
Abstract
Background
Associations of neutrophil-to-lymphocyte ratio (NLR) and its longitudinal change with risk of fatal strokes are unclear in older populations.
Methods
In this retrospective analysis, a total of 27,799 participants were included and followed up for a mean of 14.3 years (standard deviation = 3.2). 838 stroke deaths were recorded. Cox proportional hazards regression was used to assess associations of NLR with fatal strokes.
Results
Compared to those in the first quartile and after adjustment for a series of factors, the participants in the highest neutrophil quartile had an increased risk of fatal all stroke (adjusted hazard ratio (aHR) = 1.45, 95% confidence interval (CI), 1.18–1.79) and fatal ischaemic stroke (aHR = 1.58, 95% CI, 1.17–2.12). Restricted cubic splines showed an increased trend of relationship between the NLR and fatal all stroke. The participants with the highest NLR quartile had an increased risk of fatal all stroke (aHR = 1.52, 95% CI, 1.23–1.88) and fatal ischaemic stroke (aHR = 1.59, 95% CI, 1.13–2.26), respectively; Similar associations repeated after further C-reactive protein adjustment; a 21% and a 32% increased risk of fatal all stroke and fatal ischaemic stroke showed in a continuous variable model. Those in NLR change with 5% increase had a 70% increased risk of fatal all stroke (aHR = 1.70, 95%CI, 1.13–2.57), compared to those in stable (−5%∼5%).
Conclusions
Higher NLR was associated with an increased risk of fatal all stroke and fatal ischaemic stroke, and its longitudinal change increase of ≥ 5% was associated with an increased risk of fatal all stroke in a relatively healthy older population.
Summary box
What is already known on this subject?
White blood cell and neutrophil counts are commonly inflammatory markers; they have been related to the risk of stroke events.
What this study adds?
The neutrophil-to-lymphocyte ratio and its longitudinal increased change were associated with the risk of fatal stroke occurrence in relatively healthy older populations.
How this study might affect research, practice or policy?
A continuous chronic inflammation increases the risk of fatal stroke occurrence. The clinicians should pay more attention to asymptomatic inflammatory characteristics in relatively healthy older populations.
Introduction
Stroke has become the second and the leading cause of deaths worldwide, 2015 1 and in China, 2013. 2 It is classified mainly as ischaemic and haemorrhagic stroke. Hypertension, diabetes, and smoking have been known as the shared risk factors of stroke incidence, and related closely to a chronic inflammation.3–6 Chronic inflammatory diseases were associated with an increased risk of stroke,7–9 suggesting that inflammation runs through the pathophysiological progress in stroke.
The neutrophil-to-lymphocyte ratio (NLR) has been widely used to predict various causes of death such as cancer, 10 coronary heart disease (CHD) 11 and all-cause death.12,13 Current studies addressing the relationship between the NLR and the risk of fatal stroke focused mainly on stroke onset, and corresponding results are inconsistent because of no long period enough for conducting follow-up.14–16 Such data and information were based on acute inpatients, and all of tests were conducted after stroke happened. Thus, the corresponding results should reflect a status under stress reaction; the NLR should be more likely to direct an acute inflammation. Such clinical studies revealed that the NLR could be used as a predictor for future mortality risk of CHD, 11 30-day mortality and morbidity 17 and neurological deterioration (ND) 18 after intra-cerebral hemorrhage (ICH), symptomatic hemorrhagic transformation (sHT) in acute ischemic stroke, 19 and poststroke cognitive impairment (PSCI). 20 Additionally, higher total white blood cell and neutrophil counts were related to an increased risk of fatal stroke occurrence in a relative healthy older population, 21 although it is unclear whether the NLR, especially its longitudinal change, is associated with the risk of fatal stroke occurrence. Here, we aimed to systematically assess the relationship between the NLR, its longitudinal change and future risk of fatal all stroke, fatal ischaemic or haemorrhagic stroke occurrences in a relatively healthy older population.
Methods
Study Design, Data Source and Participants
This is a retrospective analysis of fatal stroke occurrences in the Guangzhou Biobank Cohort Study (GBCS) from September 30th, 2003 to April 13th, 2021. All GBCS participants were recruited from a population of permanent residents aged 50 years or older in Guangzhou in southern China. Details of the GBCS have been reported previously. 22 The baseline (from September 30th, 2003 to February 28th, 2008) and follow-up information included a face-to-face computer-assisted interview by trained nurses on lifestyle, the family and personal medical history; assessments of anthropometric data and blood pressure; and a series of laboratory tests. Each participant had made an appointment in advance to ensure good health, was able to go to the designated place, and had to sit and rest for at least half an hour before sampling and examination.
