
Abstract
Podoplanin (PDPN) is known to play a role in thrombosis, metastasis of tumor cells, the epithelial–mesenchymal transition (EMT), and immune response. The present study aim to evaluate the clinical significance of soluble PDPN (sPDPN) in hypercoagulability and cellular immune status in patients with non-small cell lung cancer (NSCLC). Enzyme-linked immunosorbent assay (ELISA) was used to determine plasma sPDPN levels, and T-lymphocyte distribution was determined using flow cytometry. The levels of sPDPN were markedly higher in the NSCLC group than control group, and sPDPN was higher in patients with advanced-stage and with distant metastases. The high-sPDPN group had lower absolute numbers of CD3+, CD4+, and CD4+/CD8+ ratio than low-sPDPN group. Correlation analysis indicated that sPDPN was positively linked to platelet (r = 0.50, P < .001), D-dimer (r = 0.52, P < .001), and fibrinogen (r = 0.37, P < .001); and inversely correlated with CD3+ (r = −0.37, P < .001), CD4+ (r = −0.44, P < .001), and CD4+/CD8+ (r = −0.37, P < .001). Multivariate logistic regression analysis indicated that sPDPN (odds ratio [OR] = 2.293; 95% CI, 1.559−3.373) and tumor stage (OR = 15.857; 95% CI, 1.484−169.401) were separate risk indicators for hypercoagulability. The receiver operating characteristic curves (ROC) indicated that sPDPN had high diagnostic values for hypercoagulability in NSCLC patients. In conclusion, plasma sPDPN was not only linked to hypercoagulability, but it may also be an indicator of the body's cellular immune status in NSCLC patients.
Introduction
One of the most prevalent malignant tumors and the principle cause of cancer mortality worldwide is lung cancer. 1 According to cell origin, lung cancer is classified into 2 main histologic groups: small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC), with the latter accounting for ∼85% of all lung cancers. 2 It is widely recognized that people with cancer are more likely to experience thrombotic events,3,4 and individuals with lung cancer are at highest risk for these events. 5 Numerous studies have depicted that lung cancer as linked to hypercoagulability through activation of the coagulation and fibrinolytic systems. 6 The term “hypercoagulability” refers to a state of vascular endothelial injury, anticoagulation, and fibrinolytic dysfunction due to a variety of factors; and thrombotic events are prone to occur in this state. 7
Previous studies have revealed a marked correlation between the composition and function of the immune system and the development, progression, and prognosis of lung cancers.8–10 T lymphocytes are crucial in the cellular immune reaction, especially in anti-tumor immune response. T lymphocytes can be further classified as CD3+CD8+ and CD3+CD4+ according to their surface markers. 11 In lung cancer patients, peripheral CD8+ T-cell counts were higher than in healthy controls, but CD3+, CD4+ T cells, and the CD4+/CD8+ were considerably lower. 12 Additionally, individuals with lung cancer who had higher percentages of peripheral CD3+ and CD4+ T cells, and higher CD4/CD8 ratios, had longer overall survival times. 13
Podoplanin (PDPN) is a mucin-type transmembrane glycoprotein that is known to be a hallmark of lymphatic endothelial cells. 14 It is highly expressed by various types of tumor tissue and cells, including brain gliomas, 15 lung cancer, 16 pancreatic cancer, 17 breast cancer, 18 and gastric cancer. 19 PDPN is the unique internal ligand of C-type lectin-like receptor 2 (CLEC-2). 20 It has been determined that CLEC-2 is a receptor for the platelet (PLT)-activating snake venom rhodocytin, which is highly and virtually exclusively expressed in PLTs. The binding of PDPN to PLT CLEC-2 triggers PLT activation and aggregation. 21 Previous studies have illustrated that the expression of PDPN is linked to thrombosis, metastasis of cancer cells, inflammatory response, the epithelial–mesenchymal transition (EMT), lymphatic vessel production, and immune responses.22–27 Current research on plasma soluble PDPN is primarily focused on the diagnosis and prediction of distant metastases in lung cancer, with only a few studies on its association with hypercoagulability and the immunologic state. 28
In our study, plasma soluble PDPN (sPDPN) levels in a healthy control group (n = 40) and NSCLC group (n = 106) were measured with enzyme-linked immunosorbent assay (ELISA), and we then determined T-lymphocyte subsets to illustrate the clinical implications of sPDPN in hypercoagulability and cellular immune status in NSCLC patients.
