
Abstract
Background:
Diagnosing cerebral venous sinus thrombosis (CVST) in patients referring to emergency service or neurology outpatient unit with complaints of headache is a challenging task. Magnetic resonance (MR) venography is the gold standard, but there are limitations regarding its use.
Aim:
To evaluate the validity of red cell distribution width (RDW) in CVST diagnosis in patients presenting with headache.
Methods:
A total of 138 patients comprising 37 patients with CVST and 101 control primer headache cases were included in this retrospective cross-sectional study. Control group consists of hospitalized patients with primary headache. Venous blood hemoglobin (Hb), platelet, mean corpuscular volume (MCV), RDW, fibrinogen, and vitamin B12 levels of the patients were recorded at the first referral. Diagnosis of CVST was established by MR venography.
Results:
The RDW ratio of patients with a diagnosis of CVST was significantly higher than that in patients with primary headache (15.3 ± 1.4 vs 13.3 ± 0.5; P <.0001). Fibrinogen and vitamin B12 levels were not significantly different between the 2 groups. In a total of 11 patients, there was more than 1 thrombosis. In 21 of the patients with CVST, gene mutation was detected. There was no significant difference between the patients with and without mutations regarding RDW values. Diagnostic validity of RDW was found to be excellent in differentiating patients with CVST and primary headache (area under the curve = 0.996; 95% CI: 0.990-1.000). Optimum RDW cutoff value was determined as 14.1% (sensitivity: 91.9%, specificity: 99%, positive predictive value: 92.8, negative predictive value: 0.082).
Conclusion:
We suppose that among patients presenting with the complaint of headache, RDW value may lead to diagnose CVST.
Introduction
Headache accounts for 4% of emergency department (ED) referrals and two-third of neurology outpatient referrals. 1,2 Among patients with headache, cerebral venous sinus thrombosis (CVST) is a fatal and uncommon disease, and its diagnosis is potentially challenging. 3 Incidence of CVST was reported as 7 of 100,000 hospitalized patients, 4,5 and it accounts for 0.5% to 1.0% of all patients with stroke. It is most commonly encountered in young adult females (75%). The most common presenting symptom is headache (88.8%), and it can be the only presenting sign or symptom in patients with CVST. 6 The CVST diagnosis in patients with headache can be established in tertiary health facilities. The most employed noninvasive diagnostic method is magnetic resonance venography in suspected cases of CVST. 7 Access to this method is relatively difficult and it is relatively expensive. Also its use in emergency conditions is limited and it is relatively time consuming.
Red corpuscle distribution width (RDW) indicates whether the red cells are different in size or not (anisocytosis). The RDW being higher than normal is a marker of difference in size between red cells. 8 Measurement of RDW level is a relatively easy-to-do and less costly parameter of blood count test among routine blood tests. Although each instrument has its own upper limit values, over 14% is considered as pathologic. In a recent study by Kim et al in patients with acute cerebral infarct, higher RDW values were reported to be correlated with poor clinical outcome and mortality. 9 In another study, higher RDW value was reported as related to stroke. 10 Recently, in acute myocardial infarction, cardiac insufficiency, stable angina, peripheral arterial diseases, and arterial ischemic stroke, the patients’ RDW values were found to be higher. 11
To the best of our knowledge, RDW level was never measured in patients with CVST, which is a rare subtype of stroke. The objective of our study is to investigate the efficacy of RDW values in detecting CVST.
Materials and Methods
Patients, Setting, and Inclusion–Exclusion Criteria
In this retrospective cross-sectional study, 148 patients hospitalized in neurology clinic between the years 2010 and 2012 were investigated. Of the 47 patients with CVST, 7 were excluded since they had no headache and 3 because of anemia, which may interfere with the RDW values. Control group consisted of consecutive hospitalized patients with primary headache having the following diagnosis: 55 tension-type headache, 25 migraine, and 21 other types of headache (cluster, coital, SUNCT, etc). Finally, a total of 138 patients were included—37 patients with CVST and 101 control cases. In both groups, there was no known comorbidity.
