
Abstract
Keywords
Introduction
Deep vein thrombosis (DVT) is defined as an obstructive disease, its formation mechanism is that abnormal blood clots form in the deep vein vessels, which further block the blood vessels of lower limbs and hinder venous reflux. It is relatively common in the elderly patients with fractures and bedridden, mainly occurring in lower limbs. 1 Among them, lower extremity DVT (LEDVT) is a serious multi-factor fatal disease with an annual incidence of 45 to 117 cases per 100,000 persons. 2 The mortality rate is as high as 6% within one month after diagnosis of LEDVT. 3 With the increasing morbidity and mortality of LEDVT, several preventions and treatments have been applied in recent years. It is essential for clinicians to identify potential markers which may predict the risk of LEDVT so as to carry out targeted treatments and improve patients’ quality of life.
DVT with endothelial dysfunction would further lead to atherosclerosis (AS), 4 which indicates that there may be a correlation between DVT and AS, and DVT patients may have an increased risk of subsequent AS.5,6 Circulating blood lipid levels have been confirmed to be strongly associated with the risk of atherosclerosis (AS).7–11 However, whether dyslipidemia is related to DVT is yet to be identified. Some studies have found that hyperlipidemia may increase the risk of DVT,12,13 whereas other studies found that the associations between blood lipid levels and the risk of DVT were uncertain 14 or even irrelevant. 15 Furthermore, current studies have mainly investigated the associations between blood lipid levels and secondary LEDVT following surgery, and the evidence regarding the associations between blood lipid levels and primary LEDVT remains scarce and has so far yielded inconclusive results. This study aimed to assess the potential associations between blood lipid levels and the risk of LEDVT to identify high-risk individuals, which may provide a reference for clinical applications of anticoagulant LEDVT treatment.
Methods
Study Population and Design
The demographic and clinical characteristics of 984 patients from the electronic health record in Changzhou First People's Hospital, Jiangsu province, China between January 2016 and May 2020 were enrolled. The study was approved by the Ethics Committee of the Third Affiliated Hospital of Soochow University and informed consent was taken from all the patients. The diagnostic criteria of LEDVT were based on the “Guidelines for the Diagnosis and Treatment of Deep Vein Thrombosis (third edition)” published by the Vascular Surgery Group of the Chinese Medical Association Surgery Branch. 16
The inclusion criteria were as follows: (1) age ≥ 18 years; (2) the case group: participants were diagnosed with primary LEDVT for the first time and without any obvious inducement; the control group: participants without a history of venous thromboembolism or AS. All included case group patients had acute LEDVT, which was confirmed by objective tests such as venography or duplex ultrasonography.
The exclusion criteria were as follows: (1) congenital or acquired coagulopathy, or hemoglobinopathy; (2) anticoagulant therapy, and steroid, hormones, or lipid-lowering medications before blood test; (3) a history of blood diseases, such as hemophilia, thrombocytopenia, or purpura leukemia; (4) liver or kidney dysfunction; (5) a history of malignant tumors within 5 years; (6) a recent history of major surgical trauma; (7) presented with bleeding or thromboembolic episodes before the study for six months, such as cerebral hemorrhage, cerebral infarction, or myocardial infarction.
Data Acquisition
The general data were collected, including age, sex, body mass index (BMI), disease course, ill position, smoking history, history of current illness, and drug use. The laboratory indicators were also collected, including triglyceride (TG), total cholesterol (TC), HDL cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), activated partial thromboplastin time (APTT), thromboplastin time (TT), prothrombin time (PT), and fibrinogen (FIB), neutrophils (NEUT), platelet (PLT), and lymphocyte (LY).
Blood Collection and Measurement
All patients were emergency admissions. Fasting venous blood samples were collected from patients after admission, and then odium citrate anticoagulated plasma and non-anticoagulant serum were prepared. Plasma amples were used for the detection of APTT, TT, PT, and FIB using Sysmex CS-5100 automated coagulation analyzer (Sysmex, Japan). Serum samples were utilized for the detection of TG, TC, HDL-C, LDL-C, and ApoA1/B by a AU5831 Biochemical Analyzer (Beckman Coulter, American). All operation procedures were strictly implemented in accordance with the instrument operation manual.
