
Abstract
Background:
Atrial fibrillation (AF) is the most common cardiac arrhythmia and is frequently present in patients with mitral regurgitation (MR). Currently, there is a lack of real-world evidence specifically addressing the clinical performance of direct oral anticoagulants (DOACs) in patients with AF and concomitant MR. Therefore, the aim of the present study was to assess the efficacy and safety profile of DOACs therapy in patients with AF and MR.
Methods:
Data for this study were sourced from the Atrial Fibrillation Research Database in the Department of Cardiology at Monaldi Hospital. The database was queried for AF patients with MR who were prescribed DOACs therapy. The primary safety outcome was defined as the annual incidence rate of major bleeding events and the primary effectiveness outcome as the annual incidence rate of all events classified as ischemic stroke, transient ischemic attacks, and systemic embolisms.
Results:
Consecutive AF patients with concomitant mild to severe MR who received DOACs therapy (n = 259) were included. Patients were dichotomized in 2 groups according to MR severity: a mild-to-moderate group (MR 1-2+; n = 151) and a moderate-to-severe group (MR 3-4+; n = 108). The incidence rate of major bleedings was significantly higher in MR 3-4+ group (3.92%) compared with the MR 1-2+ group (1.18%; hazard ratio [HR]: 3.2; 95% CI: 1.4-7.3; P = .0059). The incidence rate of thromboembolic events between MR 3-4+ group (0.66%) and MR 1-2+ group (0.62%) was not significantly different (HR: 0.75; P = .823).
Conclusions:
In the present study, there was no difference in the efficacy profile of DOACs between AF patients with mild-to-moderate and moderate-to-severe MR. Considering the increased bleeding risk, a close and careful follow-up should be warranted for patients with moderate-to-severe MR.
Introduction
Atrial fibrillation (AF) is the most common arrhythmia in general population and is frequently associated with significant valvular heart disease (VHD). 1,2 Mitral regurgitation (MR) is the most frequent VHD worldwide 3 and during its natural course AF onset is associated with increased cardiac mortality. 4 Direct oral anticoagulants (DOACs) are considered a first-line anticoagulant treatments in patients with “non-mechanical and rheumatic mitral” (non-MARM) valvular AF. 5 Despite evidence from randomized trials suggest DOACs are a valid therapeutic strategy in AF patients with VHD, 6 currently, the real-world clinical performance of DOACs in the exclusive setting of MR remains largely unexplored. The aim of our study was to evaluate the safety and efficacy of DOACs therapy in AF patients with mild-to-severe MR, thus providing novel insights in this clinical context.
Materials and Methods
Database
Data for this study were sourced from the prospectively maintained Atrial Fibrillation Research Database (NCT03760874), in the Department of Cardiology at Monaldi Hospital which includes all patients with AF (paroxysmal, persistent, and permanent), followed at our institution between March 2013 and July 2018. Follow-up data were obtained through outpatient visits each 3 to 6 months. During the follow-up visits, the clinical status, occurrence of stroke, transient ischemic attack (TIA), systemic embolism (SE), major bleeding (MB), intracranial hemorrhage (ICH), minor bleedings, or other side effects were assessed. All included patients received baseline and follow-up echocardiographic examination. The study was approved by the local institutional review committee. Ischemic stroke was defined as a focal neurologic deficit lasting for at least 24 hours with no signs of hemorrhage on cerebral imaging and was verified radiologically. Transient ischemic attack was defined as an acute focal neurologic deficit lasting less than 24 hours. Systemic embolism was defined as an acute vascular insufficiency associated with clinical or radiographic evidence of arterial occlusion and not associated with another likely cause.
Major bleeding was defined as fatal bleeding or symptomatic bleeding in a critical area or organ or bleeding causing a fall in hemoglobin level of ≥2 g/dL or more or leading to transfusion of 2 or more units of whole blood or red cells. 7 Minor bleed was defined as overt bleeding not meeting the criteria for MB but requiring medical intervention, unscheduled contact (visit or telephone) with a physician, temporary interruption of the use of a study drug (ie, delayed dosing), pain, or impairment of daily activities.