Laboratory Methods
Venous blood samples were obtained from patients for complete blood count (CBC) at the time of referral to the ED. As inpatients in neurology clinics, fibrinogen,
Red cell distribution width (RDW) is a parameter of the standard full blood count tests, measuring the size variability of erythrocytes. 8 Elevated RDW levels can be observed in many clinical conditions, such as anemia, nutritional deficiencies, hemodilution, and abnormalities of the erythropoietin response. The RDW levels may also increase the iron-deficiency anemia, vitamin B12 and folate deficiency, hemolysis, and blood transfusion. 12 We have excluded patients who had any illness that may affect RDW levels (such as thalassemia trait, hereditary helliptocytosis, hemoglobin C disease, hypertension, diabetes, etc) from the study and observed that vitamin B12 levels were similar in each group.
Imaging
In each patient in the study, imaging was performed by 1.5-T (Siemens Medical Systems, Siemens Inc., Erlangen, Germany) magnetic resonance imaging (MRI) device with head coil. The MRI was performed with conventional pulse sequence spin echo in sagittal and axial plane, fast Spin echo T2-weighted and fast fluid-attenuated inversion recovery sequences in transverse plane. Following MRI test in patients with suspected CVST, diagnosis was established by MRI venography.
Ethics and Statistics
The study was approved by the institutional ethics committee. Data were recorded as percentage, mean, and standard deviation. Comparisons between patients with CVST and primary headache were made by using chi-square tests for categorical variables and independent samples t test or Mann-Whitney U tests for normally or abnormally distributed continuous variables, respectively. Receiver–operating characteristic (ROC) curve analyses were performed to identify the optimal cutoff point of RDW for the prediction of CVST among patients with headache. Analysis of the data was performed using SPSS 20.0 (SPSS, Inc, Chicago, Illinois).
Results
Totally, 138 patients with headache were included into the study. Of them, 37 (26.8%) were patients with CVST and 101 (71.6%) patients were evaluated as controls (Table 1). There was no significant difference between the 2 groups regarding demographic characteristics. Demographic information and laboratory findings of both groups are shown in Table 1.
Demographic and Laboratory Features of CVST and Control Groups.
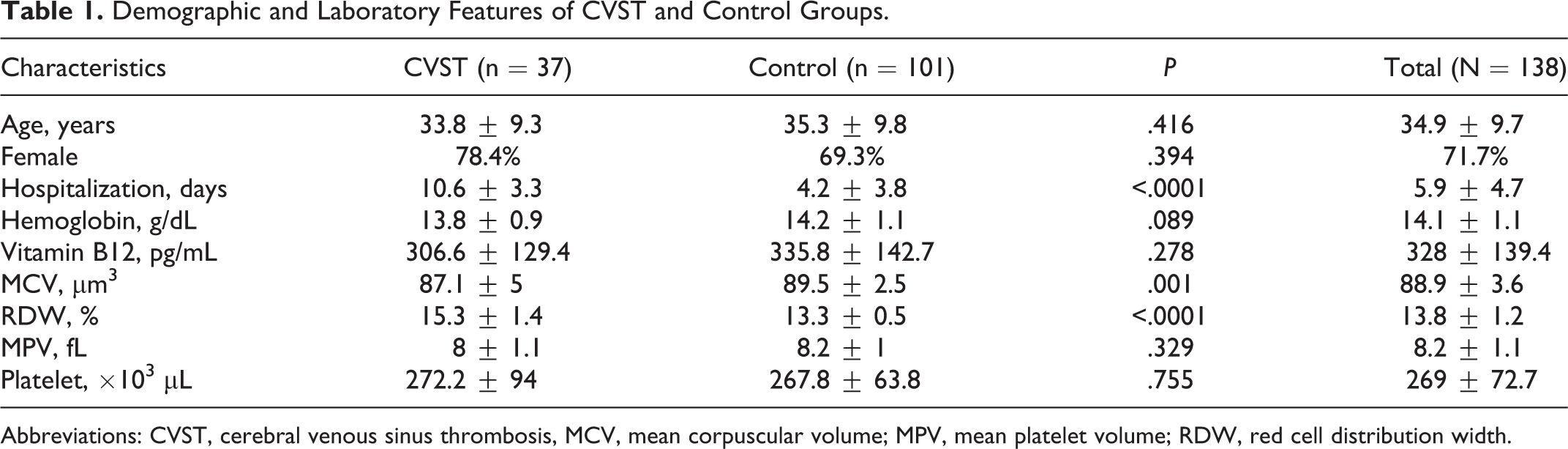
Abbreviations: CVST, cerebral venous sinus thrombosis, MCV, mean corpuscular volume; MPV, mean platelet volume; RDW, red cell distribution width.
