
Abstract
In the recent years, there has been significant transformation in the management of valvular heart disease (VHD), as a result of new minimally invasive technologies, such as the transcatheter aortic valve implantation (TAVI). Conventionally, mechanical heart valves require anticoagulation with warfarin to prevent thrombogenic events. Lately, there has been an uptrend in the usage of direct-acting oral anticoagulants (DOACs) in both mechanical and bioprosthetic heart valves. In clinical practice, there has shown to be notable heterogeneity in the antithrombotic regimen for patients. Recommendations from clinical guidelines and emerging data on DOAC use in these settings will be critically reviewed here. Future large, randomized-controlled trials are warranted to delineate the role of DOACs in patients receiving a bioprosthetic valve/TAVI or mechanical heart valve, with and without a baseline indication for anticoagulation or antiplatelets. Until clinical trial data from well-designed studies are available, providers must remain vigilant about DOAC use in patients with VHD, especially in patients with a bioprosthetic or mechanical heart valve.
Introduction
Valvular heart disease (VHD) describes any abnormality in the anatomy or function of a valve, which includes the mitral, aortic, pulmonary, and tricuspid valves. 1 Worldwide, the epidemiology of VHD is most commonly attributable to rheumatic heart disease; in the setting of untreated streptococcal infection, rheumatic fever may occur, and consequently, inflammation and scarring of the heart valve, primarily in the mitral valve. 2 On the contrary, in the United States and other higher-income countries, the availability and accessibility of effective antibiotics for streptococcal infections shift the predominating epidemiology to valvular degeneration and calcification, both of which have been associated with the normal aging process.1,2
In the United States, VHD affects approximately 3% of the population and causes up to 30,000 deaths annually; whereas worldwide, VHD in the manifestation of rheumatic heart disease affects roughly 5% of the population and causes over 300,000 deaths annually.1–4 Mortality is primarily resultant of complications related to blood pooling or stasis, as well as fragments of the diseased valves embolizing—causing heart failure, stroke, myocardial infarction, and venous thromboembolism. The most commonly affected valves are the mitral and aortic, due to higher sheer stress on the left side of the heart. The majority of deaths emerge from disease in the aortic valve. 3
Diseased valves can be replaced surgically with a mechanical or bioprosthetic valve, or implanted with a bioprosthetic valve by way of the transcatheter approach. Management of VHD has been customarily in the form of surgical valve repair and replacement, both of which are considered invasive. In the recent years, significant technological advances with less invasive transcatheter heart valve procedures have transformed the management of VHD. 1 Reductions in morbidity and mortality have been observed with procedures involving the MitraClip, and either comparable or lower stroke and mortality rates with transcatheter aortic valve implantation (TAVI).5–7 There are inherent advantages and complications which each surgical and transcatheter approach, such as the ability to forgo anticoagulation with TAVI, but greater long-term durability with surgically placed mechanical valves.8–10 Studies were screened from 2010 to April 1, 2022 in Medline, Embase, and the Cochrane Library. Journals were hand-searched for relevant articles, abstracts, and conference proceedings. Additionally, ClinicalTrials.gov was screened for pertinent clinical trial data.
Selection Between a Mechanical and Bioprosthetic Heart Valve
The rationale for the decision between a mechanical and bioprosthetic heart valve is constructed on the results of a large, randomized Veteran Affairs trial in 2000. 11 In this study, 575 patients receiving an aortic or mitral valve replacement were randomized to a bioprosthetic or the Bjork-Shiley spherical disc mechanical prosthesis, an older generation mechanical valve. After 15 years, the all-cause mortality was significantly reduced in the mechanical aortic valve group compared to the bioprosthetic aortic valve group (p = 0.02). However, the latter group had a significantly higher rate of primary valve failure, especially in those <65 years (p < 0.001), and higher reoperation rate (p < 0.004). Additionally, the bleeding rate was significantly higher for the mechanical valve group due to the required use of anticoagulation.
A more recent retrospective, propensity-matched cohort study of 4253 patients between 50 and 69 years old showed similar results.
