
Abstract
Keywords
Introduction
Acute ischemic stroke (AIS) remains a global health burden as it represents the second leading cause of a significant morbidity. 1 Several nonmodifiable risk factors such as age and gender and modifiable risk factors such as hypertension and heart failure are known to represent major contributors to the incidence of stroke. 2 While it is difficult to control the effect of nonmodifiable risk factors, major public health efforts have focused on managing modifiable risk factors, such as congestive heart failure (HF) to decrease the stroke burden. 3
Heart failure is a complicated clinical condition caused by structural or functional cardiac distress, resulting in decreased cardiac output or increased intracardiac pressures. 4 More than 15% of AIS patients present with HF, and AIS is reported to be caused by HF in at least 9% of stroke cases.4,5 Moreover, HF constitutes the source of various damaging pathophysiologic mechanisms in AIS, including the release of prothrombotic and proinflammatory mediators and poor cerebral tissue oxygenation. 6 Therefore, HF may affect the safety and efficacy of acute recanalization stroke therapies, including the use of recombinant tissue plasminogen activator (rtPA). 7
The standard treatment for ischemic stroke is rtPA. Since its approval by the FDA in 1996, rtPA has resulted in significantly better clinical outcomes in patients with symptomatic stroke, 7 such that more than 30% of patients who meet inclusion criteria experience only minimal or no disability following treatment with rtPA. 8 When treated with rtPA, the clinical response in AIS-HF patients is the same as in AIS patients without HF. 2 This finding indicates the efficacy and safety of rtPA for AIS-HF patients. 9 Moreover, there is no evidence of an increased risk of symptomatic intracerebral hemorrhage (sICH) after intravenous rtPA in AIS-HF patients. 10 However, despite the safety of rtPA, many AIS-HF patients are less likely to be treated with rtPA and more likely to present with higher rates of mortality and long-term deficits compared to a similar cohort without HF.11,12
Safety of rtPA implies that ischemic stroke patients treated with rtPA are not associated with complications related to intravenous r-tPA including symptomatic intracranial hemorrhage, and major systemic hemorrhage.11,12 One possibility that many AIS-HF patients are less likely to be treated with rtPA could be that AIS-HF patients may present with risk factors that worsen outcomes following rtPA therapy and are therefore unable to benefit from the demonstrated advantage of rtPA reperfusion therapy. This study aims to identify risk factors associated with exclusion from rtPA therapy in AIS patients with HF. Our results may help identify specific stroke risk factors that could explain why some cohorts of AIS-HF patients are less likely to receive rtPA. Knowledge of these factors will provide further insight into specific risk factors that can be managed to improve the care of AIS patients with heart failure.
Methods
Study Population
This is a retrospective cohort study using data obtained from a regional stroke registry of Prisma Health Upstate. The registry includes all patients aged >18 admitted to Prisma Health stroke unit between January 2010 and January 2016. The description of the registry is provided in previous studies.13,14 Our study was approved by the Prisma Health ethics committee. We extracted data from all AIS patients with and without HF who underwent a series of blood tests and brain imaging to confirm ischemic stroke at admission. All data were obtained from electronic records. Patients with a prior diagnosis of primary intracerebral, intraventricular, or subarachnoid hemorrhage or those unable to complete coronal vascular imaging were not included in our data analysis. The inclusion criteria included patients’ data for strokes diagnosed and confirmed by computed tomography (CT) or magnetic resonance imaging (MRI) within 7 days of the appearance of symptoms or clinical signs. We focused on data for AIS patients with and without a history of HF for this study and collected patients’ demographics, laboratory values, medical history, and medications. The demographic variables included age, race, gender, ethnicity, and Body mass index (BMI). In addition, data for NIH stroke severity (NIHSS) were collected. Data on risk factors were collected, including atrial fibrillation/atrial flutter, coronary artery disease (CAD), carotid stenosis, depression, diabetes, drug or alcohol use, dyslipidemia, family history of stroke, congestive heart failure (CHF), hormonal replacement therapy, hypertension, migraine, obesity, prior stroke, prior transient ischemic attack (TIA), prosthetic heart valve, peripheral vascular disease, chronic renal disease, sleep apnea, and history of smoking. Data on ambulatory status were recorded at different times during the entire clinical encounter: on admission, during admission, and after discharge. Scoring ambulatory data was performed in this fashion: 0 (not documented); 1 (patient not able to ambulate); 2: (ambulate with assistance) 3: (ambulate independently). Improvement in ambulation was quantified by taking their score at discharge and subtracting their ambulation score on admission, with greater than zero being an improvement in ambulation.