Materials and Methods
Patient Selection
Patients were selected from the Second Affiliated Hospital of Xu Zhou Medical University between November 2021 and December 2022. Inclusion criteria are as follows: (i) age ≥18 and <80 years; (ii) patients with pathologically confirmed NSCLC; (iii) first diagnosis without any anti-tumor treatment; (iv) absence of other malignant tumors; and (v) complete clinical data. Exclusion criteria are as follows: (i) received anti-tumor therapy such as surgery or chemoradiation; (ii) acquired immune deficiency syndrome (AIDS) and autoimmune diseases; (iii) patients with previous heparin-associated thrombocytopenia, hematologic diseases, cerebrovascular diseases, chronic liver disease, and other diseases that affect coagulation function; (iv) a history of oral or intravenous hormone use in the previous month; and (v) a history of surgery, trauma, and burns within the previous 6 months and who received antiplatelet treatment. The Ethics Committee of the Second Affiliated Hospital of Xu Zhou Medical University approved this study, and informed consent was obtained from all individuals ([2021]111003).
Clinical Data Collection
A medical record management system was utilized to collect clinical and pathologic data, including age, sex, stage, smoking history, histology, and coagulation indicators (PLT, D-dimer, prothrombin time [PT], activated partial thromboplastin time [APTT], antithrombin [AT], and fibrinogen [FIB]). According to the 7th National Conference on Thrombosis and Hemostasis in China, hypercoagulability was defined as meeting at least 2 of the following criteria: FIB >4.0 g/L, D-dimer >550 μg/L, PLT >300 × 109/L, APTT shortened by >3 s, and PT shortened by >3 s.
Determination of Plasma sPDPN by ELISA
The ELISA method was used to determine the level of sPDPN. Commercial ELISA kits for sPDPN were obtained from Jianglaibio, Shanghai, China. All procedures were performed following the manufacturers’ instructions.
Analysis of T-Lymphocyte Subsets
We used Beckman Coulter FC-500 flow cytometer (Beckman Coulter, USA) to measure the levels of T-lymphocyte subsets. The antibodies used in this study were as follows: CD3 FITC/CD16+56-PE/CD45-PerCP-CY5.5/CD4-PC7/CD19-APC/CD8-APC-Cy7 fluorescent monoclonal antibodies (mAbs) (Beijing Tongsheng Times, China). All procedures were performed by strictly following the manufacturer's instructions.
Statistical Analysis
Our statistical analysis was conducted using SPSS (version 19), and we used R software (version 4.1.0) for constructing the figures. For continuous variables and after testing for normality, we described the data in terms of the mean ± standard deviation; otherwise, the median (Q1-Q3) was used. Categorical variables are shown as a frequency (percentage). We applied Student's t-test or a nonparametric test to compare quantitative data between 2 groups, and Pearson's correlation was applied to analyze the relationship between sPDPN and laboratory parameters. The influencing factors of hypercoagulability in NSCLC patients were analyzed using logistic regression analysis. Receiver operating characteristic (ROC) curves were adopted to assess the diagnostic value of sPDPN in the hypercoagulable state and to determine the optimal cutoff point based on the Youden index. A value of P < .05 was considered to be statistically significant.
Results
Demographic Information
As shown in Table 1, a total of 40 volunteers and 106 NSCLC patients were recruited for the present study. Compared with the controls, the NSCLC patients were old (P < .001) and had significantly high D-dimer and FIB levels and PLT counts. In contrast, there were lower CD3+, CD4+, and CD4+/CD8+ ratio in the NSCLC patients. We observed no difference with respect to sex, smoking history, APTT, or CD8+ T-cell count.
Baseline Information of Enrolled Patients.