12
There was a higher reoperative rate and lower rate of major bleeding with the bioprosthetic compared to the mechanical valve, and comparable rates of stroke and 15-year survival between the two groups. In accordance with these studies, typically, a mechanical valve is preferred if a patient is <65 years, has an acceptable risk of bleeding due to the necessity of anticoagulation, and already has a baseline indication for anticoagulation. On the other hand, a bioprosthetic valve is preferred in patients
Anticoagulation for Mechanical Heart Valves
Anticoagulation is required for mechanical heart valves to prevent valve thrombosis and currently, the only available option is warfarin with the international normalized ratio (INR) goal being dependent on the type of valve, valve location, and risk factors for thrombosis (Table 1).8–10 There is no established role for direct-acting oral anticoagulants (DOACs) currently in these patients with mechanical heart valves, regardless of the presence of other indications such as venous thromboembolism and non-valvular atrial fibrillation.13–16 To prevent any ambiguity, the 2021 guideline update by the American College of Cardiology and American Heart Association clarified the term “nonvalvular atrial fibrillation” as not implying that VHD is completely absent; rather, “nonvalvular atrial fibrillation” indicates atrial fibrillation in the absence of moderate or severe mitral stenosis and mechanical heart valves—because patients with either of these two conditions were excluded from the key DOAC trials. 17

Abbreviation: international normalized ratio (INR), thromboembolism (TE).
*TE risk factors include previous history of thromboembolism, hypercoagulability, dysfunctional left ventricle, or atrial fibrillation.
†Lower INR goal approved by the United States Federal Drug Administration in 2015.
From the early stages, major DOAC trials have excluded patients with mechanical heart valves on the basis of the RE-ALIGN study. 18 In the phase-II dose-validation study, 252 patients with mechanical aortic or mitral valves were randomized 2:1 to dabigatran or warfarin, respectively. Dabigatran was dose-adjusted based on renal function, and the INR goal was consistent with guideline recommendations.8–10 After 12 weeks, the study was halted prematurely due to an excess of stroke and bleeding in the dabigatran group. Higher rates of thromboembolic events were found in patients receiving dabigatran within 7 days of valve surgery, compared to initiating dabigatran 3 months after valve surgery. Upon analysis of plasma trough levels of dabigatran, thromboembolic events were found with both lower and higher trough levels, indicating lack of correlation between plasma level and thromboembolic risk. The time-in-therapeutic range (TTR) of warfarin, a commonly used marker to assess the quality of warfarin therapy, was about 50% in the RE-ALIGN study. This TTR is lower than rates that are typically recommended, which is at least 60-70%, and also lower than rates observed in other major DOAC trials for atrial fibrillation.19–22
The excess stroke risk for dabigatran may be explained by the pharmacological differences between warfarin and dabigatran. Warfarin inhibits tissue factor-induced coagulation via factor VII, contact pathway-induced coagulation via factor IX, common pathway-induced coagulation via factors X and II, and proteins C and S. On the contrary, dabigatran inhibits thrombin exclusively.23,24 Due to warfarin's ability to inhibit more broadly, especially the tissue factor that may play a key role in the pathophysiology of mechanical valve-induced thrombosis, warfarin may offer greater protection against ischemic events compared to dabigatran.23,24
The excess bleeding risk seen in the dabigatran arm may be linked to the pharmacokinetic properties of dabigatran. Dabigatran is a prodrug, and following oral administration, is 6% bioavailable. Consequently, the residual amount of dabigatran due to incomplete absorption may cause direct topical anticoagulant effects as it advances through the gastrointestinal tract.25,26 This is in contrast to warfarin, which is 95% absorbed, and it is not known to cause any direct topical anticoagulant activity in the gastrointestinal tract. 27 Due to excess risk of stroke and bleeding, dabigatran has a contraindication for use in patients with mechanical heart valves. 13 Since this trial, there have been limited trials on DOACs in mechanical heart valves—thus apixaban, edoxaban, and rivaroxaban carry a warning for, but not contraindication against, use in this population.14–16 There exists small-scale safety studies for rivaroxaban, and a summary of data on DOACs in mechanical heart valves is presented in Table 2.
Summary of Studies for DOACs in Mechanical Heart Valves.

Abbreviation: direct-acting oral anticoagulant (DOAC).