Statistical Analysis
All statistical analyses were performed by SPSS Statistics version 23.0 (Armonk, NY: IBM Corp.). Continuous variables were represented by the mean ± standard deviation (Mean ± SD) or median with interquartile spacing [M (Q1, Q3)], and the independent samples t-test/Mann-Whitney U test was used for intergroup comparison. Categorical variables were described by the number of cases/constituent ratio [N (%)], and χ2 test or Fisher's exact test was adopted for intergroup comparison. Univariate and multivariate logistic regression analyses were used to assess the associations between the blood lipid levels and the risk of LEDVT. The odds ratio (OR) with 95% confidence intervals (CIs) were calculated in the multivariate regression model. P<0.05 was considered statistically significant.
Results
Baseline Features
In this study, a total of 500 subjects were eventually selected from 984 participants based on inclusion and exclusion criteria, including 246 cases and 254 controls. The detailed flow chart of data screening was shown in Figure 1. Compared with the control group, the average age of patients in the LEDVT group was higher (t = −6.395, P<0.001). Additionally, the proportion of patients with hypertension in the LEDVT group was significantly higher than that in the control group (χ2 = 7.328, P = 0.007). Compared with the control group, the levels of NEUT (Z = −12.679, P<0.001), TG (Z = 3.031, P = 0.002), APTT (Z = −2.972, P = 0.003), and FIB (Z = −6.196, P<0.001) in the LEDVT group were significantly increased, while the level of HDL-C (Z = −5.845, P<0.001), LDL-C (Z = −1.993, P = 0.046), ApoA1 (Z = −9.192, P<0.001), ApoB (Z = −2.218, P = 0.027), and TT (Z = −12.689, P<0.001) in the LEDVT group were lower. The Baseline characteristics were shown in Table 1.
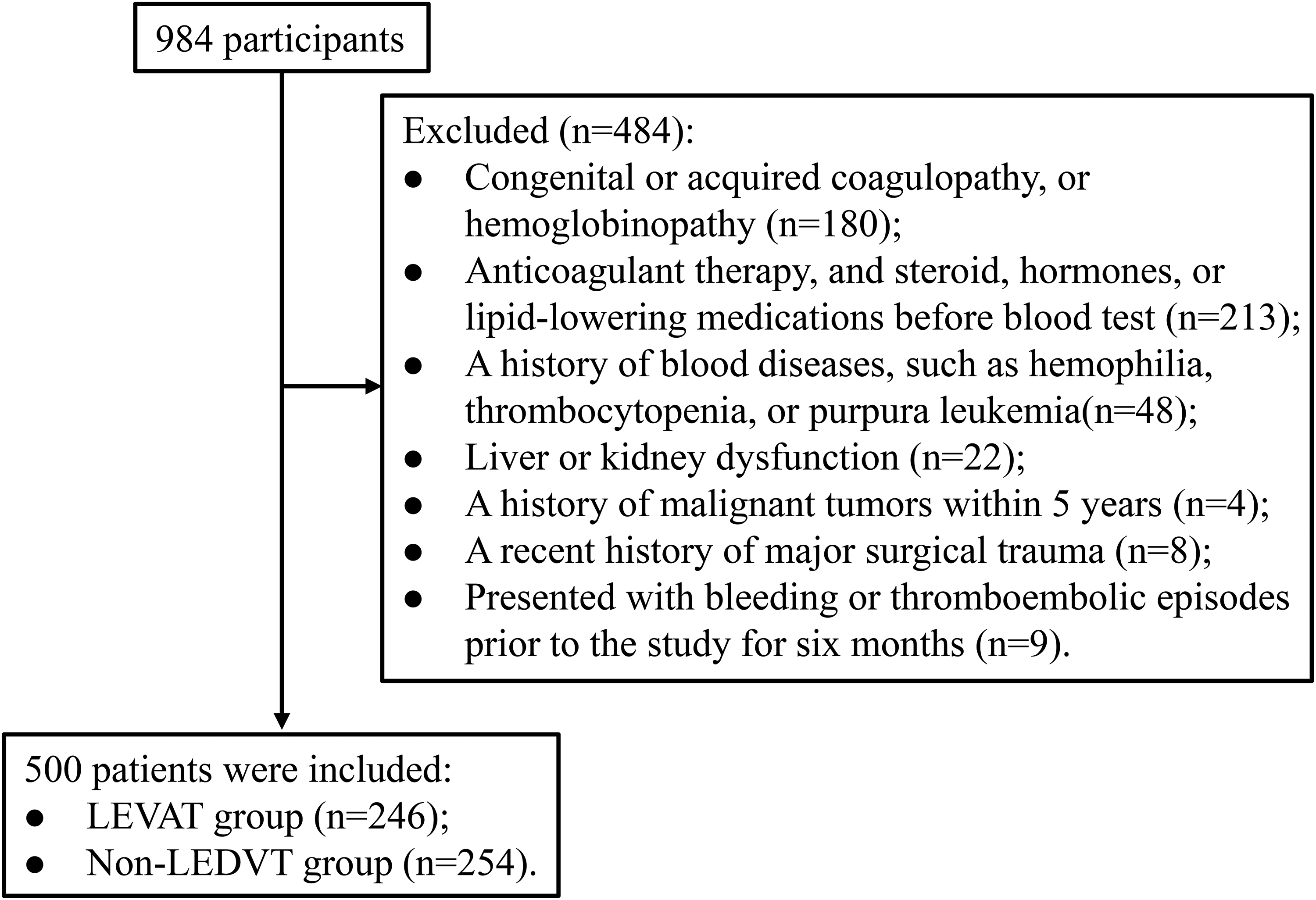
Flowchart of data filtering.