Statistical Analysis
All statistical analyses were determined using the Statistical Package for Social Sciences version 26.0 for Windows (SPSS, Chicago, IL), and P < .05 was considered statistically significant. Univariate analysis was used to determine differences in risk factors in AIS with or without a previous diagnosis of HF, and AIS patients with or without HF stratified by receipt or no receipt of rtPA. Univariate analysis was used to evaluate differences in continuous and categorical variables. For all continuous variables, the mean, standard deviation, and range were calculated using the Student's T-tests, while discrete variables were analyzed using Pearson's Chi-Squared analyses. The univariate analysis was used to identify demographics and risk factors for acute ischemic stroke patients stratified by receipt or no receipt of rtPA for Table 1, while Table 2, compares risk factors of acute ischemic stroke patients with or without heart failure stratified by receipt or no receipt of rtPA
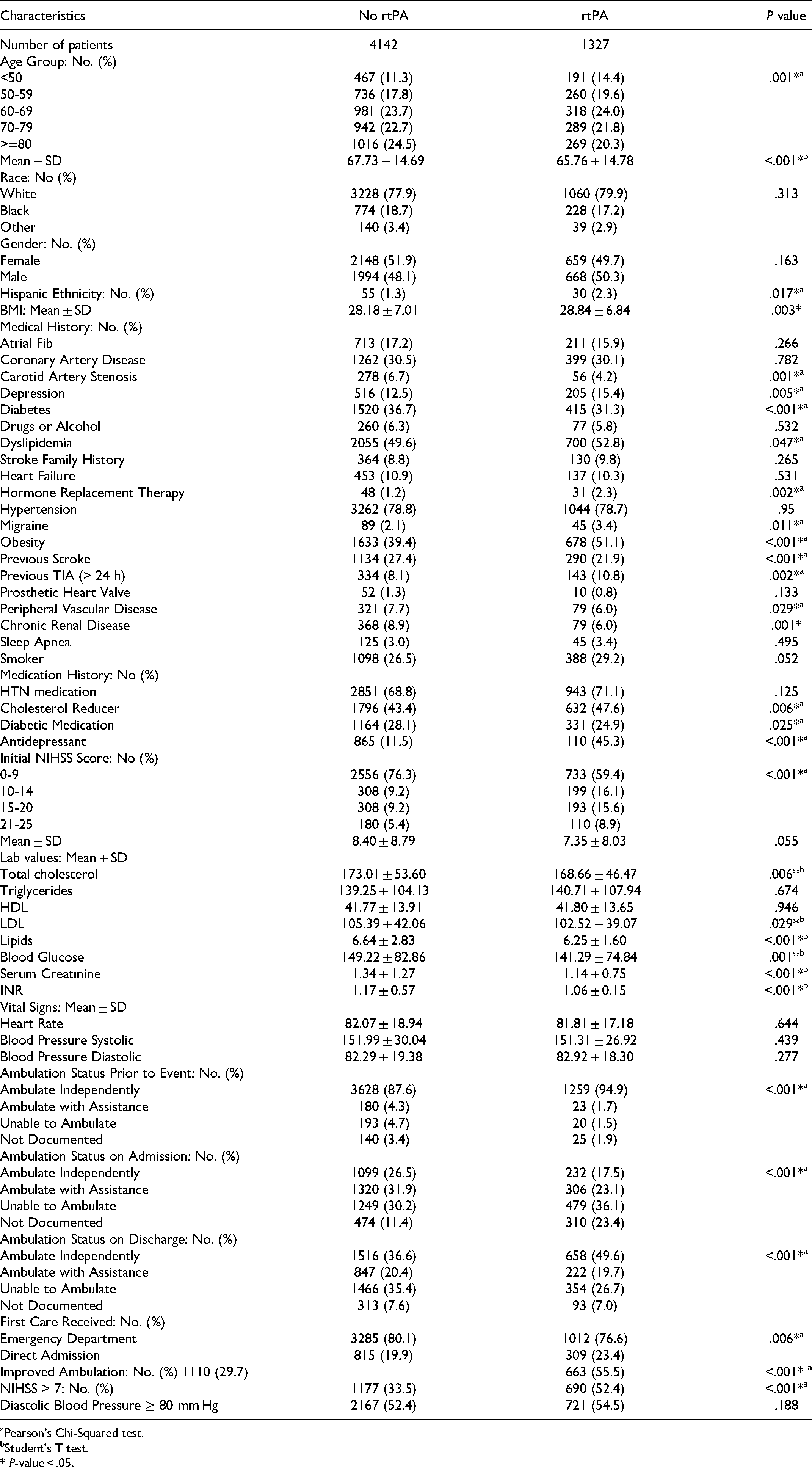
Demographic and Factors for Acute Ischemic Stroke Patients Stratified by Absence or Presence of rtPA use Among Acute Ischemic Stroke Patients.
Pearson's Chi-Squared test.
Student's T test.
* P-value < .05.
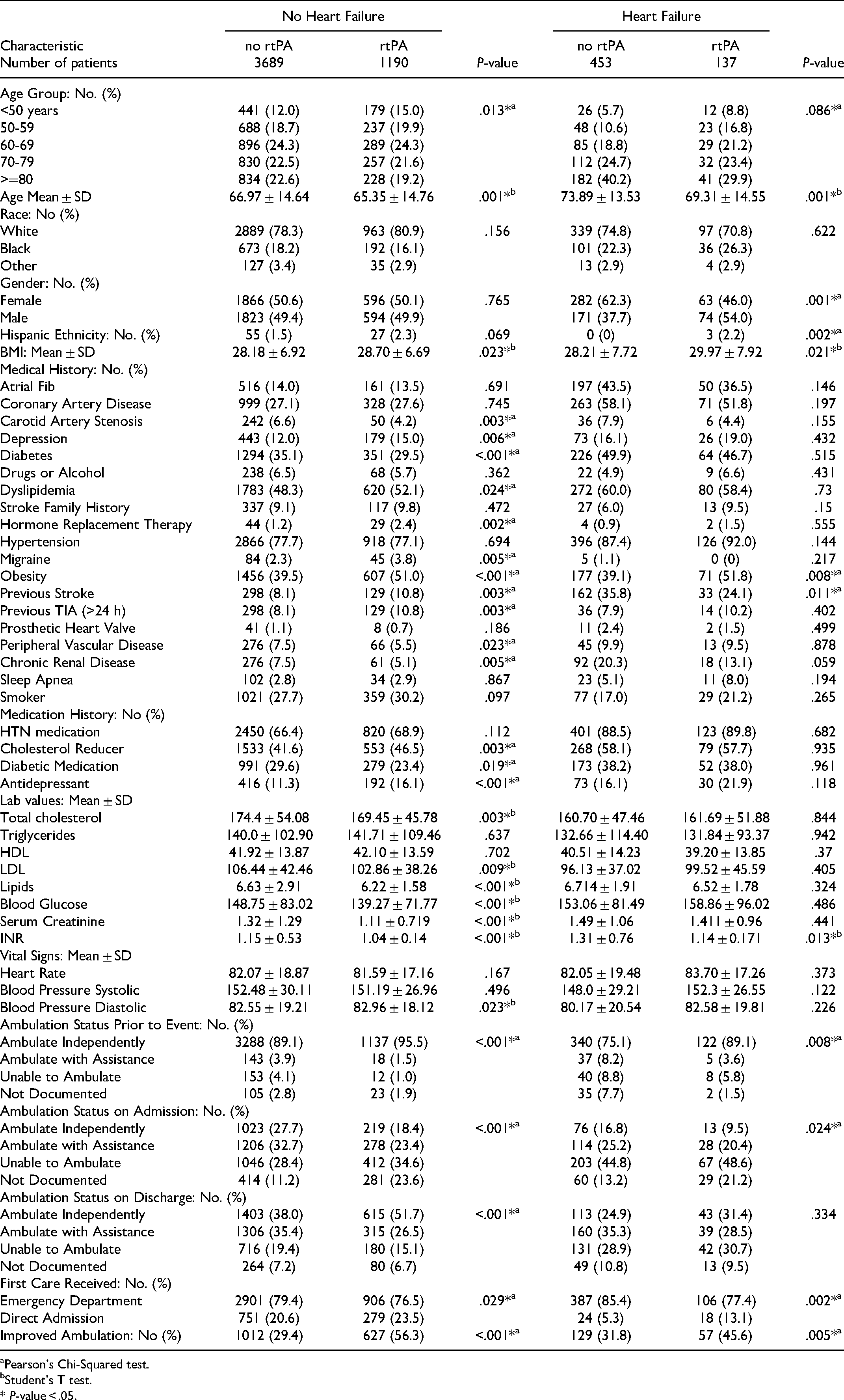
Comparison of Demographics and Risk Factors of Acute Ischemic Stroke Patients with or Without Heart Failure Dependent on rtPA Administration.
Pearson's Chi-Squared test.
Student's T test.
* P-value < .05.