Bioprosthetic Heart Valves/TAVI with Concurrent Indication for Anticoagulation
Unlike with mechanical heart valves, DOACs are an option per the American and European guidelines for patients with bioprosthetic heart valves/TAVI, with several noteworthy caveats.8–10 Generally, long-term antithrombotic therapy in patients with bioprosthetic heart valve or TAVI can be limited to a single life-long antiplatelet agent. Long-term anticoagulation is not necessary unless the patients have another indication or comorbidity.8–10 Higher risks of thrombosis during the first 3 to 6 months postoperatively may require temporary treatment with warfarin, a DOAC, or dual antiplatelet therapy (DAPT).8–10 A single antiplatelet can be used for patients with unacceptably high bleeding risks, though it is less preferred.
The recommendation is to continue anticoagulation therapy with either warfarin or a DOAC without adding other antithrombotic agents in patients who were already taking an anticoagulant prior to TAVI in the absence of any recent coronary stenting (eg <3 months). 9 In patients with a recent coronary stent, it is advised to take a single antiplatelet in addition to the original anticoagulant (either warfarin or a DOAC) as dual therapy for 1-6 months. Afterward, the patient can be continued on monotherapy with the original anticoagulant, which is consistent with the updated 2021 North American consensus for post-stent management in patients with atrial fibrillation. 32
These recommendations are primarily derived from subgroup analyses of the landmark DOAC trials in atrial fibrillation. In a post-hoc subgroup analysis of ARISTOTLE, 82 patients with bioprosthetic valves
Summary of Studies for DOACs in Bioprosthetic Heart Valves/TAVI with Concurrent Indication for Anticoagulation.
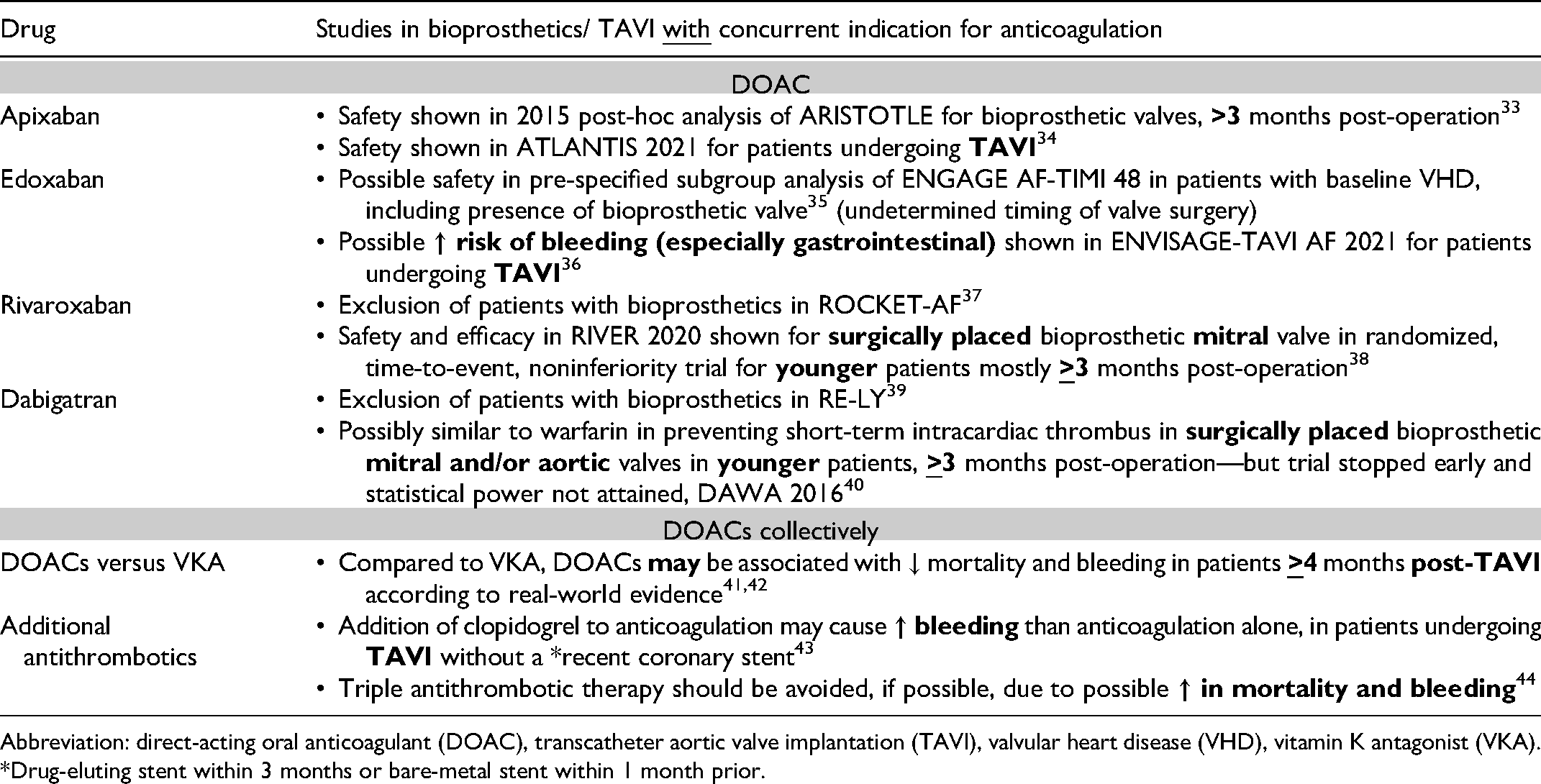
Abbreviation: direct-acting oral anticoagulant (DOAC), transcatheter aortic valve implantation (TAVI), valvular heart disease (VHD), vitamin K antagonist (VKA).
*Drug-eluting stent within 3 months or bare-metal stent within 1 month prior.
Apixaban
For that reason, the subsequent ATLANTIS trial 2021 was conducted to assess the impact of apixaban in patients undergoing TAVI with and without a baseline indication for anticoagulation. 34 In this phase III, open-label, randomized, superiority study, patients were stratified by presence (n = 451) or absence of an indication for anticoagulation (n = 1049). Notable exclusion criteria included coronary stenting within 2 weeks and glomerular filtration rate (GFR) <15 ml/min or on hemodialysis. The mean age was 82 years, which is consistent with the general TAVI population in clinical practice. At baseline, 27% had atrial fibrillation, 26% had a prior coronary stent, and the mean GFR was 62 ml/min.