Abbreviations: APTT, activated partial thromboplastin time; NSCLC, non-small cell lung cancer; PT, prothrombin time. Numbers in bold represent statistical significance.
Comparison of Plasma sPDPN Concentrations in NSCLC Patients and Healthy Individuals
The levels of sPDPN were markedly higher in the NSCLC group than those in the controls (Figure 1A). Additionally, plasma sPDPN was higher in cases with stage III + IV cancer than that in individuals at stage I + II (Figure 1B). A significant elevation in the sPDPN level was observed in the distant metastases group, compared with the group without metastases (Figure 1C).

The levels of sPDPN in NSCLC patients and healthy individuals. (A) The levels of sPDPN in NSCLC patients and controls. (B) The levels of sPDPN in patients at different cancer stages. (C) The levels of sPDPN in the non-metastatic and metastatic groups. *P < .05, **P < .01, ***P < .001. Abbreviations: NSCLC, non-small cell lung cancer; sPDPN, soluble podoplanin.
Correlation Between sPDPN Levels and T-Lymphocyte Subsets
We divided lung cancer patients into high-sPDPN and low-sPDPN groups based on the median of plasma sPDPN levels, and univariate analysis revealed that the absolute numbers of CD3+, CD4+, and CD4+/CD8+ ratio in high-sPDPN patients significantly decreased compared with those in the low-sPDPN patients (Table 2).
Differences in T-Lymphocyte Subsets Between the Two Groups With Low and High sPDPN Levels.

Abbreviation: sPDPN, soluble podoplanin. Numbers in bold represent statistical significance.
Correlations of Plasma sPDPN Levels With Coagulation Parameters and T-Lymphocyte Subsets in Patients With NSCLC
In the present study, correlation analysis indicated that sPDPN was positively linked to PLT count (r = 0.50, P < .001) and D-dimer (r = 0.52, P < .001) and FIB levels (r = 0.37, P < .001); and the level of sPDPN was negatively correlated with CD3+ (r = −0.37, P < .001), CD4+ (r = −0.44, P < .001), and CD4+/CD8+ (r = −0.37, P < .001) (the specific data are detailed in Figure 2).

Association of sPDPN with coagulation parameters and T-lymphocyte subsets in patients with NSCLC. The coagulation parameters consisted of PT, APTT, AT, FIB, D-dimer, and PLT. The T-lymphocyte subsets consisted of CD3+, CD4+, CD8+, CD4+/CD8+. Abbreviations: APTT, activated partial thromboplastin time; AT, antithrombin; FIB, fibrinogen; NSCLC, non-small cell lung cancer; PLT, platelet; PT, prothrombin time; sPDPN, soluble podoplanin. *P < .05, **P < .01, ***P < .001.
Analysis of Risk Factors for Hypercoagulability
The effect of clinical parameters on hypercoagulability was evaluated by employing logistic regression analysis. Univariate analysis showed that sPDPN (odds ratio [OR] = 2.216; 95% CI, 1.652-2.973), AT (OR = 0.970; 95% CI, 0.947-0.994), cancer stage (OR = 20.667; 95% CI, 5.732-74.508), metastases (OR = 18.750; 95% CI, 2.347-148.071), and smoking (OR = 3.193; 95% CI, 1.437-7.098) were related to hypercoagulability (Table 3). We then performed a multivariate analysis of the variables and showed that sPDPN (OR = 2.293; 95% CI, 1.559-3.373) and cancer stage (OR = 15.857; 95% CI, 1.484-169.401) were separate risk indicators and that AT (OR = 0.949; 95% CI, 0.910-0.989) was a protective factor for hypercoagulation (Table 3).
Associations Between Clinical Parameters and Hypercoagulability in Patients With NSCLC.