Exposure Indicators
The blood cell counts were performed with a counter (KX-21, Sysmex, Japan) in Guangzhou Twelfth People's Hospital. The neutrophil (NEUT) and the lymphocyte (LYM) counts were determined automatically. The NLR was calculated accordingly from the NEUT and the LYM counts. Fasting glucose, cholesterol, triglycerides, liver and kidney function and high-sensitivity C-reactive protein (hs-CRP) were measured with an analyzer (Cobas c-311, Roche, Switzerland). The hospital laboratory performs internal and external quality control procedures according to the China Association of Laboratory Quality Control.
Study Outcomes and Potential Confounders
Information on underlying causes of death up to April 13th, 2021, was obtained mostly via record linkage with Guangzhou Centers for Disease Control and Prevention (GZCDC). Because there was no other information for stroke severity, infarct volume, site of lesion and infectious complications, fatal stroke occurrence was chosen as the primary outcome of this study. Death causes were coded according to the 10th revision of the International Classification of Diseases (ICD) as follows: I60–I69 for stroke; I60.0–I62.9 and I69.0–I69.2 for haemorrhagic stroke; I63.0–I63.9 and I69.3 for ischaemic stroke; and the other codes for unclassified stroke. When the death certificates were not issued by medical institutions, the causes were verified by the GZCDC as part of their quality assurance programmed by cross-checking past medical history and conducting verbal autopsy by 5 senior clinicians from Guangzhou Twelfth People's Hospital, the Universities of Hong Kong, China and Birmingham, UK. To examine the extent to which baseline factors in relation to the risks of stroke, ischaemic and haemorrhagic stroke, we included the factors in different models. Model 1 was a crude hazard ratio model without adjustment for any confounders. Model 2 contained a multivariate adjustment for factors including sex, age, smoking (never, former and current), alcohol consumption (never, former and current), International Physical Activity Questionnaire-assessed physical activity (inactive, moderate and active), 23 body mass index (BMI, defined as weight in kg÷height in m2), self-rated health, hypertension, diabetes, dyslipidaemia, cancer, Genitourinary disease (GD), chest disease and the platelet count. Model 3 included hs-CRP as a competing confounder in addition to the confounders in model 2.
Statistical Analysis
The NEUTs, the LYMs and the NLRs were classified by quartiles, respectively: the first quartile (<3.0*10^9/L), the second quartile (3.0–3.6*10^9/L), the third quartile (3.7–4.4*10^9/L) and the fourth quartile (>4.5*10^9/L) for the NEUTs; the first quartile (<1.8*10^9/L),the second quartile (1.8–2.1*10^9/L), the third quartile (2.2–2.5*10^9/L) and the fourth quartile (>2.5*10^9/L) for the LYM; the first quartile (≤1.39), the second quartile (1.40–1.75), the third quartile (1.76–2.23) and the fourth quartile (≥ 2.24) for the NLR; and the NLR was then analyzed as a continuous parameter using a restricted cubic splines curve model (RCS), and as a dichotomous variable and continuous variable respectively: 3 knots at the 10th, the 50th, and the 90th percentiles for the RCS; ≤1.75 versus > 1.75 for a dichotomous variable. For longitudinal NLR changes, we chose one follow up closest to baseline, thus only those who participated in the first follow-up (from March 2008 to December 2012) were included, and the follow-up period started from baseline (September 2003 to February 2008); an exposure period was therefore followed by the beginning of baseline. The group (±5%) was formed, from those with two exposures and those who survived. Continuous variables are presented as the mean ± standard deviation, and categorical variables were described by frequency and percentage. The chi-squared and Fisher's exact test were used for categorical variables, and analysis of variance (ANOVA) and the Kruskal-Wallis test were used for continuous variables. Based on the results of the crude hazard ratio model analysis, a sensitivity analysis was conducted in which model 2 and model 3 were repeated for the participants without CVD at baseline and further adjustment for hs-CRP. All analyses were performed using STATA (Version 14.0; StataCorp LP, College Station, TX, USA). All p values were 2 sided, and statistical significance was defined as p < 0.05; p values for trends in the models were calculated as ordinal scores from the second, the third and the fourth quartiles when taking the first quartile as the reference.