The stratum of patients with an indication for anticoagulation was randomized to either vitamin K antagonist or apixaban (exact timing from TAVI procedure unknown). 34 At 1 year, in a post-hoc analysis, apixaban was not superior to vitamin K antagonist for the primary composite outcome, which included time to death, stroke, myocardial infarction, systemic emboli, intracardiac or valve thrombosis, venous thromboembolism, and major bleedings (HR 1.02, 95% CI 0.68-1.51). Safety outcomes were similar between the groups. The study investigators surmise that apixaban is a reasonable option in place of warfarin for patients requiring anticoagulation undergoing TAVI.
Edoxaban
ENGAGE AF-TIMI 48 was the key trial comparing edoxaban versus warfarin in patients with atrial fibrillation. A subgroup analysis of ENGAGE AF-TIMI 48 compared patients with (n = 2824) and without VHD (n = 18,222) using pre-specified outcomes. Notably, only 0.9% (n = 191) of the total population had a bioprosthetic valve (exact timing from operation unknown). 35 After adjusting for differences in baseline characteristics, the presence of VHD was associated with increased risk of death, major adverse cardiovascular events, and major bleeding. However, relative differences were not noted between the edoxaban and warfarin groups. Lack of statistical power and possibility of residual confounding may exist as expected of this study design.
The recent ENVISAGE-TAVI AF trial actually illuminated the safety concerns of edoxaban in patients with bioprosthetic valves and a baseline indication for anticoagulation. 36 In this multicenter, randomized, prospective, open-label, noninferiority study, 1426 patients with pre-existing atrial fibrillation were given edoxaban or warfarin within 12 h to 7 days after successful TAVI. The primary efficacy outcome was a composite of net adverse clinical events, which included death from any cause, myocardial infarction, ischemic stroke, systemic thromboembolic event, valve thrombosis, or major bleeding. The mean age was 82 years, consistent with the target population for TAVI. Roughly half the patients were on concomitant antiplatelets, and the TTR for warfarin was acceptable at 64%.
