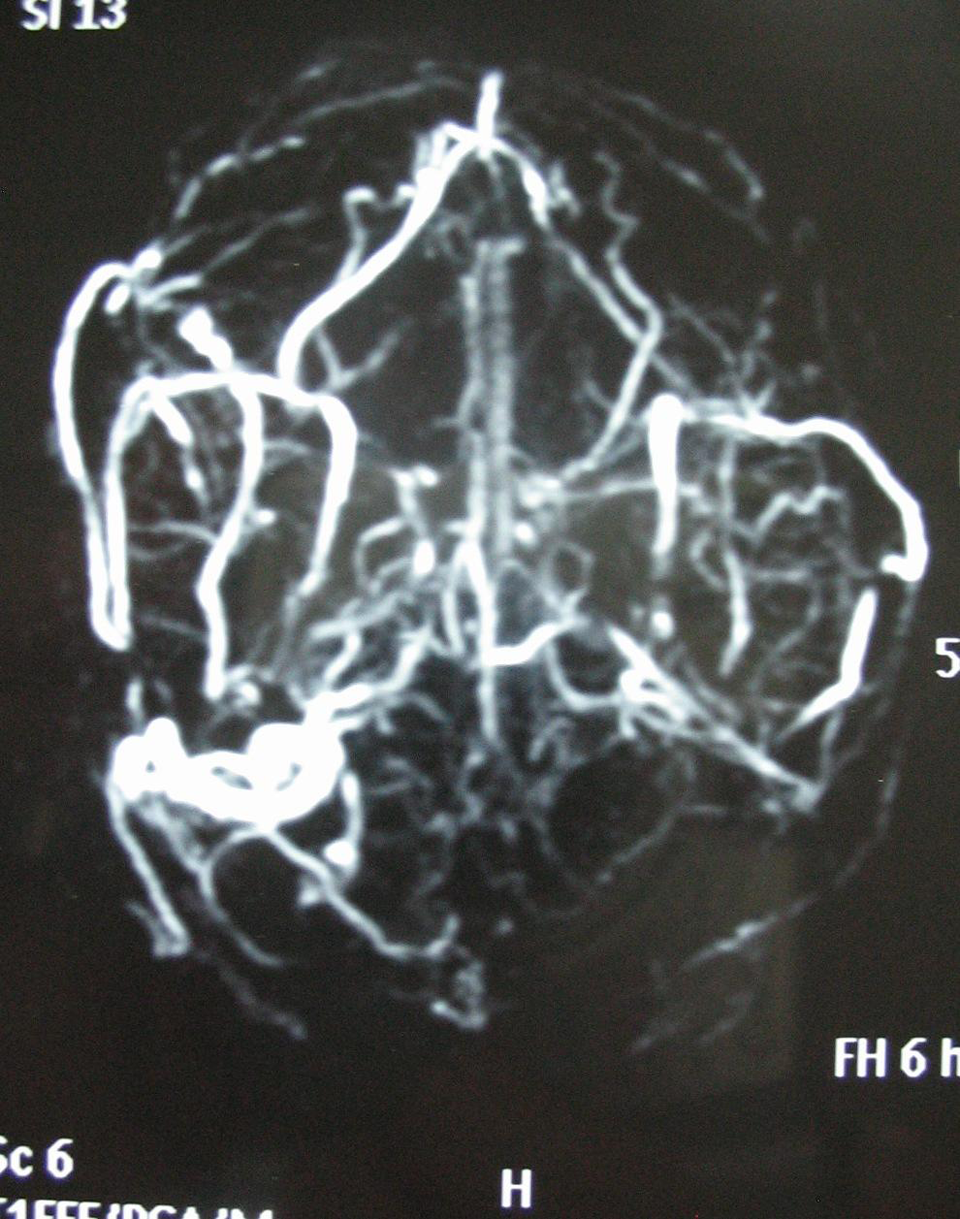
Cerebral magnetic resonance venography of case 1 shows thromboses on superior and inferior sagittal sinuses, left transverse, and sigmoid sinuses
The patient was hospitalized with the diagnoses of CVST, borderline hypertension, and pseudotumor cerebri due to CVST. On follow-up, nadroparin calcium, acetazolamide, and prednisolone were administered. After the intestinal biopsy, gluten-free diet was assayed for CD. On 11th day of hospitalization, the patient, whose symptoms regressed, was discharged with gluten-free diet and nadroparin calcium. Currently, he is on the second month of follow-up and symptom free.