Results
Baseline Characteristics
In total, 30,430 participants were screened. Among the data exclusions, there were 286 because of a previous history of stroke, 315 because of an unclear stroke history, 372 because of loss to follow-up with unknown vital status, 1658 because of incomplete information on the NEUT, the LYM and platelet counts, hypertension, diabetes, dyslipidaemia, smoking, alcohol consumption, physical activity, BMI, self-rated health, cancer, GD or chest disease. A total of 27,799 participants who were free of stroke at baseline were included in this study. After a mean follow-up time of 14.3 (standard deviation = 3.2) years with 320,859 person-years, 838 stroke deaths (413 ischaemic, 264 haemorrhagic and 161 unclassified) were recorded (Figure 1).

Flow diagram of participants selected for the analysis of this study.
The baseline characteristics of the participants are presented in Table 1. Compared to the population in the first NLR quartile, the populations in the highest NLR included more men, were older, had more hypertensive, current smoking and drinker, diabetes; had less physical activity, dyslipidaemia, GD and had poorer self-rated health.
Baseline characteristics by the NLR quartiles of participants in the GBCS (n = 27,799).
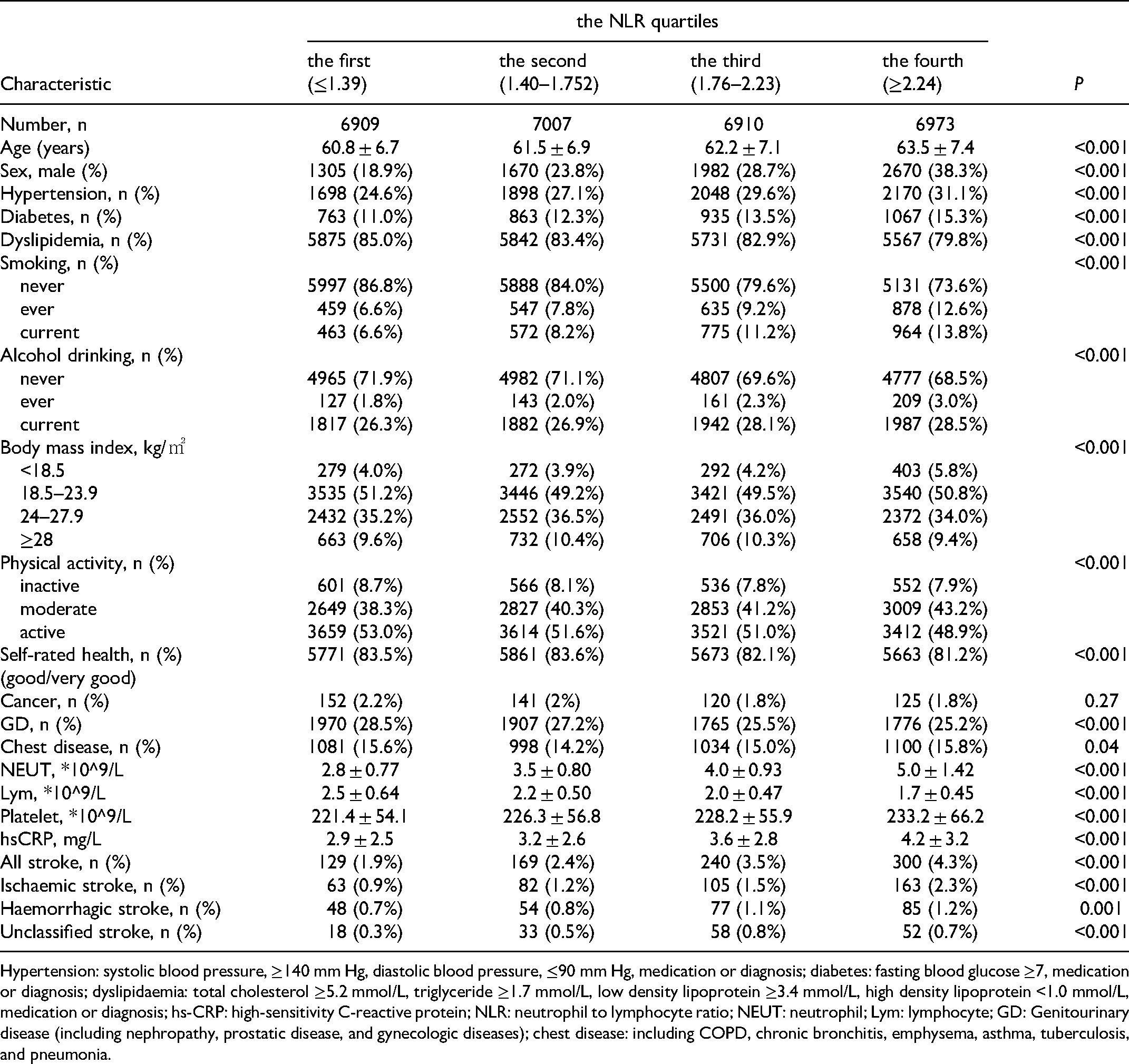
Hypertension: systolic blood pressure, ≥140 mm Hg, diastolic blood pressure, ≤90 mm Hg, medication or diagnosis; diabetes: fasting blood glucose ≥7, medication or diagnosis; dyslipidaemia: total cholesterol ≥5.2 mmol/L, triglyceride ≥1.7 mmol/L, low density lipoprotein ≥3.4 mmol/L, high density lipoprotein <1.0 mmol/L, medication or diagnosis; hs-CRP: high-sensitivity C-reactive protein; NLR: neutrophil to lymphocyte ratio; NEUT: neutrophil; Lym: lymphocyte; GD: Genitourinary disease (including nephropathy, prostatic disease, and gynecologic diseases); chest disease: including COPD, chronic bronchitis, emphysema, asthma, tuberculosis, and pneumonia.
The NEUT and the LYM in Relation to the Risk of Fatal Stroke Occurrence