After a median duration of follow-up of 18 months, edoxaban was noninferior to warfarin for the primary efficacy outcome (HR 1.05, 95% CI 0.85-1.31, noninferiority margin 1.38; p = 0.01 for noninferiority). However, the primary safety outcome of major bleeding was higher in the edoxaban group (HR 1.4, 95% CI 1.03-1.91, noninferiority margin 1.38; p = 0.93 for noninferiority). 36 Of major bleeding types, gastrointestinal bleeding was most notable despite similar rates of proton-pump inhibitor usage. Occurrence of intracranial hemorrhage and fatal bleeding were similar between the groups. Limitations include possible reporting bias given the open-label nature of the study and probable interference with routine monitoring associated with COVID-19 pandemic. Nevertheless, this study suggests possible safety concerns for edoxaban, especially gastrointestinal bleeding. Similarly to the theoretical mechanism for dabigatran-induced gastrointestinal bleeding discussed previously, edoxaban is 50% bioavailable and the unabsorbed drug may have direct topical anticoagulant effects in the gastrointestinal tract until it is excreted unchanged in the feces.25,26
Rivaroxaban
The early landmark trial with rivaroxaban in atrial fibrillation patients, the ROCKET-AF trial, excluded all patients with artificial valve prostheses, including bioprosthetics. 37 More recently, the RIVER trial was published and it was an open-label, noninferiority trial randomizing 1005 patients with atrial fibrillation to rivaroxaban or warfarin at least 48 h following bioprosthetic mitral valve implantation. 38 The primary outcome was a composite of death, major cardiovascular events, or major bleeding at 12 months, as calculated per the restricted mean survival time (RMST) method. The TTR was acceptable at 65.5% and the study had almost complete follow-up. The mean age was 59 years, with only 35% of the study population at least 65 years old. It is not known how many study patients were 75 years or older, which is more representative of typical TAVI patients.
The mean time until the occurrence of a primary-outcome event for rivaroxaban was noninferior to that of warfarin (RMST difference 7.4 days, 95% CI − 1.4 to 16.3, p < 0.001 for noninferiority). 38 The rate of major bleeding was also noninferior for rivaroxaban compared to warfarin (HR 0.54, 95% CI 0.21-1.35). It is vital to note that most of the patients (approximately 80%) were randomized at least 3 months after mitral valve implantation, and thus were considered stable and at lower risk of thrombotic events. Further, given the open-label design, performance and reporting bias may be present, and results cannot be extrapolated to patients with bioprosthetic aortic valves.
Dabigatran
After harm was seen in the dabigatran arm in the RE-ALIGN trial, patients with prosthetic heart valves, including bioprosthetic, were excluded from the RE-LY study.18,39 The effects of dabigatran in patients with prosthetic heart valves were not studied again until the DAWA study. This was a phase II, randomized, prospective, open-label, pilot study of dabigatran versus warfarin for post-operative atrial fibrillation in patients with a surgically placed mitral and/or aortic bioprosthetic valve placed
Registry Data of DOACs Collectively
Recent registry studies aimed to characterize the safety and efficacy of DOACs compared to a vitamin K antagonist in patients post-TAVI with a concurrent indication for anticoagulation, primarily atrial fibrillation.
41
OCEAN was an observational, prospective, propensity score-matched study of registry data from 2013 to 2017 among 14 hospitals in Japan. In 403 patients with atrial fibrillation post-TAVI, 56% were on DOACs (unspecified type) and the remaining were on a vitamin K antagonist. The mean age was 84.4 years, which is reflective of the typical TAVI population. At least 78% of patients had received a TAVI
At baseline, patients on vitamin K antagonist had higher usage of either single or dual antiplatelet therapy, compared to the DOAC group. 41 Upon adjustment of baseline characteristics, the DOAC group was still associated with significantly reduced all-cause mortality after 19 months of follow-up. Other outcomes were not significantly different. Although this study may provide insights about real-world evidence, it is worth bearing in mind the limitations. There were no reports on INR. There may be inaccuracies with coding and clinical events and all events were self-reported by the centers. Results cannot be extrapolated to other countries and confirmation is needed from larger, prospective randomized trials.