We performed a subgroup analysis and found no difference between RDW levels among patients with headache according to the diagnosis of headache in the control group. The RDW values were significantly higher in patients with CVST compared to patients with primary headache, but MCV values were lower. Hospital stay was longer in patients with CVST. Fibrinogen level was investigated in both groups, but no significant difference was found (316 ± 97.4 in the CVST group [n = 14] vs 314 ± 129.2 in the control group [n = 55]; P = .954). Only in 4 patients with CVST, the
Signs and Symptoms of Patients With CVST.
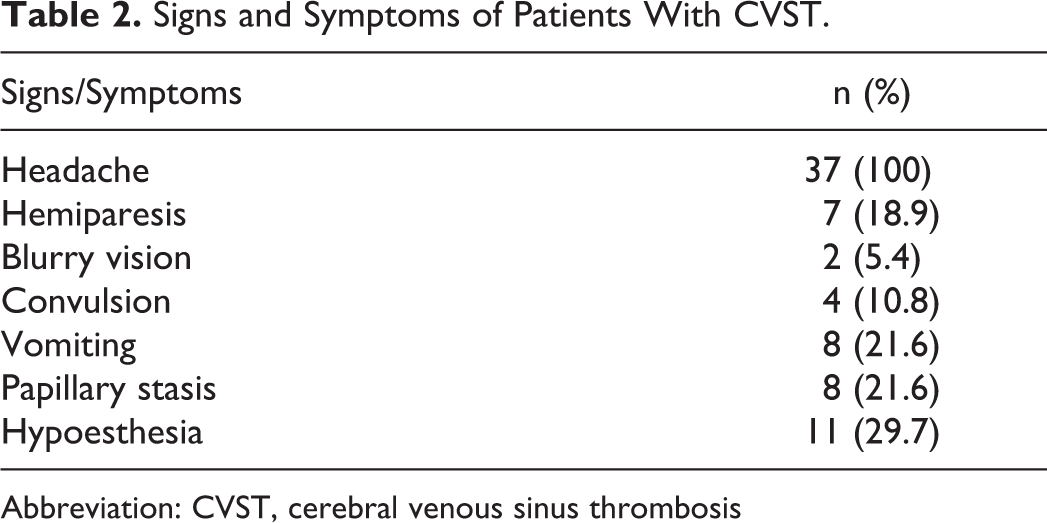
Abbreviation: CVST, cerebral venous sinus thrombosis
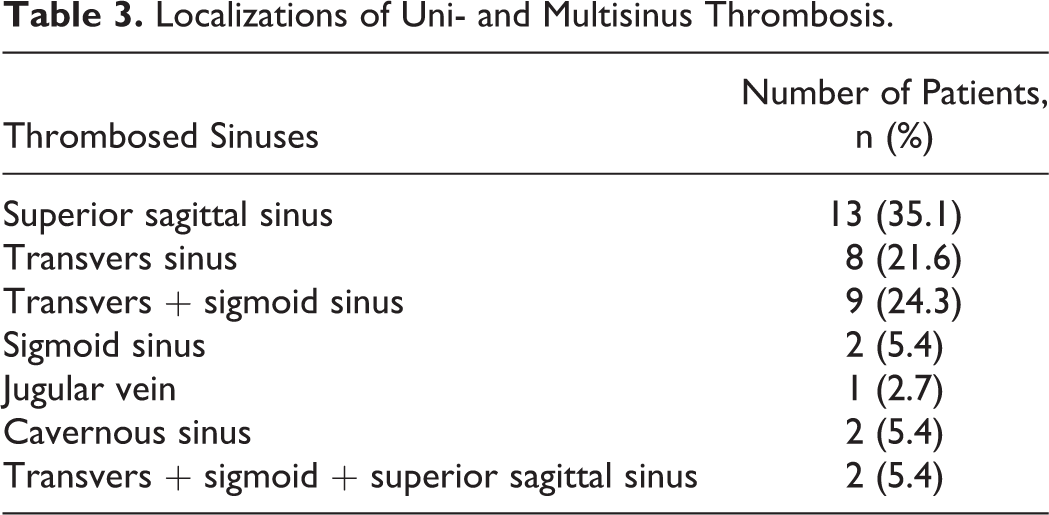
Localizations of Uni- and Multisinus Thrombosis.