Patients Population
The database was queried for AF patients with MR who were prescribed DOACs therapy. The MR severity was assessed at baseline evaluation and during follow-up visits through a multiparametric approach, principally based on semi-quantitative method (vena contracta measurement), according to recent guidelines. 8 We identified 562 patients with AF and MR who received DOACs therapy. Atrial fibrillation patients with bioprosthetic valve (n = 30), prior cardiac surgery (n = 77), concomitant more than mild aortic valve disease (n = 73), prescription of antiplatelet (n = 50), or dose-reduced DOACs therapy (n = 30) and patients who had follow-up less than 360-days after the first qualifying anticoagulant prescription (n = 43) were excluded from the analysis.
Finally, 259 patients with AF and MR treated with DOACs were dichotomized in 2 groups according to MR severity: a mild-to moderate group (MR 1-2+; n = 151) and a moderate-to severe group (MR 3-4+; n = 108). Mean follow-up time was 434 days (interquartile range: 387-519) and 560 days (interquartile range 446-689) for MR 1-2+ and MR 3-4+ group, respectively.
End Points
The primary safety outcome was the incidence rate of MB. The primary effectiveness outcome was incidence rate of all events classified as ischemic stroke, TIA, and SE.
Statistical Analysis
The distribution of data was assessed by using both the Kolmorov–Smirnov and the Shapiro–Wilk test. Descriptive statistics of patient characteristics were carried out; continuous variables were expressed as mean ± SD or median with interquartile range, and percentage were reported for the categorical variables The incidence of bleeding was calculated both as incidence rate (the ratio between the number of new events occurred during the follow-up and the person-time accrued from the study members) every 100 patient-years and as cumulative incidence. Proportional hazard models applied to the incident rate function were employed to define the primary safety and effectiveness end points. Continuous variables were compared using t tests, and categorical variables were compared using χ2 tests. Cox regression analysis was performed to evaluate the effects of baseline different variables between MR 1-2+ and MR 3-4+ group on survival free from occurrence of safety and effectiveness end point. A Kaplan–Meier analysis and log-rank test were used to compare the event rates of predetermined end points over time. A 2-sided P value less than .05 was considered significant for all tests. All statistical analyses were performed using Rstudio (RStudio Team .2016 RStudio: Integrated Development for R. RStudio, Inc.; http://www.rstudio.com/.).
Results
Study Population
Baseline demographic and clinical features of the groups are shown in Table 1. The only statistically significant different features between MR 3-4+ group (age 73.04 ± 11.85 years, males: n = 47; 43.51%) versus MR 1-2+ group (age 72.03 ± 12.59 years, males: n = 82, 54.3%) were a more impaired renal function (25% vs 15.23%; P = .04), a higher prevalence of dilated cardiomyopathy (12.03% vs 4.64%; P = .02) and heart failure (44.44% vs 29.8%; P = .01), persistent (21.3% vs 26.49%; P = .02) or permanent (52.77% vs 45.03%; P < .01) AF, and rate of implanted cardiac devices (40.74% vs 27.15%; P = .02). There were no significant differences of DOACs prescription, CHA2DS2-VASc, and HASBLED score between the groups. During the follow-up period, there was no crossover from DOACs to vitamin K antagonists therapy in the study population. Moreover, the degree of kidney failure and of MR did not significantly change during the time course of the study.
Baseline Demographic and Clinical Characteristics of Study Population.a

Abbreviations: AF, atrial fibrillation; CHA2DS2, Congestive heart failure, Hypertension, Age (>65 = 1 point, >75 = 2 points), Diabetes, previous Stroke/transient ischemic attack (2 points); COPD, chronic obstructive pulmonary disease; DOAC, direct oral anticoagulant; HAS-BLED,
a Values are mean ± SD unless otherwise stated.
Bold values are statistically significant.