For the multivariate analysis, significant associations in the univariate comparisons were entered into a binary multivariable logistic regression model. The adjusted odds ratios (ORs) for risk factors were calculated from their respective coefficients in the logistic regression models. We used a backward stepwise logistic regression analysis approach and considered a statistical variable removal level of P < .10. Potential risk factors associated with inclusion or exclusion from rtPA were calculated. We performed subgroup analyses for AIS patients with HF while AIS patients without HF served as the control. We determined our models’ sensitivity, specificity, and accuracy by using the area under the Receiver Operating Curve (ROC). The Hosmer Lemeshow test determined multicollinearity and interactions among the independent variables.
Results
A total of 5469 AIS were identified. Of these, 4142 patients did not receive rtPA, while 1327 patients received rtPA. Table 1 presents the risk factors of AIS patients stratified by treatment with or without rtPA while Table 2 presents risk factors, demographics, and laboratory characteristics of AIS patients with or without HF stratified by rtPA treatment. Compared with the AIS-HF group without rtPA, AIS-HF patients that received rtPA were more likely to be Hispanics, younger, and have a higher BMI, obese with a history of elevated INR, ambulate independently prior to the stroke event and demonstrate improvement in ambulation status after discharge. They were less likely to be females, treated in the emergency department, and less likely to present with a history of previous stroke and an elevated INR.
AIS patients without HF that received rtPA were younger, with higher BMI, more likely to present with a history of depression, dyslipidemia, migraine, obesity, history of previous stroke, TIA, taking hormone replacement therapy, cholesterol reducers, antidepressants and more likely to present with higher diastolic blood pressure. They were less likely to present with peripheral vascular disease, chronic renal disease, higher total cholesterol, LDL, and lipids. AIS patients without HF that received rtPA were less likely to present with higher blood glucose, serum creatine, elevated INR, take diabetic medication, treated in the emergency department, ambulate independently prior to the stroke event, during admission or after discharge.
The results for the adjusted analysis for risk factors associated with rtPA in the AIS population of patients without HF are presented in Table 3. AIS patients without HF that did not receive rtPA therapy were more likely to be Hispanic, have coronary artery stenosis, a previous history of stroke, and present with elevated heart rate, INR, lipid levels, and serum creatinine. AIS patients without HF treated with rtPA were more likely to present with a history of a previous TIA, high total cholesterol, and direct admission for treatment. The discriminating power of the model was strong, as shown by the ROC curve (Figure 1), with the area under the curve (AUROC) = 0.698 (95% CI, 0.678-0.718 P < .001).