Etiology of CVST.
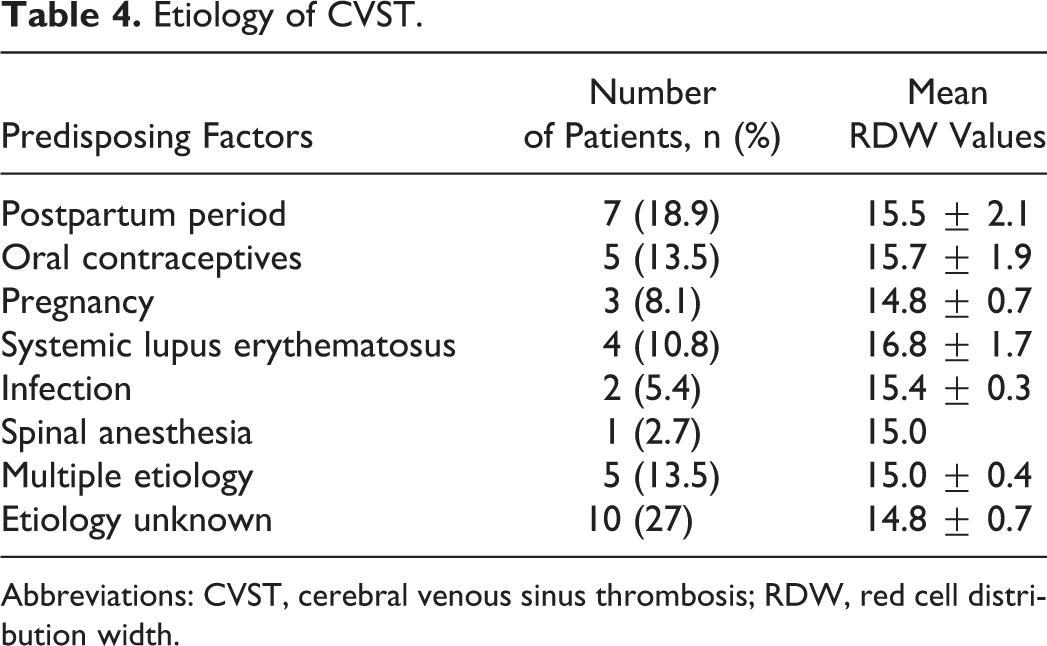
Abbreviations: CVST, cerebral venous sinus thrombosis; RDW, red cell distribution width.
After we evaluated the discriminative value of RDW and MCV in differentiating patients with CVST and primary headache, we found the diagnostic accuracy was better in RDW (Table 5). In differentiating CVST from primary headaches, it was found that the optimum RDW cutoff value was 14.1% (Table 6).
The Areas Under the ROC Curves for CVST for Diagnostic Parameters in Patients With Headache.
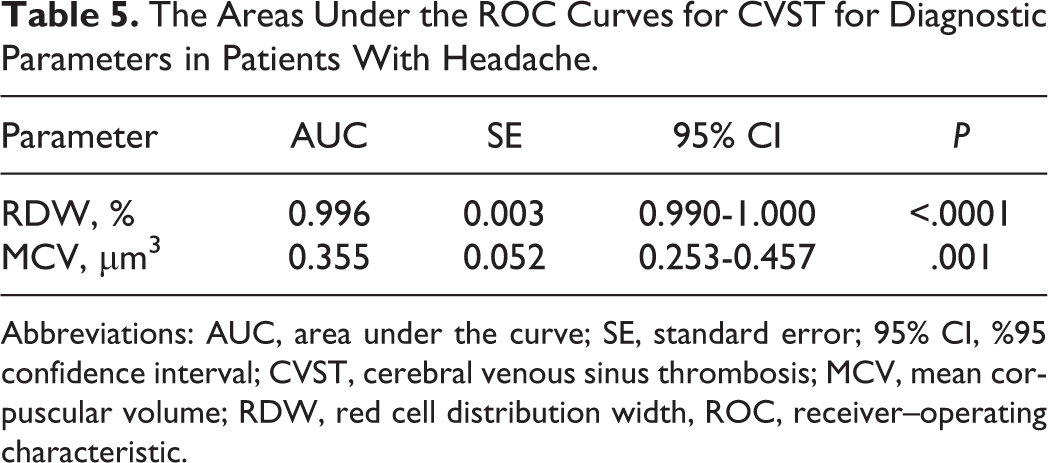
Abbreviations: AUC, area under the curve; SE, standard error; 95% CI, %95 confidence interval; CVST, cerebral venous sinus thrombosis; MCV, mean corpuscular volume; RDW, red cell distribution width, ROC, receiver–operating characteristic.