Baseline Characteristics.

Note. The data are represented as the mean ± standard deviation (M ± SD) or median with interquartile spacing [M (Q1, Q3)] for measurement data or as a numerical proportion for count data. LEDVT, lower extremity deep venous thrombosis; BMI, body mass index; PLT, platelet; NEUT, neutrophils; LY, lymphocyte; TG, triglyceride; TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C, low density lipoprotein cholesterol; ApoA1, apolipoprotein A1; ApoB, apolipoprotein B; APTT, activated partial thromboplastin time; TT, thromboplastin time; PT, prothrombin time; FIB, fibrinogen.
Associations Between Blood Lipid Levels and LEDVT
Table 2 shows the results of multivariate logistic regression analysis after adjusting the covariates (age, sex, hypertension, NEUT, APTT, TT, and FIB). The risk of LEDVT in patients with HDL-C levels of 0.965 to 1.14 mmol/L, 1.14 to 1.36 mmol/L, and > 1.36 mmol/L was 0.366 (95%CI: 0.179 to 0.749), 0.183 (95%CI: 0.087 to 0.385), 0.203 (95%CI: 0.096 to 0.431) times that of patiens with HDL-C<0.965 mmol/L, respectively (P<0.05). The risk of LEDVT in patients with ApoA1 levels of 1.06 to 1.22 mmol/L, 1.22 to 1.38 mmol/L, and > 1.38 mmol/L was 0.146- (95%CI: 0.063 to 0.340), 0.057- (95%CI: 0.024 to 0.135), and 0.059-fold (95%CI: 0.024 to 0.144) that of patients with ApoA1<1.06 mmol/L. The risk of LEDVT in patients with TG levels of 0.985 to 1.37 mmol/L, 1.37 to 1.91 mmol/L, and >1.91 mmol/L were 2.243 (95% CI: 1.094 to 4.599), 2.224 (95%CI: 1.091 to 4.535), and 2.540 (95%CI: 1.251 to 5.155) times higher than that of those with TG level<0.985 mmol/L, respectively. The risk of LEDVT in subjects with TC level of 4.57 to 5.17 mmol/L was 0.471-fold comparison than that of those with TC<3.97 mmol/L (OR = 0.471, 95%CI: 0.234 to 0.947).
Results of Univariate and Multivariate Logistic Regression Analysis on the Associations Between Blood Lipids and LEDVT.

Note. Multivariate analysis adjusted for age, sex, hypertension, neutrophils, activated partial thromboplastin time, thromboplastin time, and fibrinogen. OR, odds ratio; CI, confidence interval; TG, triglyceride; TC, total cholesterol; HDL-C, high density lipoprotein cholesterol; LDL-C low density lipoprotein cholesterol, ApoA1, apolipoprotein A1; ApoB, apolipoprotein B.
Discussion
In the present study, we investigated the associations between the blood lipid levels and LEDVT, overall results showed that high HDL-C and ApoA1 levels were associated with the decreased risk of LEDVT, but high TG levels were associated with increased risk of LEDVT. Besides, within the normal range, high TC levels were associated with decreased risk of LEDVT, independent of known LEDVT risk factors such as age, hypertension, NEUT, APTT, and FIB.