Prior to the NLR analysis, we observed that those in the highest NEUT quartile had a significant association with an increased risk for fatal all stroke (adjusted HR (aHR) = 1.45, 95% CI 1.18–1.79, P < 0.001), fatal ischaemic stroke (aHR = 1.58, 95% CI 1.17–2.12, P = 0.003) and unclassified stroke (aHR = 1.81,95% CI 1.06–3.08, P = 0.03), while no significant association was obtained between the LYM and the risk of fatal strokes after adjustments for a series of factors (Supplementary Table 1).
The NLR in Relation to the Risk of Fatal Stroke Occurrence
In a restricted cubic splines model, there is an increased trend of the relationship between the NLR and the risk of fatal all stroke occurrence, and the cutoff value of NLR level was of 1.90 after a multivariable adjustment were made (Figure 2). In both Table 2 and Supplementary Figure 1, the NLRs had an increasing trend for risks of fatal all stroke (P for trend <0.001) and fatal ischaemic stroke (P for trend = 0.003); the participants in the fourth NLR quartile had respectively an increased risk of fatal all stroke (aHR = 1.52, 95% CI 1.23–1.88, P < 0.001) and fatal ischaemic stroke (aHR = 1.64, 95% CI 1.22–2.21, P = 0.001) after adjustment for a series of factors. Similar results were observed for fatal all stroke (men: aHR = 1.59, 95% CI 1.13–2.26, P = 0.008; women: aHR = 1.45, 95% CI 1.11–1.90, P = 0.007) and fatal ischaemic stroke (women: aHR = 1.71, 95% CI 1.15–2.55, P = 0.008). Table 3 and Supplementary Figure 2A show higher NLRs in relation to an increased risk of fatal all stroke (aHR = 1.58, 95% CI 1.16–2.15, P = 0.004) and fatal ischaemic stroke (aHR = 1.96, 95% CI 1.27–3.04, P = 0.003), and an increasing trend was obtained for fatal all stroke (P = 0.005) and fatal ischaemic stroke (P = 0.008) after further hs-CRP adjustment.

Association of NLR with the risk of fatal stroke with the RCS model (n = 27,799). The solid blue line is the multivariable adjusted hazard ratio, with dashed lines showing 95% confidence intervals with three knots. A multivariate model, adjusted for sex, age, diabetes, hypertension, dyslipidaemia, smoking, alcohol consumption, physical activity, body mass index, self-rated health, cancer, genitourinary diseases, chest disease and platelet count, was used.
Association of the NLRs with fatal stroke occurrence in the GBCS (n = 27,799).