Diagnostic Value of the Cutoff Value of RDW for CVST in Patients With Headache.
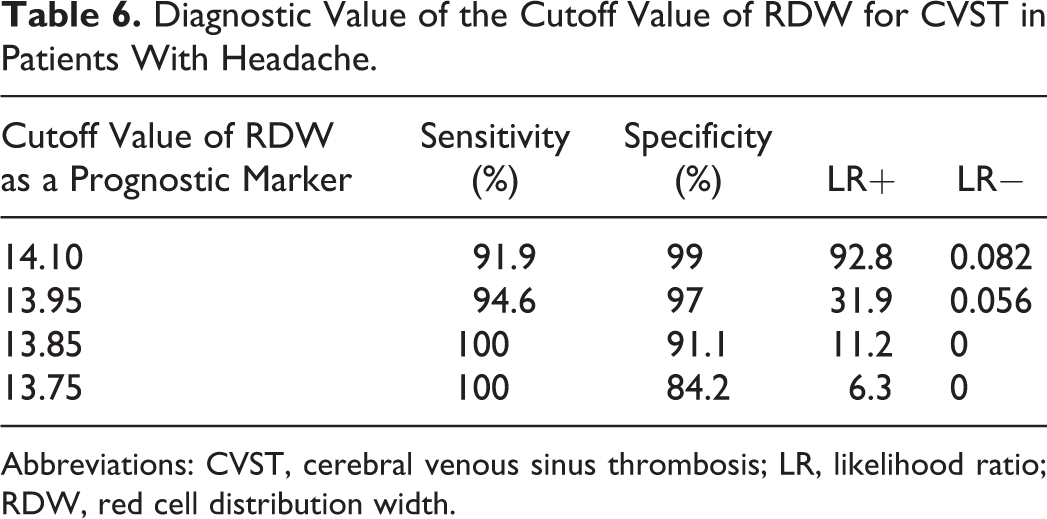
Abbreviations: CVST, cerebral venous sinus thrombosis; LR, likelihood ratio; RDW, red cell distribution width.
Cutoff levels differed according to gender. For males, the best cutoff values, sensitivity, specificity, likelihood ratio (LR)+ and LR− were 14.05, 87.5%, 98.6%, 27.1, and 0.13, respectively. For females, these parameters were 13.95, 96.6%, 97.1%, 33.8, and 0.04, respectively.
In patients with CVST, there was no relation between hospital stay and RDW levels (P = .826). There was no death among patients with CVST.
Discussion
Per our study, RDW is a highly valuable tool in the diagnosis of CVST in patients presenting with headache.
Cerebral venous sinus thrombosis is an important disorder that should be considered in differential diagnosis and may result in severe neurological sequel if overlooked. The mean age is 39 years, with approximately 75% female predominance, 13 and the main clinical spectrum includes headache, seizures, focal neurological signs, and alteration in consciousness. 14 Current data on the symptomatology of CVST give no information on the predictive value of specific modes of presentation or their combination. 15 Main predisposing conditions for CVST are oral contraceptives (54.3%), prothrombotic conditions (34.1%) such as factor V Leiden, antithrombin 3 deficiency, protein C or S deficiency, pregnancy/puerperium (21%), and infection (12.3%). Other risk factors include head injury, lumbar puncture, and young age. 16,17 The most frequent locations are the superior sagittal sinus (62%), transverse sinus (41%-45%), straight sinus (18%), and cortical veins (17%). 6
Since definitive diagnosis of CVST is possible only by MRI venography, the rates of missed diagnosis is high in emergency conditions. 18 In a study, median duration from symptom onset to diagnosis was 7 days, and delays were associated with worse outcomes, especially visual deficits. 19 Initial noncontrast head computed tomography (CT) is positive in only 70% of the patients, and sensitivity is found to be only 30%. 6,16 Imaging as performed by venous CT angiography or MR angiography has only 1 to 2 of 10 chances to detect CVST when typical symptoms are present. 15 The gold standard for the diagnosis of CVST is MRI venography. 18 However, MRI venography is a costly and time-consuming test. Thus, it may not be carried out in unstable patients. Inability to perform it in patients with prosthesis is another setback. Our study is of significance, since it points out that before using any imaging method the RDW values within the risk group patients may determine patients that are candidates for MRI venography.