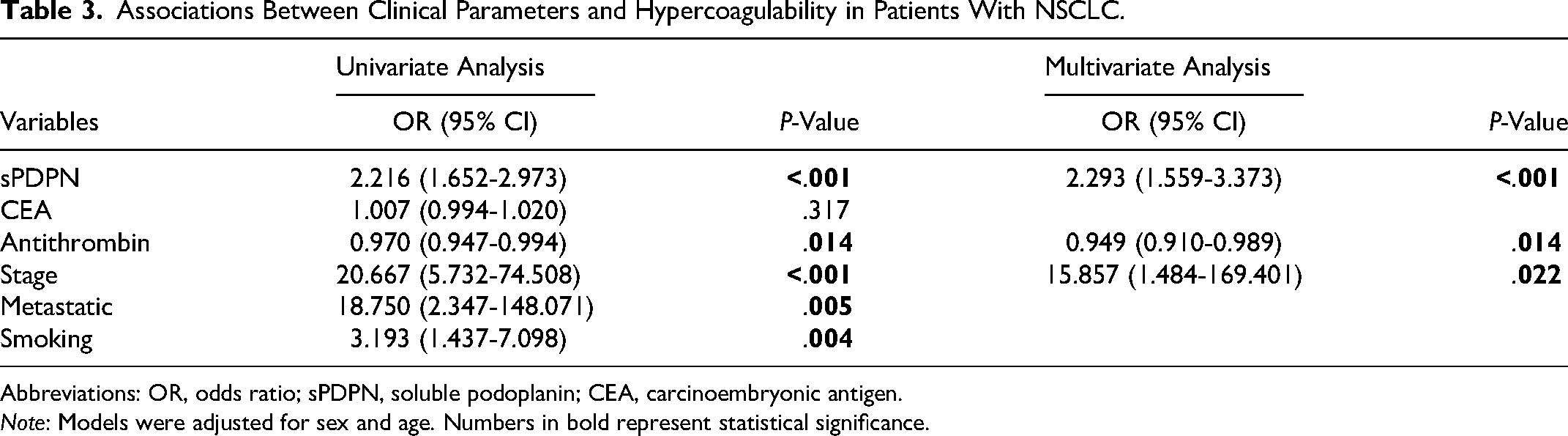
Abbreviations: OR, odds ratio; sPDPN, soluble podoplanin; CEA, carcinoembryonic antigen.
Note: Models were adjusted for sex and age. Numbers in bold represent statistical significance.
Predictive Utility of Clinical Parameters for Hypercoagulability
We used area under the ROC curve (AUC) to access the predictive utility of clinical parameters (including sPDPN, stage, and AT) for the hypercoagulable state. The AUCs for hypercoagulability of plasma sPDPN, stage, AT, sPDPN + AT, sPDPN + stage, stage + AT, and sPDPN + stage + AT were 0.908, 0.761, 0.662, 0.928, 0.920, 0.838, and 0.939, respectively (Figure 3). The optimal cutoff points were assessed using the Youden index, and optimal cutoff concentrations for sPDPN and AT were 9.43 ng/mL (at a sensitivity of 80% and specificity of 98%) and 87.3% (a sensitivity of 53% and specificity of 77%), respectively. The results of Delong test showed that compared with sPDPN alone for the diagnosis of hypercoagulation, the combined diagnosis was not statistically different (P all >.05), although the area under the curve increased.

ROC curves for hypercoagulability in patients with NSCLC were predicted by sPDPN, stage, and AT. Abbreviations: AT, antithrombin; AUC, area under the curve; NSCLC, non-small cell lung cancer; ROC, receiver operating characteristic; sPDPN, soluble podoplanin.
Discussion
A common complication in lung cancer patients is hypercoagulability. 29 A hypercoagulable state is characterized by elevated coagulation, diminished anticoagulation function, and impaired tissue fibrinolytic activity. 30 Patients with lung cancer typically manifest more severe coagulation abnormalities and a higher incidence of venous thromboembolism (VTE) than patients with other malignancies.31,32 Multiple coagulation factors and signaling pathways are involved in the mechanisms underlying the increased incidence of hypercoagulability in lung cancer patients. Procoagulant factors such as tissue factor and tumor procoagulant are expressed by cancer cells and are crucial for activating the coagulation cascade. 33 A recent meta-analysis conducted by Bayleyegn et al showed that lung cancer patients possessed a considerably greater PLT count and higher plasma D-dimer and FIB levels relative to the control groups. 34
PDPN has been shown to be upregulated in the subendothelial wall in certain pathologic states, causing PLT activation and thrombosis. 35 Furthermore, PDPN causes hypercoagulability by inducing PLT aggregation and activation by binding of its domain to CLEC-2 expressed on the PLT surface.36,37 Several recent studies have further confirmed that excessive levels of PDPN expression in cancer cells might cause PLT aggregation, increasing the risk of thrombosis.38,39 Payne et al 40 also reported that mice with reduced PDPN were protected from deep vein thrombosis. Hence, we speculate that increased PDPN expression is a sign of hypercoagulability and acts as a risk factor for thromboembolism in patients with NSCLC.
