
Abstract
This practical guidance, endorsed by the Brazilian Society of Thrombosis and Hemostasis and The Brazilian Society of Angiology and Vascular Surgery, the International Union of Angiology and the European Venous Forum, aims to provide physicians with clear guidance, based on current best evidence-based data, on clinical strategies to manage antithrombotic strategies in patients with coronavirus disease 2019.
Keywords
Introduction
Coronavirus disease 2019 (COVID-19) predispose patients to arterial and venous thrombotic complications due to its endothelial dysfunction and interplay with intense inflammation, platelet activation, and stasis. 1,2 Also, many patients receiving antithrombotic therapy for venous or arterial thrombotic disease may develop COVID-19 or have its anticoagulation strategy affected by the pandemic crisis. 3 A fair number of guidelines and statement documents were rapidly published and, unfortunately, given the urgent nature of the pandemic, many proposing some never-evaluated anticoagulation/thrombosis management strategies. In this practical guide, we review the current understanding of the pathogenesis, evolving epidemiology and propose an evidence-based management strategy for patients with COVID-19 who develop venous or arterial thrombosis, and of those with preexisting cardiovascular disease who develop COVID-19, or those who need their antithrombotic regimens to be managed during the COVID-19 pandemic. The objective is to keep this guidance very practical, highlighting the knowledge gaps and areas of uncertainty where randomized clinical trials (RCTs) are desperately needed.
What Is Known
Coronavirus disease 2019 now deemed a pandemic by World Health Organization (WHO) It causes severe hypoxemia and severe acute respiratory syndrome Cardiovascular disease = ↑risk of severe COVID-19 Coronavirus disease 2019 with no history cardiovascular disease = ↑risk of severe cardiovascular complications Cardiomyopathy, strokes, severe venous and arterial thrombosis, cardiovascular death High rates of thrombotic events, particularly pulmonary embolism (PE) Sepsis-induced coagulopathy COVID-19 = microvascular thrombosis
What Is Unknown
Coronavirus disease 2019 full mechanism of thrombogenesis Is there any risk score that accurately predicts thrombotic events in patients with COVID-19?” Is there room for a novel anticoagulation strategy other than prophylaxis for patients with COVID-19? When is extended venous thromboembolism (VTE) prophylaxis needed? Is Role of invasive procedures such as fibrinolytic agents and catheter-directed thrombolysis
Venous Thromboembolism With PE or Primary Pulmonary Thrombosis?
Cattaneo and colleagues, involved in the COVID-19 outbreak in Northern Italy reports that 388 patients have been admitted to their wards, and none of them developed symptomatic or asymptomatic deep venous thrombosis (DVT) during their hospital stay. This group performed leg compression ultrasonography, which failed to detect DVT events in all of the 64 tested patients, independently of the severity of their condition and length of in-hospital bed rest. 7 Also, Klok and colleagues from the Netherlands report 184 patients with severe COVID-19, all hospitalized in intensive care unit and treated mostly with standard doses of low-molecular-weight heparins (LMWH) for thromboprophylaxis. They observed a high incidence of VTE (n =28). However, only 1 patient had DVT. 8 It is questioned whether the observed pulmonary vessel occlusions that have been described in reports on patients with COVID-19 are exclusively caused by PE or other thrombotic pathology. Postmortem analysis suggests thrombo-hemorrhagic microangiopathy, enlarged pulmonary blood vessels containing microthrombi, and diffuse thrombotic material is observed also in other organs. 9 Nevertheless, the distinction between both pathologies is not an easy task, because their pathogenesis and, hence, anticoagulant treatment is arguably different. Figure 1 depicts the Coronavirus disease 2019 and thrombotic risk mechanism and Figure 2 shows the high incidence of thrombotic events reported by Klok and colleagues.

Coronavirus disease 2019 and thrombotic risk mechanism. Severe acute respiratory-CoV-2 direct pulmonary and systemic infection, due to its endothelial invasion and dysfunction, activates an inflammatory response, leading to the release of inflammatory mediators. Endothelial and hemostatic activation ensues, with decreased levels of tissue factor pathway inhibitor (TFPI) and increased tissue factor. This viral infection inflammation/coagulation interplay, 4 in association with stasis, cardiovascular diseases, and genetics, leverages the hemostatic derangement 5,6 It results in venous thromboembolism (VTE), particularly pulmonary embolism (PE), arterial thrombosis, myocardial infarction (MI), strokes, and cardiovascular death. In case of further hemostatic derangement; disseminated intravascular coagulation (DIC), whose treatment is different from PE.