Similar to the OCEAN study, there was a prospective, propensity score-matched, observational study in France from 2010 to 2017 of the TAVI registries and national health claims database to compare DOACs to vitamin K antagonists in post-TAVI patients with a baseline indication for anticoagulation. 42 Of 8962 patients, 24.3% were on DOACs, and the remaining were on vitamin K antagonists. Among patients on DOACs, the majority were on apixaban (52.5%), rivaroxaban (35.4%), and dabigatran (12.1%). The mean age was 83 years. The duration from which patients received a bioprosthetic valve implant to enrollment was not clear. Upon propensity matching, after 3 years, there was a significant reduction in mortality (p < 0.005) and major bleeding including hemorrhagic stroke (p < 0.005) for the DOAC group compared to the vitamin K antagonist group. Similar rates of ischemic stroke and thrombosis were seen. Like the OCEAN study, there were similar limitations, such as no reports on INR, possible coding error, lack of ability to extrapolate to other countries, and residual confounding. Nevertheless, registry studies such as these may shed light on important real-world data on patient outcomes in patients who may have been excluded from controlled clinical trials.
Additional Antithrombotics for Bioprosthetic Heart Valves/TAVI Regardless of Confirmed Concurrent Indication for Anticoagulation
There have been studies evaluating the safety and efficacy of adding antiplatelet(s) regardless of recent stenting, or anticoagulation regardless of another indication such as atrial fibrillation, after a bioprosthetic valve or TAVI. In patients post-TAVI with a baseline indication for anticoagulation, but no recent stent, the effect of adding an additional antiplatelet, namely clopidogrel, was explored in the POPular TAVI trial. 43 In this open-label randomized study, 313 post-TAVI patients with a baseline indication for anticoagulation, primarily atrial fibrillation, were given either the original anticoagulant (vitamin K antagonist or a DOAC) with the addition of clopidogrel, or the original anticoagulant alone, for the first 3 months. Patients were excluded if they had received a drug-eluting stent within 3 months or bare-metal stent within 1 month prior to TAVI. The mean age was 81 years, nearly half of the patients had coronary artery disease, and 10% had a previous episode of myocardial infarction. The actual proportion of patients with a history of coronary stenting was not reported, and patients with a recent stent were excluded. The decision regarding periprocedural anticoagulation was made by the individual attending physicians, and clopidogrel was started either the day before or on the day of TAVI.
Compared to the combined antiplatelet and anticoagulant group, the anticoagulant alone group had a significantly reduced rate of all bleeding [risk ratio (RR) 0.63, 95% CI 0.43-0.90, p = 0.01], and major, life-threatening, or disabling bleeding (RR 0.54, 95% CI 0.29-0.99) after 12 months of follow-up. 43 Similar rates of stroke and mortality were noted. Prespecified subgroup analyses showed possibly lower bleeding rates for DOACs compared to vitamin K antagonist, though the trial was not powered to detect these differences. Data on history of coronary stenting beyond 3 months for a drug-eluting stent and 1 month for bare-metal stent was omitted. However, the guideline consensus is that there appears to be no significant difference in major adverse cardiovascular events after percutaneous coronary intervention between a short duration of dual antiplatelet therapy (eg 1-3 months) and a longer duration (eg 3-6 months, 12 months), in selected patients with lower ischemic risk. 45 If patients undergoing TAVI have a baseline indication for anticoagulation, treatment with anticoagulation alone results in lower risk of bleeding and the addition of clopidogrel is not warranted.
Moreover, the impact of various antithrombotic regimens post-TAVI was explored in a network meta-analysis. 44 The study evaluated single antiplatelet alone, dual antiplatelet therapy, anticoagulant alone, anticoagulant in combination with an antiplatelet, and “triple therapy” which consisted of dual antiplatelet therapy combined with an anticoagulant. There was a total of 13 included studies, predominately observational in nature. Follow-up ranged from 3 months to 45 months, and the mean age of patients ranged from 79 to 84 years. All of the studies used vitamin K antagonist as the anticoagulant, and clopidogrel as the P2Y12 inhibitor. Most of the patients on an anticoagulant had baseline atrial fibrillation, and most on dual antiplatelet therapy had coronary artery disease although completion of coronary stenting is not known. The timing between the operation and initiation of antithrombotics was unclear.