In the present study, we found that, compared with the controls, the cancer patients had markedly high levels of D-dimers, FIB, and PLT counts. Furthermore, we discovered that sPDPN levels in NSCLC patients were considerably higher than those in healthy individuals, which was congruent with the study by Zhao et al. 41 We then analyzed the correlation of sPDPN with coagulation parameters in NSCLC patients, and the results illustrated that sPDPN levels were correlated with levels of D-dimer and FIB and of PLT counts. The significant relationship between sPDPN and coagulation indices further supports the concept that patients with NSCLC may be more likely to experience hypercoagulability and thrombosis if their sPDPN level is elevated. To further confirm this, we analyzed the indicators that could influence coagulation state, with the goal of identifying risk factors for hypercoagulability. Logistic regression analysis showed that sPDPN was a risk factor for hypercoagulation, and ROC curve showed that sPDPN had the best predictive values for hypercoagulability in NSCLC patients (AUC = 0.908, sensitivity = 80%, and specificity = 98%) than stage and AT. In addition, the results of Delong test showed that the difference in AUC between the combined diagnosis and the sPDPN diagnosis alone was not significant. Therefore, we speculate that sPDPN—as with lupus anticoagulants (LACs), 42 P-selectin, 43 procoagulant phospholipid-dependent clotting time, 44 and coagulation factor XIII (F13A1) 45 —represents a novel hypercoagulable indicator with good predictive value for the hypercoagulable state in lung cancer; and we anticipate that it will be utilized in clinical practice in the near future.
Based on a previous investigation in which the authors evaluated the role of sPDPN in the hypercoagulable state in patients with nephrotic syndrome, 46 we hypothesized that PDPN might be released in a soluble form into the circulation of lung cancer patients. Carrasco-Ramirez et al 23 demonstrated that cells expressing PDPN also release mRNA vesicles that encode PDPN proteins as well as release sPDPN into patient plasma via exosomes into the external environment and multivesicular bodies in cells and that this may be a source of sPDPN in NSCLC patients. It is reported that VTE is the second leading cause of death in cancer patients and that it is closely correlated with tumor metastasis and poor prognosis. 47 Therefore, it is important to measure sPDPN and other coagulation parameters to evaluate the hypercoagulable state and undertake some measures to prevent VTE and other thrombotic events, if necessary, in patients with NSCLC.