Case 2
A 2-year-old boy was admitted to emergency department with irritability and vomiting lasting for 2 days. On previous history, abdominal distention, which had begun after the start of nutrition other than breast milk, was noted. Family history was unremarkable. Both body weight and height were 25 percentile. Vital signs were normal. On physical examination, lethargy, brisk deep tendon reflexes, and positive meningeal irritation signs were noted. On laboratory analysis, complete blood count was normal. Serum electrolytes, serum glucose, liver and renal function tests, cholesterol, triglyceride levels, and thyroid hormone values were within normal ranges. C-reactive protein was negative, erythrocyte sedimentation rate was 14 mm/h. Serum vitamin B12 and folate levels were normal. Prothrombin time and aPTT were 13.5 seconds (normal: 11-14 seconds) and 32 seconds (normal: 30-40 seconds), respectively. Fibrinogen, proteins C and S, factors V, VII, VIII, XII, and antithrombin III were within normal ranges. Serologic tests for brucella, salmonella, lupus anticoagulants, antinuclear antibody, anticardiolipin antibodies, IgG, and IgM were negative. Factor V Leiden and prothrombin GA20210 mutations were not detected. Tandem mass spectrophotometry and detailed blood carnitine profile were normal. Homocysteine level was 8 µmol/L (normal: 5-12 µmol/L). Antitissue transglutaminase IgA and IgG, anti-endomysium IgA were positive. In our center, duodenal biopsy could be performed only children aged older than 5 years. Therefore, in this patient, intestinal biopsy could not be performed because of younger age. Transthoracic echocardiographic examination was normal. Ultrasonographic examinations of abdomen and urinary systems were normal. On cranial MRI (Figure 2 ) and cerebral MR venography, thrombosis on right transverse sinuses was seen. Cerebrospinal fluid examinations were normal. The patient was hospitalized with the diagnoses of CVST and CD. On follow-up, nadroparin calcium was administered and gluten-free diet was assayed. On 12th day of hospitalization, the patient, whose symptoms regressed, was discharged with gluten-free diet and nadroparin calcium. Currently, he is on the sixth month of follow-up and symptom free. Abdominal distention was not seen thereafter.

Cranial magnetic resonance imaging of case 2 shows the thrombosis on right transverse sinuses.
Discussion
Cerebral venous sinus thrombosis is an uncommon disease in childhood. Infants less than 1 year of age comprise half the cases. Neonatal CVST has an estimated incidence of 41 per 100 000 population per year. 3 Thrombosis more often involves the superficial venous system and can be associated with venous infarction in 40% to 50% of cases. 3 Dehydration, local head and neck or systemic infections, congenital heart disease, and anemia are the risk factors for childhood. Additional risk factors for neonatal CVST include asphyxia, chorioamnionitis, congenital heart disease, polycythemia, sepsis, and dehydration. 3 The importance of genetic and acquired prothrombotic disorders has been emphasized in recent series of pediatric CVST. 4,5 In a study which was performed by Sébire et al, and which were to examine clinical presentations of CVST, the prothrombotic risk factors and other predisposing events, anemia, high cholesterol, high triglycerides, high lipoprotein (a), high fibrinogen, low protein S, low protein C, low antithrombin, high factor VIII, low factor XII, factor V Leiden mutation, prothrombin 20210 mutation, thermolabile methylenetetrahydrofolate reductase homozygosity, high anticardiolipin IgG, hemoglobin Sickle Cell disease, chronically iron-deficient anemia were defined as risk factors. 6 In our reports, we did not find these risk factors in any patients.
Classical findings of CD usually start at 1 to 3 years of life. Toddlers and young children classically present with chronic diarrhea, vomiting, poor appetite, abdominal distension, abdominal pain, irritability, and failure to thrive sometimes after the introduction of gluten in the diet. 2 In adults, a variety of neuropsychiatric conditions, such as depression and anxiety, have been reported in individuals with CD. 2 In our study, case 1 had no any gastrointestinal symptoms and case 2 had only abdominal distention. The diagnosis of CD is confirmed by positive results of serological tests and evidence of characteristic histopathological findings on intestinal biopsy like in case 1, or CD 7 can also be confirmed with resolved problems after gluten-free diet like in case 2. Development of autoimmune diseases is one of the complications of CD. Tissue transglutaminase enzyme is an auto-antigen that is related with gluten-associated immune events. 8 In a study by Ozge et al, a patient with recurrent stroke and CD showed evidence of a central nervous system vasculitis. 9 Rush et al reported biopsy-proven central nervous system vasculitis in association with CD. 10 Kieslich et al designed a study to investigate brain white-matter lesions in CD. 11 Pratesi et al found that sera from patients with active CD contain IgA antibodies that react with human brain vessel structures, giving intense fluorescence. These antibodies were not present in sera from celiac patients on a gluten-free diet or nonceliac controls. They emphasized that this finding might be involved in the abnormal nervous system manifestations frequently described in association with CD. 12 In the light of these knowledge; tissue transglutaminase is the major autoantigen in CD and is thought to maintain vascular endothelial integrity. Anti-endomysial IgA antibodies demonstrate to be the same autoantibody as antitransglutaminase, react with cerebral vasculature, suggesting an autoimmune mechanism for CD-associated vasculopathy. Because CD is a potentially treatable cause of cerebral vasculopathy, serology—specifically antitissue transglutaminase antibodies—should be included in the evaluation of cryptogenic stroke or CVST in childhood, even in the absence of typical gut symptoms. 13 In literature, there are limited studies about CD with CSVT association. In these studies, some risk factors other than CD were found. However, in our patients, we only found CD as a risk factor for CVST.
In our cases, case 1 had only symptoms related to CVST, case 2 had only abdominal distention and symptoms related with CVST. Both of them had normal weight and height and seemed healthy until CVST occurring. We did not exactly say that CVST occurred due to CD. However, we think that CD might be a predisposing factor for CVST. Because in literature there are some reports about CD and portal vein thrombosis or CD and cerebral infarct or CD and epilepsy association. Therefore, we think that cases with CVST can be investigated for CD and in these cases, gluten-free diet could help the treatment.
In conclusion, we suggest that CD can be routinely screened in children with CVST even in the absence of any typical gut symptoms and algorithm of CVST can be involved in the investigation of CD. Controlled, large-scale researches should be performed to understand the risk factor of CD.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.