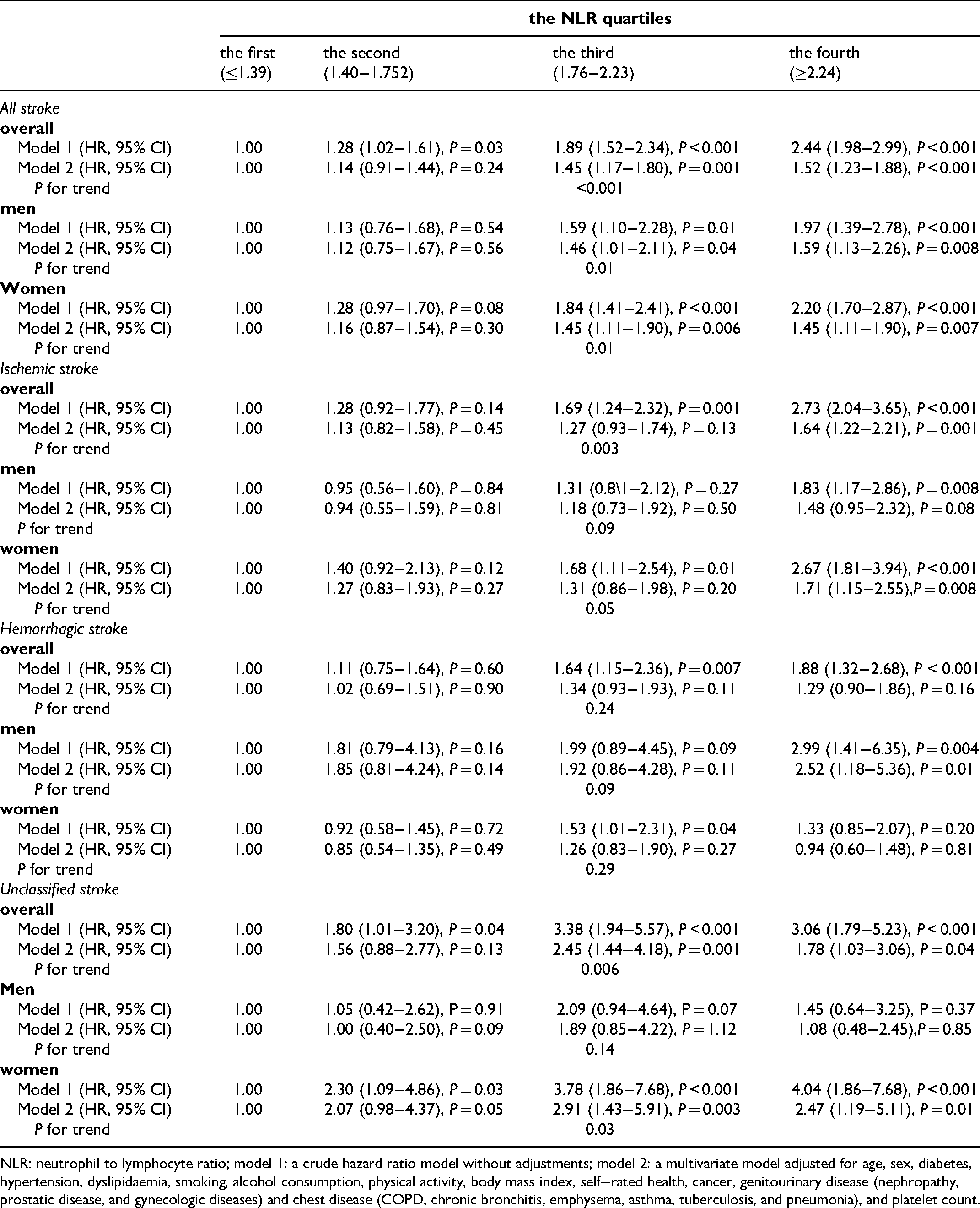
NLR: neutrophil to lymphocyte ratio; model 1: a crude hazard ratio model without adjustments; model 2: a multivariate model adjusted for age, sex, diabetes, hypertension, dyslipidaemia, smoking, alcohol consumption, physical activity, body mass index, self−rated health, cancer, genitourinary disease (nephropathy, prostatic disease, and gynecologic diseases) and chest disease (COPD, chronic bronchitis, emphysema, asthma, tuberculosis, and pneumonia), and platelet count.