We understand that cellular immunity serves as the primary mode of anti-tumor immunity in the body, and lymphocyte infiltration is the core of cellular immunity. It is currently believed that tumor onset, development, and prognosis are all linked to the body's immune status48,49; and some studies suggest that T-lymphocyte subsets has the potential to become a target for clinical immunotherapy of tumors as well as prognostic biomarkers.50,51 Studies showed that people with lung cancer are often immunosuppressed, with alterations in the number of lymphocyte subsets.52,53 Flow cytometry was used in our study to examine T-lymphocyte subsets in participants, and our results revealed that the absolute numbers of CD3+, CD4+, and CD4+/CD8+ ratio were significantly reduced in NSCLC patients but not in healthy controls, which was consistent with earlier reports.55,56 However, there is controversy regarding the changes in CD8+ cell counts in the blood of lung cancer patients, most likely because there are 2 types of CD8+ T cells: CD8+CD28− T cells and CD8+CD28+ T cells, exerting an opposite influence on the immune system. 54 In our study, we did not find differences in CD8+ counts between NSCLC and healthy cases; we suspect that the relatively small number of patients is one of the main reasons. To investigate the link between sPDPN and cellular immune function in NSCLC patients, we divided lung cancer patients into high-sPDPN and low-sPDPN groups based on the median of sPDPN levels and discovered that the high-sPDPN group had lower CD3+, CD4+, and CD4+/CD8+ cell counts. Moreover, to analyze the correlation between sPDPN and cellular immune status, we conducted correlation analyses between sPDPN and T-lymphocyte subsets; and according to our results, the level of sPDPN was inversely correlated with CD3+, CD4+, and CD4+/CD8+ ratio. As a result, our findings confirmed that sPDPN levels were associated with an abnormal distribution of T-lymphocyte subsets in the peripheral blood of patients with NSCLC, and this can indirectly reflect the body's cellular immune status. Previous studies have suggested that both CD4+ and CD8+ T cells express PDPN, which then acts as a coinhibitory receptor to reduce T-lymphocyte survival in the tumor microenvironment (TME). 55 Our research also showed that patients with elevated sPDPN levels had advanced stages of cancer and metastases and that immunosuppressive factors were present in the body, inhibiting lymphocyte differentiation and maturation and reducing the numbers of lymphocytes.
The role of PDPN in immunosuppression has been confirmed,24,56 and anti-PDPN mAbs are currently being used in the treatment of solid tumors. These mAbs bind to the PLAG domain and block PDPN–CLEC-2 interactions, thus abrogating PDPN-induced PLT aggregation and distant metastases of tumor cells.57,58 These findings indicated that anti-PDPN mAb is likely to become a novel tumor-targeting drug in the future. Chimeric antigen receptor T-cell immunotherapy (CAR-T) is a novel precision-targeted therapeutic modality for tumors. CAR-T cells were demonstrated to exert a highly specific inhibitory effect on PDPN-positive glioblastoma cells in vitro, and CAR-T cell injection in immunocompromised mice also slowed the growth of transplanted gliomas in vivo. 59 Whether CAR-T therapy is effective and specific in lung cancer patients who manifest high levels of sPDPN warrants further investigation. We believe that research into the mechanism by which PDPN transmits inhibitory signals in T cells will help researchers to better understand the molecular basis of PDPN immunosuppression and that it will provide new avenues in tumor immunotherapy.
Our study had some limitations. First, due to a relatively small number of patients, the generalizability of our findings is limited, and more studies are needed in the future. Second, although the binding of PDPN to CLEC-2 promotes PLT aggregation and activation that leads to hypercoagulable states, we did not measure specific markers of PLT activation such as glycoprotein VI (GPVI) and CD62P. We realize that our findings must also be confirmed by additional research. Third, immune function changes may not always be reflected as changes in the absolute numbers of immune cells. Lymphocyte functions should therefore be further examined to support our findings.
Conclusion
Our findings suggest that plasma soluble sPDPN levels are closely associated with a hypercoagulable state and that they exhibit a favorable predictive value of the hypercoagulable state in NSCLC patients. Additionally, sPDPN levels were related to an abnormal distribution of lymphocyte subsets in the peripheral blood of patients with NSCLC, and this could indirectly reflect the body's immune status. Anti-tumor drugs that target PDPN action are currently being developed, and we hypothesize that such drugs also improve anti-tumor effects by altering the hypercoagulable state and cellular immune status of patients with NSCLC.
Footnotes
Author Contributions
Jie Zhao and Yan-Min Zhang contributed to the study conception and design. Material preparation and data collection were performed by Qian Zhang, Kun Peng, and Jing-Ying Huang. Ru-Yu Zhang, Li-Hong Xin, and Lin Wang conducted statistical analyses of this work. Lin Wang provided financial and technical support for this study. The first draft of the manuscript was written by Qian Zhang and Kun Peng. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Youth Medical Science and Technology Innovation Project of the Xuzhou Municipal Health Commission, Development Fund of Affiliated Hospital of Xuzhou Medical University (grant numbers XWKYHT20210565 and XYFY2020051).