Safety and Effectiveness Outcome
A total of 23 patients (16 in MR 3-4+ group and 7 in MR 1-2+ group) experienced MB. The cumulative incidence over 3-years of MB was 14.8% (16/108) in MR 3-4+ group and 4.6% (7/151) in MR 1-2+ group (P = .003). The incidence rate of MB was 3.92% per 100 person-years in MR 3-4+ versus 1.18% in MR 1-2+ group (hazard ratio [HR]: 3.2; 95% CI: 1.4-7.3; P = .0059). Figure 1 shows the Kaplan–Meier cumulative probability of major bleeding event-free survival of MR 3-4+ and MR 1-2+ groups (log-rank 7.5870; P = .0059). At univariate Cox regression analysis, MR 3-4+ (HR: 0.30; 95% CI: 0.12-0.74; P < .01), evidence of heart failure (HR: 0.28; 95% CI: 0.11-0.69; P < .01), and baseline left ventricle ejection fraction (HR: 0.95; 95% CI: 0.92-0.98; P < .01) were predictors of major bleedings. By multivariate Cox regression model, none of these variables was significantly associated with safety outcome, and MR 3-4+ did not predict major bleedings (HR: 0.53; 95% CI: 0.04-6.16; P = .61).

Kaplan–Meier cumulative probability of major bleeding event-free survival in MR 1-2+ and MR 3-4+ group.
Five patients (2 in MR 3-4+ group, 3 in MR 1-2+ group) experienced the effectiveness end point during the follow-up period. The cumulative incidence over 3 years of thromboembolic events in the MR 1-2+ and MR 3-4+ groups was 1.9% (3/151) and 1.8% (2/108), respectively (P = .75). The incidence rate of thromboembolic events was 0.66% per 100 person-years in MR 3-4+ versus 0.62% in MR 1-2+ group (HR: 0.75; 95% CI: 0.13-4.3; P = .823). Figure 2 shows the Kaplan–Meier cumulative probability of thrombotic event-free survival in MR 1-2+ and MR 3-4+ groups (log rank 0.1062; P = .7446).
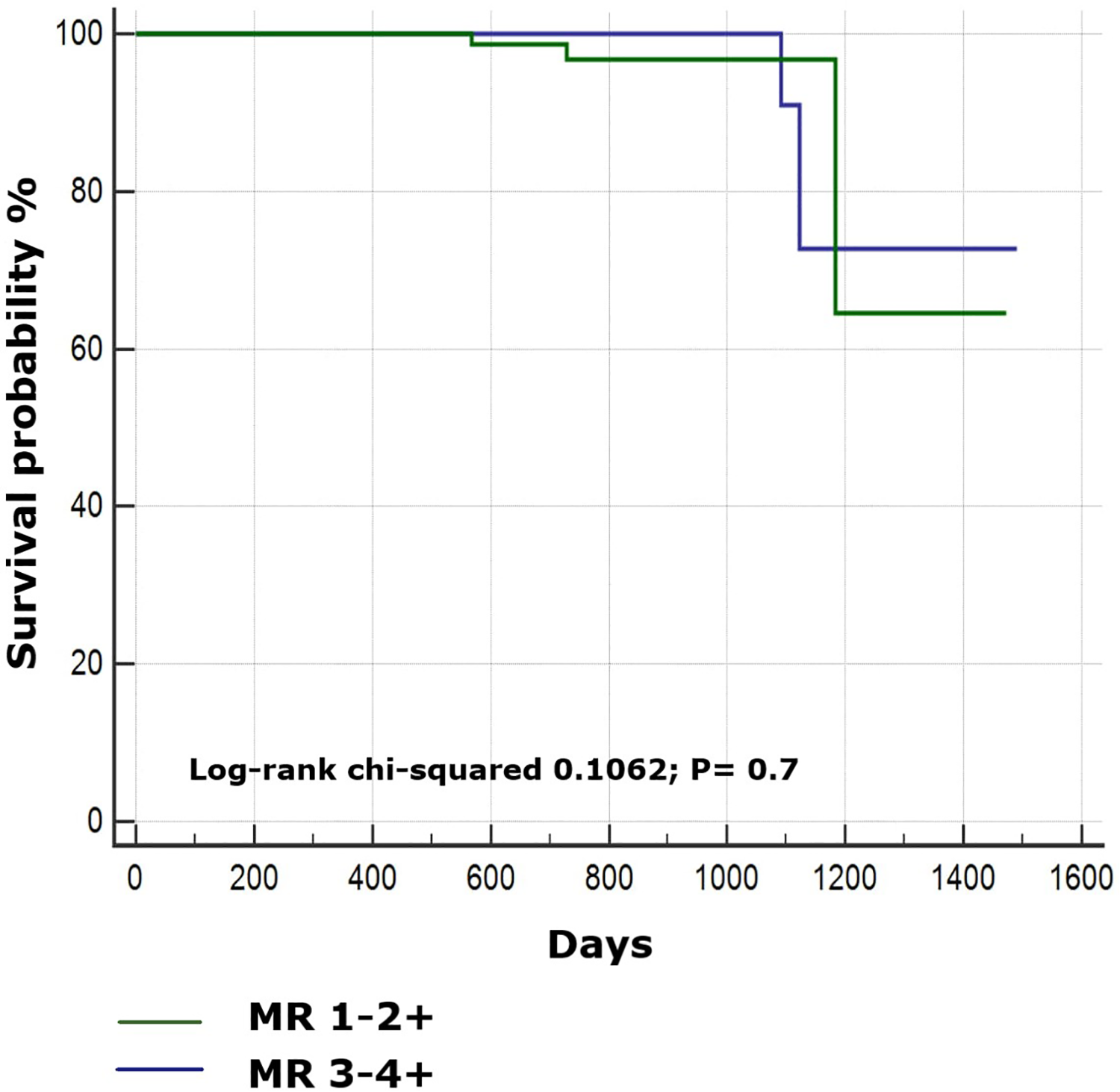
Kaplan–Meier cumulative probability of thromboembolic event-free survival in MR 1-2+ and MR 3-4+ group.
Discussion
The current definition of “valvular AF” refers to patients with AF related to hemodynamically significant mitral stenosis or prosthetic mechanical heart valves (1) and landmark randomized clinical trials (RCTs) on DOACs have excluded these patients, considering them at particularly high risk of thromboembolic events. 9 Considering the heterogeneity of the “non-valvular” definition and the variable inclusion criteria of the 4 pivotal trials on DOACs, the terms “non-MARM valvular AF” and Evaluated Heartvalves, Rheumatic or Artificial (EHRA) type 2 VHD have also been proposed to clearly identify AF patients with valvular disease who could benefit from DOACs therapy. 5,10 Despite growing real-world evidence suggesting a favorable clinical profile in patients with bioprosthetic heart valves, 11,12 the real-world benefit of DOACs in patients with non-MARM valvular AF or EHRA type 2 VHD remains an important unfocused clinical issue not definitively addressed.