ROC curve for acute ischemic stroke patients without heart failure treated with rtPA. Area under the curve (AUC) values for the ROC analysis indicates a better discriminative capability of the model (AUC = 0.698, 95% CI, P < .001).
Clinical Factors that were Associated with rtPA Treatment for Acute Ischemic Stroke Patients Without Heart Failure. Adjusted OR<1 Indicates Factors Associated with Exclusion from rtPA While OR>1 Indicates Factors Associated with Getting rtPA Treatment. Hosmer-Lemeshow Test (P = .742), Cox & Snell (R2 = 0.105). The Overall Classified Percentage of 68.8% was Applied to Check for Fitness of the Logistic Regression Model. *Indicates Statistical Significance (P < .05) with a 95% Confidence Interval.

Backward Stepwise model based on Likelihood Ratio was applied.
Model assumptions were fulfilled.
Multicollinearity and interactions among independent variables were checked and no significant interactions were found.
Hosmer-Lemeshow test (P = .742), Cox & Snell (R2 = 0.105).
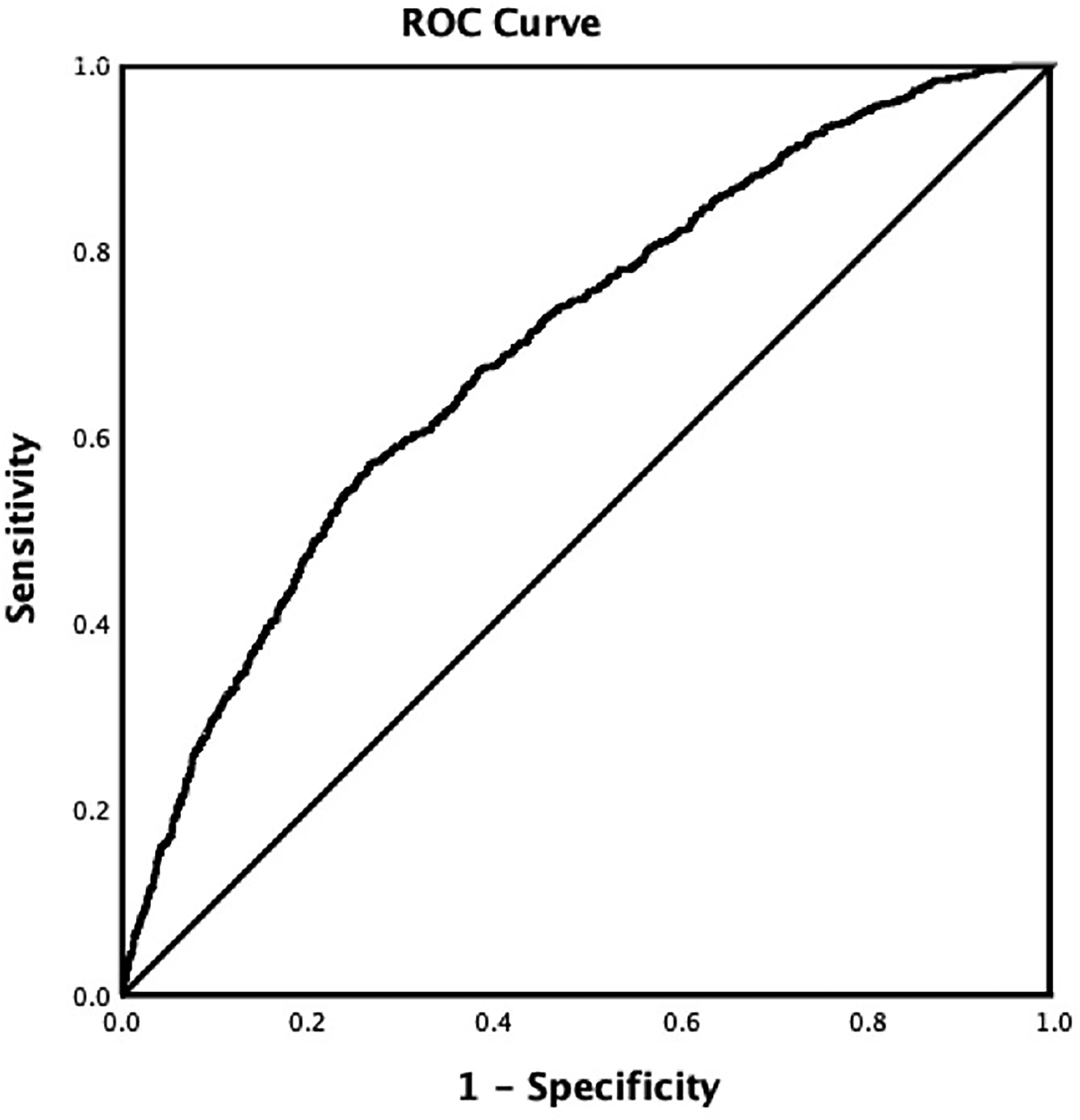
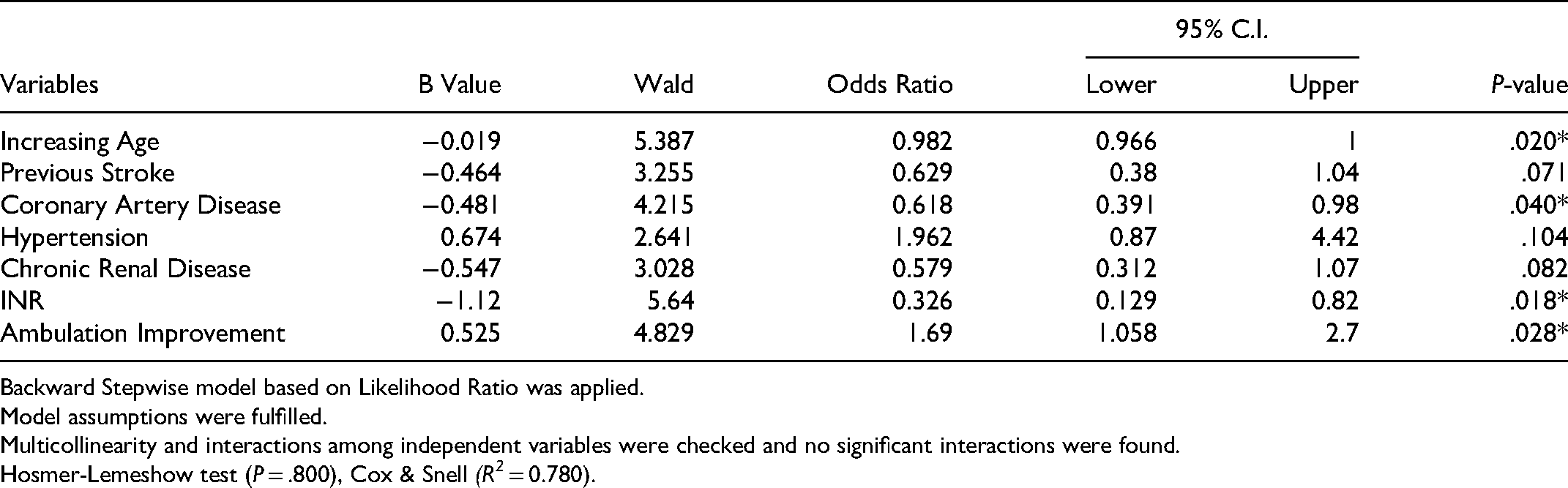
The risk factors associated with rtPA therapy in AIS patients with HF are presented in Table 4. Patients with increasing age that presented with coronary artery disease and a high INR level were more likely to not to receive rtPA. In contrast, AIS-HF patients with improved ambulation were more likely to be treated with rtPA. The discriminating power of the model was strong, as shown by the ROC curve (Figure 2), with the AUROC = 0.668 (95% CI, 0.611-0.724, P < .001).