Association of NLRs with fatal stroke occurrence among participants without CVD at baseline and further hs-CRP adjustment (n = 10,991).

NLR: neutrophil to lymphocyte ratio; hs-CRP: high-sensitivity C-reactive protein; CVD: cerebrovascular disease (including coronary heart disease, angina, myocardial infarction and peripheral vascular disease); model 1: a crude hazard ratio model without adjustments; model 3:a multivariate model adjusted for age, sex, diabetes, hypertension, dyslipidemia, smoking, alcohol consumption, physical activity, body mass index, self-rated health, cancer, and genitourinary disease (nephropathy, prostatic disease, and gynecologic diseases), chest disease (COPD, chronic bronchitis, emphysema, asthma, and tuberculosis, pneumonia), platelet count and hs-CRP.
Additionally, the participants in NLRs >1.75 had an increased risk of fatal all stroke (aHR = 1.43, 95% CI 1.16–1.75, P = 0.001) and fatal ischaemic stroke (aHR = 1.55, 95% CI 1.16–2.09, P = 0.003), compared to those in NLR≤1.75; Similar results for fatal all stroke (aHR = 1.21 95% CI 1.11–1.32, P < 0.001) and fatal ischaemic stroke (aHR = 1.32 95% CI 1.18–1.47, P < 0.001) were observed when the NLRs were conducted as a continuous variable (Supplementary Table 2, Supplementary Figure 2B and 2C).
The NLR Changes in Relation to the Risk of Fatal Stroke Occurrence
The basic characteristics of the participants at the 1stfollow-up are shown in Supplementary Table 3. Compared to those with a stable NLR (from −5% to 5%), the population with a NLR gain (at >5%) had higher proportions of active activity, hypertension, chest diseases and NEUT counts; lower proportions of, physical activity; and lower LYM counts (all P < 0.05). Table 4 and Supplementary Figure 3 show the association between the risk of fatal stroke and the NLR change from baseline (from September 2003 to February 2008) to the first follow-up (from March 2008 to December 2012). The participants with NLR increase in excess of 5% had a significant risk of fatal all stroke (aHR = 1.70, 95% CI 1.13–2.57, P = 0.01), compared to the stable participants.
Association of NLR change with fatal stroke occurrence in the GBCS (n = 11039).
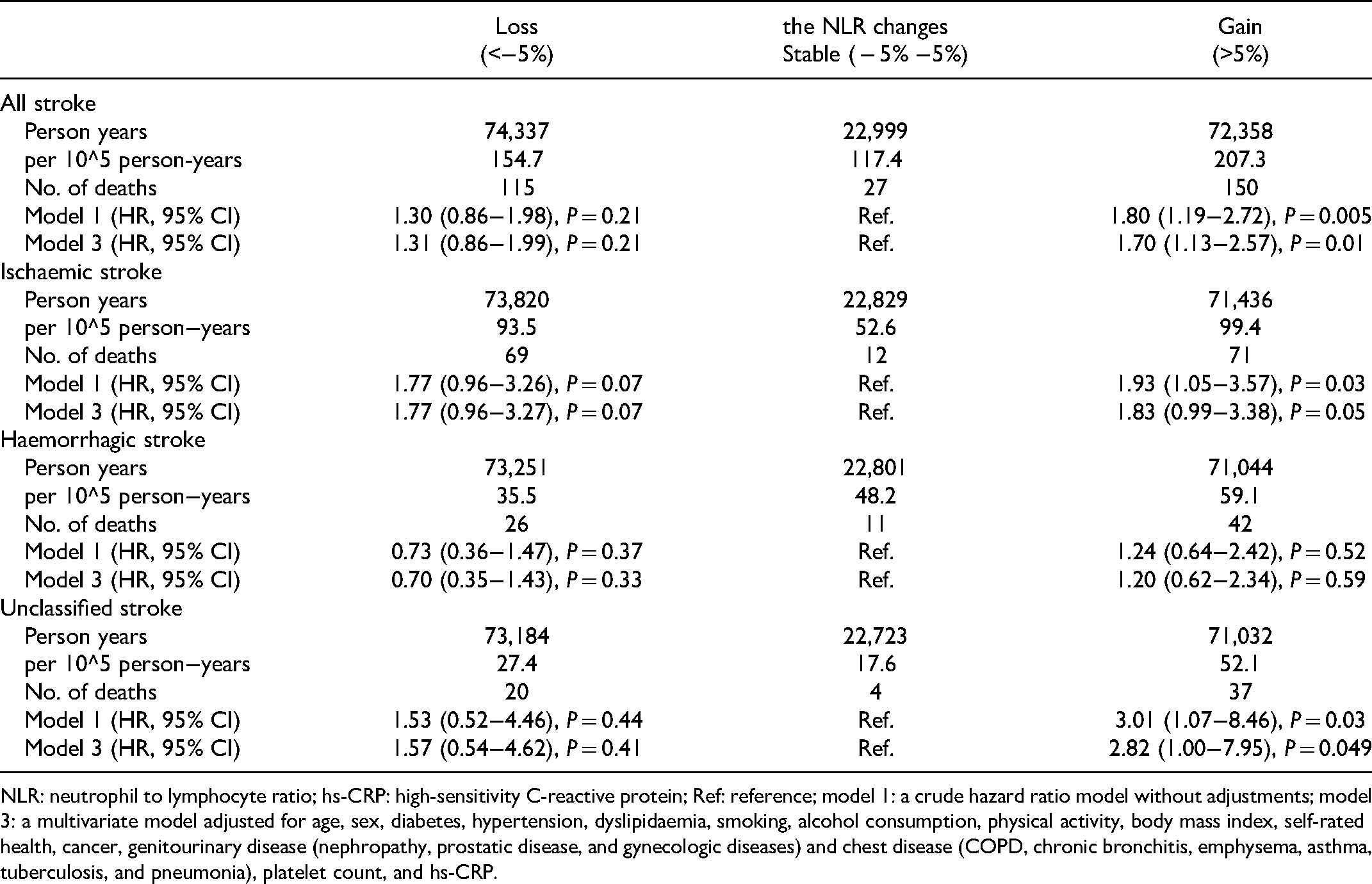
NLR: neutrophil to lymphocyte ratio; hs-CRP: high-sensitivity C-reactive protein; Ref: reference; model 1: a crude hazard ratio model without adjustments; model 3: a multivariate model adjusted for age, sex, diabetes, hypertension, dyslipidaemia, smoking, alcohol consumption, physical activity, body mass index, self-rated health, cancer, genitourinary disease (nephropathy, prostatic disease, and gynecologic diseases) and chest disease (COPD, chronic bronchitis, emphysema, asthma, tuberculosis, and pneumonia), platelet count, and hs-CRP.