Four main RCTs have included a variable proportion of AF patients with VHD, 13 -16 with MR being the most represented (>70%) valvular disease subtype. 16 Even though post hoc analysis and meta-analysis of the 4 pivotal RCT have shown an overall favorable clinical profile of DOACs therapy versus vitamin K antagonists in AF patients with VHD, 13 -17 neither subanalysis of RCT nor real-world studies evaluated the performance of DOACs in the exclusive setting of AF and MR.
The present retrospective observational cohort study specifically addressed the real-world clinical performance of DOACs therapy in patients with AF and concomitant MR, according to a different degree of MR. We observed no significant differences in the annual rates of thromboembolic events between AF patients with mild-moderate MR and moderate-severe MR treated with DOACs. Our observed incident rate is slightly lower than that reported in a recently published nationwide cohort study, which, however, assessed the thromboembolic events in a subgroup of incident AF patients with combined mitral and aortic regurgitation. 18 The overall low rates of observed thromboembolic events among our population could be explained by the protective effect of significant MR on stroke events. 19 In chronic MR, the left atrium is exposed to significant volume overload progressively leading to chamber dilatation and remodeling, which represents the physiopathological substrate for AF onset and maintenance. 20 Several studies have reported a reduced incidence of left atrium appendage spontaneous echo contrast and thrombosis in patients with AF and non-rheumatic MR 21,22 and the most reasonable mechanism is the protective “washing” effect of the turbulent MR flow, which increases endoluminal shear stress in the left atrium, thereby preventing thrombus formation. A previous study by Fukuda and colleagues showed that mild MR was associated with a 2.7-fold increased risk of stroke/thromboembolism, while severe forms may possibly have a “protective” effect. 23 Moreover, a large, retrospective, single-center analysis conducted in a large cohort of patients with non-valvular AF showed that neither MR nor its severity was associated with a higher risk of stroke or SE. 24 Conversely, in a recent large real-life cohort study, AF patients with concomitant MR had a similar thromboembolic risk compared to AF patients without MR, also after adjustment for oral anticoagulant therapy, and severe MR was associated with a similar risk for thromboembolic events compared to other AF patients. 25 Unfortunately only vitamin K antagonists recipients are reported in this study, 25 and globally, few data are available on the potential effects of DOACs therapy on the thromboembolic risk of AF patients with different MR severity. Therefore, in light of these controversial evidence, our preliminary finding may suggest an increased efficacy of DOACs in severe MR compared to mild MR group. However, considering the study design and the impossibility to adjust for baseline different MR severity in our population, we have not enough data to definitively support this preliminary finding that needs further corroboration in specifically designed trial with a more controlled study population.