ROC for acute ischemic stroke patients treated with heart failure. Area under the curve (AUC) values in ROC analysis indicates a better discriminative capability of the model with the area under the ROC curve (AUC) = 0.668, 95% CI, P < .001.
Clinical Factors Associated with rtPA Treatment for Ischemic Stroke Patients with Heart Failure. Adjusted OR<1 Indicates Factors that are Associated with Exclusion from rtPA While OR>1 Indicates Factors that are Associated with Treatment with rtPA. Hosmer-Lemeshow Test (P = .800), Cox & Snell (R2 = 0.780). The Overall Classified Percentage of 75.4% was Applied to Check for Fitness of the Logistic Regression Model. *Indicates Statistical Significance (P < .05) with a 95% Confidence Interval.
Backward Stepwise model based on Likelihood Ratio was applied.
Model assumptions were fulfilled.
Multicollinearity and interactions among independent variables were checked and no significant interactions were found.
Hosmer-Lemeshow test (P = .800), Cox & Snell (R2 = 0.780).
Discussion
Patients with HF are reportedly to recurrently not treated with rtPA in stroke clinical trials, either due to their poor premorbid functional status. 15 Notwithstanding, most of the evidence regarding treatment outcomes in AIS-HF patients are mainly from observational studies.16,17 Findings reveal that HF is an independent predictor of unfavorable outcomes.18,19 While a lower fraction of higher mortality risks linked to HF in AIS have been reported, 6 it has also been observed that there was no difference in the rate of successful vessel recanalization after intravenous rtPA between patients who had a stroke with and without HF.6,9 Furthermore, there was also no difference in the rate of intracranial bleeding.
While existing studies10,20 suggest that AIS-HF patients present with specific risk factors that worsen outcomes, the current study investigated the specific risk factors that may contribute to the reason that AIS-HF patients are less likely to receive rtPA and are therefore unable to benefit from the demonstrated advantage of thrombolytic therapy. In the adjusted analysis for AIS patients without HF, we observed that patients that received rtPA presented with a history of previous TIA, elevated cholesterol levels, and direct admission to a primary stroke center for treatment. Similar findings have been reported for AIS patients with histories of previous TIA,21–23 elevated cholesterol levels,13,24 and direct admission.25,26 We also observed that AIS patients without HF who did not receive rtPA were more likely to be Hispanic and present with coronary artery stenosis, previous stroke, and elevated lipid level, creatinine, INR, and heart rate. Our finding that Hispanic AIS patients without HF were more likely not to be treated with rtPA is supported by prior studies showing lower rates of rtPA use among the Hispanic population. 27
In addition, our finding that AIS patients without HF that present with coronary artery stenosis, history of previous stroke, and elevated lipid levels, INR, creatinine, and heart rate was more likely not to receive rtPA is consistent with other studies demonstrating the association between rtPA and elevated heart rate, 28 lipid levels, 29 INR, 30 creatinine, 31 coronary artery stenosis, 32 and previous stroke. 29 Estimates of eligibility for rtPA in the AIS population are reported to range from 6% to 8% of all strokes.33,34 While the most common exclusion factor for rtPA is the delay in presentation for treatment, comorbidities such as history of coronary artery stenosis,35,36 previous stroke,29,37 elevated lipids, 38 INR, 39 creatinine, 31 and heart rate 21 have been reported to contribute to the low eligibility rate for rtPA.