Based on the random effects model, study investigators found that in post-TAVI patients on triple therapy, there was a significant increase in mortality compared to all regimens (p < 0.05). 44 There was an increase in bleeding for triple therapy compared to single antiplatelet therapy (p = 0.033), with no difference in stroke rates across all regimens. Sensitivity analyses showed generally consistent results regarding triple therapy and mortality. No significant heterogeneity or inconsistency was found for the study estimates. Triple therapy should be avoided if possible, and the shortest duration utilized if clinically necessary.
Bioprosthetic Heart Valves/TAVI Without Concurrent Indication for Anticoagulation
The open-label, randomized, GALILEO study enrolled 1644 patients undergoing TAVI and without an indication for any antithrombotic agent at baseline. 46 Patients were randomized to the rivaroxaban group or aspirin group. The rivaroxaban group received rivaroxaban 10 mg daily in combination with aspirin 75-100 mg daily for 3 months and then rivaroxaban monotherapy thereafter. The aspirin group received aspirin 75-100 mg daily in combination with clopidogrel 75 mg daily for 3 months, then aspirin monotherapy thereafter. Therapy was initiated within 1 to 7 days after TAVI, with a median time of 2 days. The mean age was 80 years and 40% of patients had coronary artery disease—albeit none would have qualified for dual antiplatelet therapy based on the exclusion criteria.
After 17 months, the study was terminated prematurely due to safety concerns. There was a significantly higher rate of death or first thromboembolic event, which was the primary efficacy outcome, in the rivaroxaban group compared to the aspirin group (incidence rates 9.8 vs 7.2 per 100 person-years, respectively; HR 1.35, 95% CI 1.01-1.81, p = 0.04). 46 There was also a significantly higher rate of death and non-significantly higher rate of serious bleeding for the rivaroxaban group. On the premise of these findings, patients without a pre-existing indication for anticoagulation post-TAVI should not be initiated on rivaroxaban, including at a lower dose of 10 mg, due to a higher risk of death, thromboembolism, and bleeding.
The previously mentioned ATLANTIS trial also evaluated TAVI patients without an indication for an antithrombotic agent. The second stratum of the trial consisted of patients without an indication for anticoagulation. 34 In this stratum, apixaban was not superior to standard of care, which was either single or dual antiplatelet therapy, at year 1. Bleeding rates were comparable between the groups. Most importantly, there was a non-significantly higher rate of non-cardiovascular death in the apixaban group compared to standard of care (HR 2.99, 95% CI 1.07-8.35). The etiologies of the deaths were attributed to sepsis and end-stage renal failure. While these are not directly associated with anticoagulation, they may be clinically relevant findings that warrant further investigation.
Lastly, the ENAVLE study was an open-label, randomized, noninferiority study of 220 patients undergoing a surgical bioprosthetic valve implantation or repair. 47 Patients were given either edoxaban or warfarin for the first 3 months post-operation. Patients who underwent TAVI were excluded, as well as those with an indication for dual antiplatelet therapy. Patients with and without an indication for anticoagulation were included without stratification, and it was not clear who would have qualified given unreported CHA2DS2-VASc scores. The primary efficacy outcome was the composite of death, clinical thromboembolic events, and asymptomatic intracardiac thrombosis, and the primary safety outcome was major bleeding. Edoxaban was noninferior to warfarin for the primary efficacy outcome (0% vs 3.7% respectively; risk difference, − 0.0367; 95% CI, − 0.0720 to − 0.0014; p < 0.001 for noninferiority), and there was potentially comparable risk for major bleeding. A description of studies in patients without baseline indication for anticoagulation is shown in Table 4.
Summary of Studies for DOACs in Bioprosthetic Heart Valves/TAVI without Concurrent Indication for Anticoagulation.

Abbreviation: direct-acting oral anticoagulant (DOAC), transcatheter aortic valve implantation (TAVI).