The anti-thrombotic properties of HDL-C were reported in both the arteries and veins.17,18 A meta-analysis showed that patients with low HDL-C levels are more likely to develop DVT. 19 Moreover, the level of HDL-C was also lower in patients with recurrent venous embolism. 20 The previous studies are consistent with our results, indicating that raising HDL-C level may be a vital therapeutic strategy to reduce the risk of LEDVT. The property of HDL-C on reducing the risk of thrombosis was based on several mechanisms, including reduced platelet sensitivity to aggregation and weakened activation of the coagulation cascade. HDL-C could stimulate the endothelial production of nitric oxide and prostacyclin which are potent inhibitors of platelet activation, attenuate vascular expression of tissue factor, and inactivate coagulation factors by potentiating the action of activated protein C: protein S. 21 This would decrease the production of thrombin, a powerful inducer of platelet, and the formation of fibrinogen. 22
Fewer reports have addressed the associations between DVT and levels of ApoA1. Two studies14,15 showed no correlation between apolipoprotein and DVT risk. However, apolipoprotein was related to DVT in specific subgroups. For example, low ApoA1 levels were associated with increased DVT risk in male patients. 12 Another study indicated that high ApoA1 levels increased the risk of DVT in female patients who use hormones. 23 Our current research found that high ApoA1 levels were associated with decreased risk of LEDVT after adjusting the covariates. It was reported that ApoA1 could efficiently reduce the risk of DVT via activating endothelial nitric oxide synthase (eNOS) through binding endothelial receptor scavenger receptor-BI (SR-BI). 24 A previous study indicated that ApoA1 could inhibit clot formation by inhibiting platelets, 25 which may explain our results.
A meta-analysis indicated that statistically significant association was observed between high TG levels and DVT risk. 19 Additionally, Xu et al found that postoperative high TG levels were associated with increased risk of DVT. 26 However, whether the blood lipid levels are related to LEDVT remains controversial. Other studies failed to demonstrate any correlation between serum TG level and DVT.27,28 Our results were in accordance with former studies after adjusting the confounding factors, which showed that higher TG level was a risk factor for LEDVT development. Although the exact mechanism was unclear, TG was believed to partial upregulate the levels of coagulation factor VII, VIII, and IX, and plasminogen activator inhibitor-1, which might result in abnormal clotting of the blood.29,30
Our results also found that higher TC levels within the normal range were associated with a decreased risk of LEDVT. Under physiological conditions, cholesterol is essential for excitation-contraction coupling of skeletal muscles 31 and normal muscle contraction maintenance. And muscle pumps are critical in maintaining blood flow, especially in the legs. When the muscles in the limbs fail to contract normally, the blood flow in some veins slows down or even stops entirely, which was related to an increased risk of DVT. 32 In addition, cholesterol is an essential part of the endothelial cell membrane, which is of great significance for stabilizing vascular permeability and maintaining normal endothelial barrier functions. The functions of the endothelial barrier may be impaired if the level of cholesterol is too low, and tissue factors stored under the endothelium might be abnormally released into the blood, thereby activating the exogenous blood coagulation pathway and promoting thrombosis. Therefore, maintaining a higher TC level within the normal range could reduce the risk of LEDVT.
The present study has some limitations. First, it was a retrospective study and could not rule out residual confounding. Some covariates that were statistically significant in univariate analysis in the final multivariate regression analyses such as age, sex, hypertension, NEUT, APTT, TT, and FIB have been adjusted. Second, low cholesterol levels have been confirmed to be associated with some chronic disease conditions, such as malignancy, rheumatic disorders, and hyperthyroidism. In this study, subjects with malignancy were eliminated to ensure the reliability of our results. Third, blood lipid levels we analyses were collected on admission, after which time they might be affected by the naturel course of plasma lipids or lifestyle interventions. Fourth, mutation in factor V Leiden lead to a markedly increased risk of DVT, but our study did not detect it. However, studies have shown that the prevalence of factor V Leiden mutation is low in China, approximately 0.1%-0.2%.33,34 The low prevalence of factor V Leiden mutation in China may not affect the accuracy of our results.
Conclusion
This study found that high HDL-C and ApoA1 levels were associated with decreased risk of LEDVT, but high TG levels were associated with increased risk of LEDVT. Besides, within the normal range, high TC levels were associated with decreased risk of LEDVT. Given that these blood lipid levels could be readily obtained during a physical examination or routine medical examination, clinicians may be more likely to early identify and timely treat patients at high risk of LEDVT, so as to improve patients quality of life.
Footnotes
Acknowledgements
Yiming Huang and Hongwei Ge designed the experiments. Yiming Huang and Xin Wang analyzed patient clinical data. Yiming Huang and Xiaoying Zhang wrote the paper. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Changzhou Municipal Health Commission, (grant number QN201912)
Ethics Approval
Ethical approval to report this case series was obtained from Changzhou First People's Hospital. (Ref. No.107,2020).
Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.