Even though moderate-to-severe MR was not independently associated with safety outcome, in our study population, the annual rate of major bleeding events was significantly higher in patients in MR 3-4+ group compared to MR 1-2+ group (3.92% vs 1.18% respectively; P = .0059). Currently, there are few evidence investigating the relationship between the degrees of MR and bleeding risk. Blackshear et al reported an acquired reduction of von Willebrand factor in patients with moderate-to-severe MR, which is probably related to the high shear stress induced by the regurgitant flow and may consequently play a pro-bleeding effect. 26 A possible explanation could be the clinical features of MR 3-4+ groups, which showed a higher incidence of clinical heart failure and more impaired left ventricle systolic function, configuring an overall higher risk profile subgroup. However, we are not able to elucidate whether the higher bleeding risk profile of moderate-to-severe MR patients is related to heart valve disease itself, to DOACs therapy or to the presence of not considered risk factors. Therefore, our results may be hypothesis-generating and require further validation.
Limitations
The present was a retrospective observational, non-randomized study, which provided insights on the clinical performance of DOACs, without direct comparison with vitamin K antagonists and conducted on a relatively small population of AF patients with mild to severe MR with a relatively short follow-up. The inclusion of AF patients without MR as a matched control group could have been more informative. The small number of observed thromboembolic events may have reduced statistical power to detect heterogeneity in the efficacy of DOACs therapy among 2 MR groups. Besides, there may be residual confounding factors influencing both thromboembolic and bleeding risk between groups that could not be accounted for despite adjustments. Indeed, we did not include the frequency of tricuspid regurgitation in our population, but it should not be considered a significant limitation of the study, considering that also ROCKET-AF and ENGAGE-AF-TIMI 48 trial did not report the frequency of tricuspid regurgitation and that this variable has not been associated with a different clinical outcome in randomized trials of DOACs. Furthermore, MR quantification was performed following European recommendations, 7 based on a single-operator assessment and principally relying on vena contracta measurement; a multiparametric evaluation, including EROA and Rvol, may have allowed a more comprehensive assessment.
Conclusions
Currently, there is a lack of real-world data exploring the clinical performance of DOACs in the exclusive setting of AF patients and concomitant MR. The results of the present study show that there was no difference in the efficacy profile of DOACs among AF patients with mild-to-moderate and moderate-to-severe MR. However, we report a not negligible bleeding risk in patients with moderate-severe MR, which suggest a more careful follow-up in this subgroup of patients. Further extended evidence are necessary to confirm our preliminary results.
Footnotes
Author Contributions
Enrico Melillo contributed to the literature review and critical interpretation, and design and drafting of the manuscript; Anna Rago, Emilio Attena, and Maddalena Carrella contributed to the conception and design of the manuscript and data collection; Riccardo Proietti helped in data interpretation and analysis; Paolo Golino, Antonio D’Onofrio, and Gerardo Nigro contributed to the critical revision and analysis of the manuscript and gave final approval; and Vincenzo Russo contributed to the design, analysis, and interpretation; critical revision of the manuscript; and gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.