Discussion
There is strong evidence for the recommendation that patients with mechanical heart valves should be on lifelong anticoagulation with a vitamin K antagonist, such as warfarin, and the INR goal depends on patient-specific factors as discussed earlier.8–10,48 Though there are small safety studies for rivaroxaban in mechanical heart valves, large high-quality clinical trial data does not exist for DOACs, and therefore cannot be recommended at this time.28–30 Ongoing studies, such as PROACT Xa which explores the use of apixaban in mechanical heart valves, will further delineate the role of DOACs in this setting. 31
In contrast, the management strategy for patients with bioprosthetic heart valves is subdivided into two groups, patients with and without a baseline indication for anticoagulation.8–10 For the former, the original anticoagulant can be resumed after the bioprosthetic valve implantation. Additional antiplatelets should not be used, except in the setting of a recent coronary stent. 32 Ultimately, patients with an indication for anticoagulation should be on it lifelong as monotherapy.
Regarding the choice of anticoagulant, safety data exists for apixaban in patients undergoing TAVI and with a baseline indication for anticoagulation. Rivaroxaban may be used in younger patients who are at least 3 months out from the surgically placed bioprosthetic valve.33,34,38 DOACs as a group may reduce mortality and bleeding compared to vitamin K antagonist although limitations of registry studies should be noted as mentioned prior.41,42 At this time, edoxaban and dabigatran cannot be safely recommended.36,40 Usage of additional antiplatelets and triple antithrombotic therapy should be withheld, even in the case of a recent coronary stent due to higher rates of bleeding and possibly mortality.43,44
In the latter group of patients without a baseline indication for anticoagulation, the goal is to utilize single antiplatelet therapy lifelong, without any additional antithrombotics.8–10 Harm has been shown with rivaroxaban and apixaban in this group of patients undergoing TAVI, and inconclusive evidence exists for edoxaban and dabigatran.34,46,47 In the initial period after TAVI placement during which higher rates of thrombosis exist post-surgery, dual antiplatelet therapy can be used for 3-6 months. In patients with increased risk of bleeding, single antiplatelet therapy may be an alternative option but is not preferred.8–10
Despite guideline recommendations and available data, there has been significant variability in the antithrombotic regimens for patients with atrial fibrillation after a bioprosthetic valve/TAVI. 49 In a study using 2011-2015 registry data in 11,382 patients with atrial fibrillation post-TAVI, patients were prescribed the following at discharge: 7% on a single anticoagulant, 42% on a single antiplatelet, and 51% on antiplatelet(s) and anticoagulation in combination. More specifically and more concerningly, 17.6% of total patients were discharged on triple therapy. Furthermore, another registry study was conducted using data from 2014 to 2017 of 177 915 patients after a surgically placed mechanical or bioprosthetic valve. 50 Of patients discharged on a DOAC (type unspecified), 5% had a bioprosthetic valve and 1% had a mechanical valve. There is an increasing usage of DOACs in mechanical valves, even though there is a direct contraindication (dabigatran) or strong precaution against use (rivaroxaban, apixaban, edoxaban) in this population.
Conclusions
In the face of insufficient high-quality clinical trial evidence, there is significant heterogeneity in the antithrombotic regimen, especially after a bioprosthetic valve. Future large, randomized-controlled trials should assess the long-term safety and efficacy of each DOAC in comparison to vitamin K antagonists in older patients, as reflective of the typical bioprosthetic valve-receiving patient. Trials should assess the effects on long-term clinical outcomes, as well as in the immediate post-operative setting. Ideally, an optimal drug and on-label dosing should be used due to the possibility of harm associated with off-label dosing of DOACs in atrial fibrillation.51,52 It is imperative that concurrent antiplatelet(s) and presence of coronary stenting be taken into account. Additionally, the etiologies of DOAC-induced gastrointestinal bleeding and non-cardiovascular mortality be explored. Until there is the availability of robust randomized clinical trials, providers must remain cautious about DOAC use in both bioprosthetic and mechanical valves, as well as take individual patient characteristics into thoughtful consideration when selecting an antithrombotic strategy.
Footnotes
Ethics Approval and Informed Consent
The authors did not require ethical approval or informed consent for patient information to be published in this article because human subject research was not carried out for this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.