Epidemiology. Very high incidence of thrombotic COVID-associated events. The most updated epidemiology data comes from Klok and colleagues, that reevaluated their initial findings and reported a follow-up from 7 to 14 days on 184 intensive care unit (ICU) patients of whom a total of 41 died (22%) and 78 were discharged alive (43%). All patients received pharmacological thromboprophylaxis. The cumulative incidence of the composite outcome, adjusted for competing for risk of death, was 49% (95% CI: 41% to 57%). The majority of thrombotic events were pulmonary embolism (PE; 65/75; 87%). Patients diagnosed with thrombotic complications were at higher risk of all-cause death (hazard ratio [HR]: 5.4; 95% CI: 2.4 to 12). Use of therapeutic anticoagulation was not associated with all-cause death (HR: 0.79, 95% CI: 0.35-1.8). 8
Laboratory Abnormalities COVID-19 10
Lymphopenia ↑ Lactate dehydrogenase ↑ Inflammatory markers C-reactive protein
Ferritin Interleukin-6—(correlates with poor prognosis) ↑Fibrinogen
Coagulation Abnormalities COVID-19 10
Endothelial dysfunction and cytokine storm
Excess thrombin generation and fibrinolysis shutdown Thrombocytopenia or thrombocytosis Prolongation of the prothrombin time, international normalized ratio, and thrombin time ↓Activated partial thromboplastin time SIC: sepsis-induced coagulopathy Thromboelastometry: ↑ MCF FIBTEM
Venous Thromboembolism Prophylaxis for COVID-19
All patients with COVID-19 should undergo risk stratification and all patients with COVID-19 should be considered as high risk (with validated risk-scores such as the Caprini, IMPROVE, and Padua models) and receive inhospital prophylaxis. 11 The Caprini score is currently undergoing validation for patients with COVID-19. Randomized trials have demonstrated the efficacy of prophylactic anticoagulation for reducing the risk of VTE in acutely ill hospitalized medical patients, doses are standard, and appropriate use of VTE prophylaxis has been incorporated into clinical practice guidelines. 12
The choice of agents and dosing should be based on the best evidence-based data available and international guideline recommendations. The WHO interim guidance statement recommends prophylactic daily LMWHs, or twice daily subcutaneous (SC) unfractionated heparin (UFH). 13 No increased dose of anticoagulants for VTE prophylaxis in medically ill patients was validated on properly conducted RCTs. We, therefore, recommend against until ongoing trials provide reliable evidence of the efficacy safety profile of these strategies. In case pharmacological prophylaxis is contraindicated, mechanical VTE prophylaxis (intermittent pneumatic compression) should be considered in immobilized patients. 12
Extended VTE prophylaxis should be considered after hospital discharge. Previous RCTs in patients hospitalized with acute medical illness demonstrated that extended prophylaxis with enoxaparin 14 or direct oral anticoagulants (DOACs) can reduce the risk of VTE, at the cost of an increase in bleeding events, including major bleeding. 15 –17 While no data specific to COVID-19 exist, there are planned RCT for this particular high-risk population. Interestingly, clinicians have observed that patients with COVID-19 frequently fail to fall into Mariner trial criteria. For now, it is reasonable to apply a case-by-case risk stratification for thrombotic and hemorrhagic risk, followed by consideration of extended prophylaxis (for up to 45 days) for patients with an elevated risk of VTE and low risk of bleeding. 18
Venous Thromboembolism Prophylaxis Recommendations
Risk stratification and in-hospital prophylaxis (all)—IMPROVE, Caprini, Padua
The WHO Interim Guidance Statement Recommends Standard Doses
Enoxaparin 40 mg SC once daily* Fondaparinux 2.5 mg once daily Unfractionated heparin 5.000 IU SC twice daily Consider extended VTE prophylaxis with either LMWH or DOAC (up to 45 days post-discharge). Extended prophylaxis with LMWH or DOACs = ↓risk of VTE but ↑major bleeding If anticoagulants contraindicated = mechanical prophylaxis
* Enoxaparin dose adjustment: CrCl < 30 mL/minute = enoxaparin 20 mg SC once daily (↓50% of the dose)
* Enoxaparin dose adjustment for body mass index (BMI): 40 to 60 mg once daily for BMI 30 to 40 kg/m2
40 mg twice a day for BMI > 40 kg/m2
60 mg twice a day for BMI > 50 kg/m2. Figure 3 and 4 show the dose/regimen for anticoagulants for VTE prophylaxis for patients with COVID-19.
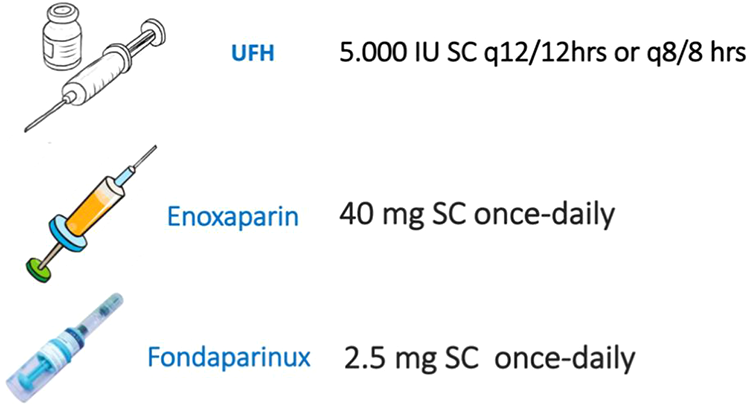
Heparins–in hospital prophylaxis doses of anticoagulants for coronavirus disease 2019 (COVID-19) patients. 19