In the AIS cohort with HF, we observed that older and present with coronary artery disease and elevated INR levels were more likely not to be treated with rtPA. Age is one of the critical factors influencing the treatment outcome of stroke. 40 The gap in clinical outcomes between those <80 and >80 years of age is significant when comparing long-term outcomes.21,41 Therefore, it is not surprising that some of the major, randomized, controlled trials testing the efficacy of thrombolytic agents excluded older patients. 42 While age is not an exclusion criterion for rtPA, 29 studies43,44 have found that patients over 80 did not receive rtPA due to a higher risk of intracranial hemorrhage or hemorrhagic conversion. Therefore, the fear of bleeding in addition to the increased burden of comorbidities in the HF population, and the association with poor neurologic outcomes and higher mortality rates45–47 may contribute to our finding that older AIS-HF patients were more likely not to be treated rtPA therapy.
Moreover, we found that AIS-HF patients with a history of CAD were more likely not to be treated with rtPA. CAD is a major contributor to HF and is associated with high morbidity and mortality.45,48 Approximately 65% of patients admitted for HF present with a history of CAD. 49 Stroke severity among AIS patients with CAD is reported to be comparable to that of AIS patients with HF. 49 This finding indicates that CAD and HF are associated with worse outcomes in AIS patients.50,51 Our finding that AIS-HF patients with CAD did not receive rtPA therapy suggests the need for a future study to distinguish CAD status by clinical history from the underlying etiology of HF in AIS patients. Such a study will provide the basis for other studies to test novel therapeutic strategies targeting CAD in the AIS-HF patient population.
We also found that AIS patients with HF that presented with an elevated International Ratio (INR) were less likely to receive rtPA. INR is used to evaluate coagulopathies associated with rtPA therapy. 52 In the current guideline, 53 an INR > 1.7 is considered as an exclusion criterion for rtPA. However, whether it is safe to administer rtPA at INR levels lower than 1.7 is controversial, especially as rising INR indicates a risk of bleeding. 54 The INR level in our AIS-HF patient cohort was 1.14, indicating that the presence of HF and an elevated INR may pose a risk of bleeding and thus lead to exclusion from rtPA.
Our finding that an improvement in ambulatory status during admission was associated with rtPA therapy in AIS-HF patients was not surprising. Improvement in ambulatory status is a quantitative metric based on a patient's stroke recovery during hospitalization. This variable has been previously documented as a predictor of long-term stroke recovery after rtPA administration. 55 This finding supports our current result that AIS-HF patients treated with rtPA were more likely to be associated with an improvement in ambulatory status.
Limitations
This was a retrospective analysis of data from a regional stroke registry. Since this is not a prospective, randomized, controlled study, it is difficult to determine cause-and-effect relationships for rtPA in AIS-HF patients. Also, the patients’ records did not define HF status, which could misclassify those with subclinical HF. Moreover, previous coronary revascularization has been shown to reduce the association between CAD and poor HF outcomes. Our results in a population with a significant revascularization history may underestimate the impact of CAD. Finally, several other factors such as heavy episodic alcohol consumption, hyperlipidemia, hypercholesterolemia, metabolomic syndrome, cardiomyopathy hypoglycemic medications not present in our stroke data base may affect the use of rtPA for AIS-HF patients. Future studies on the effect of such risk factors on the use rtPA therapy for will help to improve the care of AIS patients with or without HF.
Conclusion
Heart failure is highly prevalent in patients hospitalized for AIS. In this study, AIS patients with heart failure who presented increased age, coronary artery disease, and an elevated INR were more likely not to be treated with rtPA therapy. Our findings identify specific risk factors that can be managed to improve the use of rtPA therapy for AIS-HF patients.
Footnotes
Acknowledgment
We thank the stroke unit of PRISMA Health-Upstate for helping in the data collection.
Authors’ Contribution
CBS, KK, NP, CR, CE and TIN designed the concept, experiment, and data analysis. MS, MGE and TIN critically revised the drafts, interpreted the results, read and approved the last version of this manuscript. All authors have provided the corresponding author with permission to be named in the manuscript and approved the submission of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This is a retrospective data collection. The institutional review board approved this study of PRISMA Health institutional committee for ethics (approval number: 00052571).
Availability of Data and Materials
The retrospective datasets are available by request from the corresponding author of this manuscript, respectively.