Discussion
In this study, we found that higher NLR and its change were associated with an increased risk of fatal stroke occurrence, and the associations were independent of age, sex, hypertension, diabetes, dyslipidaemia, smoking, alcohol consumption, physical activity, BMI, self-rated health, cancer, GD, chest disease, platelet count and hs-CRP. This is the first report dressing the relationship between the NLR and its change and the risk of fatal stroke occurrence in a relatively healthy older population.
Among ischaemic and haemorrhagic stroke the former accounts for more than 80%. 24 In fact, chronic inflammation has come out prior to stroke onset and will follow after stroke happened. 25 Inflammatory response has also been known as a mechanism in which both the susceptibility and outcome was altered in stroke. 26 The NLR has been linked to a cardiovascular or stroke disease.14–16,27
Atherosclerosis is accompanied by a chronic vascular wall inflammation or endothelial dysfunction, and its plaque was known as the most common cause for ischaemic stroke. 28 Neutrophil promote a rupture or erosion of atherosclerotic plaques, lead to thrombosis and trigger acute stroke events.29,30 The NETs (neutrophil extracellular traps) and the main components were significantly increased in acute ischaemic stroke 31 and thrombus, especially in cardiogenic cerebral embolism. 32 The B2 cells (a type of lymphocyte) contributed to atherosclerosis progress, but the B1a cells (a type of lymphocyte) played a role of anti-atherosclerotic. 33 Higher NLR was an independent predictor for intracranial atherosclerosis, 34 and was associated with an increased risk of ischaemic stroke among Korean aged 30–75 years, 35 and the subjects with arterial fibrillation but without a history of stroke and transient ischaemic attack. 36 We observed not only higher NLR but also higher its change was associated with an increased risk of fatal all stroke and fatal ischaemic stroke. These results are mutual proofs in connection with the roles of total white blood cell and neutrophil in the risk of fatal stroke, 21 it suggests that a chronic “low-grade” systematic inflammation and inflammatory response has being happened prior to stroke occurrence.