Extended venous thromboembolism (VTE) prophylaxis strategy doses.
Coronavirus Disease 2019 and VTE Treatment
The mainstay treatment for VTE is anticoagulation. 20 Standard doses should be used until further data emerge from ongoing RCT. As of now, we have minimal available data to indicate lower mortality from routine use of advanced VTE therapies such as fibrinolytic therapies or vena cava filters insertions. 21 Duration of anticoagulation should be defined in a case-by-case scenario but given the severity of COVID-associated thrombotic events in combination with clinical comorbidities, it is reasonable to think on prolonged anticoagulation therapies. 22
Treatment
Full anticoagulation (mainly LMWH*, fondaparinux, or UFH while at hospital and DOACs for long-term treatment) at standard doses Minimal available data to indicate lower mortality from routine use of advanced VTE therapies ↓ The use of inferior vena cava filters and catheter-directed thrombolysis (CDC) Home treatment whenever possible Treat suspicious of PE as PE Pulmonary embolism management should follow international guidelines Submassive but stable = anticoagulation Massive (unstable PE) = fibrinolysis
No evidence to increase doses off-label
Dose adjustments with renal function*
* Enoxaparin treatment dose adjustment = CrCl < 30 mL/minute = 1 mg/kg SC once daily (↓50% of the dose). Figure 5 and 6 show the dose/regimen for anticoagulants for VTE treatment for patients with COVID-19.

Heparins–VTE treatment doses. Inhospital full anticoagulation doses of parenteral drugs for coronavirus disease 2019 (COVID-19) patients. 19

Direct oral anticoagulants anticoagulation doses for coronavirus disease 2019 (COVID-19) patients. 23
Pandemic Empirical Therapeutic Anticoagulation
Coronavirus disease 2019 is a new aggressive viral infection with scarce reliable data on its cardiovascular morbidity and mortality. Reports suggest unexpected high rates of severe thrombotic arterial and venous events. 8 Given the nature of some desperate situations, some clinicians have suggested intermediate-dose or full dose parenteral anticoagulation (rather than prophylactic dosing) for routine care of patients with COVID-19, hypothesizing that it may confer a benefit in preventing microvascular thrombosis, even in the absence of suspicious of thrombosis. 21 The existing data are very limited, primarily based on a subgroup analysis (N = 97) from a single retrospective study with limited adjustments. 24 As of now, it is not possible to evaluate the safety/efficacy profile of such unusual strategies. Proper RCTs are ongoing and will provide important guidance regarding the best anticoagulant strategies for COVID-19 thrombosis management.
Ongoing COVID-19 Anticoagulation Strategies Clinical Trials
There are currently 40 programmed studies and RCTs evaluating different anticoagulation strategies for COVID-19 thrombosis-related management registered at www.clinicaltrials.gov. Table 1 depicts these studies/trials registered up to April 30, 2020.
Ongoing Interventional Trials on VTE Management in Patients With COVID-19.

Abbreviations: COVID-19, coronavirus disease 2019; DIC, disseminated intravascular coagulation; ICU, intensive care unit; VTE, venous thromboembolism.
Final Considerations
Given the coronavirus pandemic, with its unexpected high rates of arterial and venous thrombotic events, it is understandable that clinicians on the frontline decide to stretch the boundaries of known treatment indications. So far, in the Covid-19 pandemic, we have observed that treatment has often been offered based on individual clinician’s opinion. It is not known when this pandemic will end and the scientific community in different parts of the world has been working hard to generate the appropriate evidence that is needed to guide clinical practice decisions and improve patient care. Pandemic distress does not grant freedom to choose whatever anticoagulation strategies physicians feel to be appropriate based solely on personal experiences. Clinical observations and common sense coupled with the appropriate equipoise across different interventions should be used to generate hypotheses to be tested prospectively in well-powered RCTs).
Randomized clinical trials are the most reliable approaches to evaluating the effects of new treatments and vaccines. 25 During the 2014 to 2015 West African Ebola epidemic, many questioned if such trials would be feasible. Experienced colleagues demonstrated that RCT, even in such difficult circumstances, was not only feasible but the only reliable way that could provide proper guidance, in contrast to the empirical strategies employed during pandemic times. 26
Many different trials evaluating anticoagulants and other strategies for both VTE prophylaxis and treatment are currently ongoing. Reliable data will be available soon, but until then, physicians should do what has been proven to be efficient and safe and in case of uncertainty randomize patients into ongoing clinical trials.
Footnotes
Authors’ Note
Endorsed by the Brazilian Society of Thrombosis and Hemostasis, The Brazilian Society for Angiology and Vascular Surgery, the International Union of Angiology and the European Venous Forum.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.