The
Recently, RDW elevation has been proven to reliably reflect the extent of systematic inflammation, mainly in cardiovascular and pulmonary diseases. 24 It was demonstrated that elevated RDW was a strong independent predictor of outcome in patients with chronic heart failure, pulmonary embolism, acute myocardial infarction, and end-stage renal disease. 25 Increased RDW was also found to be associated with death due to stroke. 26 Wen identified a graded and independent association of baseline RDW with intimal medial thickness/inner diameter and incidence of carotid plaque. High RDW value is closely associated with the risk of carotid artery atherosclerosis in patients with hypertension. 27 As to our knowledge, our study is the first to show a possible role for RDW in differential diagnosis of CVST among patients with headache.
In our study, the reason RDW being almost an excellent diagnostic tool may be that CVST is a disease of young/middle-aged people. It has been proven that RDW value increases in advanced age diseases such as chronic heart failure, pulmonary embolism, and acute myocardial infarction. 12 However, in patients with CVST, these conditions that may lead to false-positive results are very rare. Control group also consisted of young patients without systemic diseases, such as hematological disorders, diabetes mellitus, hepatic, or renal diseases, that alter the RDW levels.
Various mechanisms may lead to a rise in RDW in CVST. One of the most important mechanisms is inflammation. Inflammation slows iron metabolism and simultaneously inhibits erythropoietin production and response. 28 Proinflammatory cytokines have been shown to impede red cell maturation, the latter of which can manifest as an elevated RDW level. In disorders such as idiopathic pulmonary hypertension and PTE significant correlation between RDW and inflammatory cytokines has been found. 29 In addition to inflammation, oxidative stress may have a role in elevation of RDW. 20 Oxidative stress may shorten the life of erythrocytes by oxidative damage and may contribute to anisocytosis. Neurohumoral and adrenergic system activation may also elevate RDW levels by stimulating erythropoiesis. 30 In patients with CVST, various endogen mediators such as growth hormone, vascular endothelial growth factor, nitric oxide, inflammatory markers, and neurohumoral markers may cause endothelial damage. Endothelial damage may also occur in coronary artery diseases and is closely correlated with RDW. 31
Investigations studying RDW and brain diseases are limited. In a study in 2008, Ani and Ovbiagele have found that high levels of RDW have contributed to stroke. In addition to that, higher RDW has been reported to be strongly predictive of total mortality in patients with cardiovascular disease and stroke. 10 Kim et al found that elevated RDW measured in patients with acute cerebral infarction was associated with poor functional outcome and mortality. They concluded that RDW may be used as a biomarker for the prediction of long-term outcomes in patients with acute cerebral infarction. 9
Primary limitations of our study are its relatively small sample size and it being a single-center, retrospective study. Multicentered, large studies may be helpful in evaluating the validity of RDW in patients with comorbidities. However, CVST is usually seen in young females with a small potential for comorbid diseases.
Per our study, a high initial RDW value may guide to CVST diagnosis in patients presenting with headache to ED or neurology outpatient units. One practical implication of our findings may be increasing the screening rate of MRI venography in patients with headache if they have a raised RDW value. Although widely accepted upper normal limit for RDW is 14%, in our study the 13.75 cut-off value increased the probability of CVST by 6.3-fold. When the cutoff value is 14.1, the probability of CVST increases almost by 93-fold. To conclude, sensitivity and specificity of high RDW values for CVST diagnosis is high in patients presenting with headache.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.