Unlike previous clinical studies revealing a predictor role of NLR on 30-day mortality and morbidity 17 and ND 18 after ICH, sHT after acute ischemic stroke, 19 and PSCI after stroke, 20 our work focused on relative healthy older populations and explored the relationship between the NLR and the risk of fatal stroke occurrence, which have expanded the NLR” practical applications in not only prognosis and judgment on patients with strokes but also forewarning a burden of pre-existing chronic low-grade systemic inflammation, especially in a large cities’ relative healthy older population. This is because a series of study data from relatively healthy elders in south China, and each participant had been made an appointment in advance to ensure good health and was able to come the designated place by himself/herself. 22 Additionally, individuals have different white blood cell background, which can fluctuate by 15% within one day. Therefore, we considered unhealthy conditions, random walks and native operation bias as being factors that were related to WBC variation in the baseline and the first follow-up, and each participant had enough time to rest for sampling, and be measured by a fixed analyzer. Our results appear to be consistent with the existing body of literature highlighting the adverse cerebrovascular consequences of inflammation, which indicates that a continuous chronic inflammation increases the risk of fatal stroke occurrence.
In our study, a mean follow-up of 11.5 years makes this a large, prospective design for a study of general population in South China, and individuals completed a physical examination and questionnaire involving a total of 800 questions. Thus, the acquired information allows for systemic adjustments for additional potential confounding factors. However, there are limitations in this study. First, we obtained only the death information via a record linkage; therefore, our results with death as the only outcome are obviously weakened due to a lack of analysis on other clinical outcomes of stroke events. Second, the subjects could not represent Chinese individuals due to the limitations involving the general population in South China, other cohorts and ethnic population should be introduced for further verified in the future.
Conclusions
Higher NLR and longitudinal NLR increase in excess of 5% were associated with an increase risk of fatal stroke occurrence; the clinicians should pay more attention to asymptomatic inflammatory characteristics in relatively healthy older population.
Supplemental Material
sj-pptx-1-cat-10.1177_10760296221098720 - Supplemental material for Association of Neutrophil-to-Lymphocyte Ratio with the Risk of Fatal Stroke Occurrence in Older Chinese
Supplemental material, sj-pptx-1-cat-10.1177_10760296221098720 for Association of Neutrophil-to-Lymphocyte Ratio with the Risk of Fatal Stroke Occurrence in Older Chinese by Zhi-bing Hu, Qiong-qiong Zhong, Ze-xiong Lu and Feng Zhu in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
sj-docx-2-cat-10.1177_10760296221098720 - Supplemental material for Association of Neutrophil-to-Lymphocyte Ratio with the Risk of Fatal Stroke Occurrence in Older Chinese
Supplemental material, sj-docx-2-cat-10.1177_10760296221098720 for Association of Neutrophil-to-Lymphocyte Ratio with the Risk of Fatal Stroke Occurrence in Older Chinese by Zhi-bing Hu, Qiong-qiong Zhong, Ze-xiong Lu and Feng Zhu in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Acknowledgements
The Guangzhou Biobank Cohort Study investigators included Guangzhou Twelfth People's Hospital: Weisen Zhang, Min Cao, Tong Zhu, Bin Liu, and Caoqiang Jiang (Co-PI); The University of Hong Kong: C.M. Schooling, S.M. McGhee, G.M. Leung, R. Fielding, and Taihing Lam (Co-PI); The University of Birmingham: P. Adab, G. Neil Thomas, and Karkeung Cheng (Co-PI).
Author Contributions
ZBH and ZQQ contributed equally to this paper for data collection and analysis. ZXL contributed partly to this paper for data collection and analysis. FZ contributed to the study design and wrote the manuscript. All authors reviewed the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Guangzhou Science and Technology Bureau, Guangzhou, China (grant numbers 201704030132, 202102080467), Major Science and Technology Project of Guangzhou Municipal Health Commission (grant number 2021A031003), and Guangzhou Municipal Key Medical Discipline (2021-2023). The funders had no role in the study design, data collection and analysis, the decision to publish, or the preparation of the manuscript. The work was not funded by any industry sponsors.
Data Availability Statement
The datasets used and/or analyzed in this study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Guangzhou Medical Ethics Committee of the Chinese Medical Association. All participants signed informed consent forms before participation. All methods in this study were performed in accordance with the Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.