
Abstract
Inflammation plays an important role in the pathophysiology of vascular disease. In this review, we consider the associations between the neutrophil–lymphocyte ratio (NLR; an indicator of inflammation) and vascular disease and its associated risk factors. The NLR has received attention due to its role as an independent prognostic factor for coronary artery disease. The NLR can also be affected by atherosclerotic risk factors, such as hypercholesterolemia, metabolic syndrome, diabetes, and hypertension. Importantly, it can predict mortality in cardiovascular diseases. There are also reports of a positive correlation between the NLR and commonly used inflammatory markers. Inflammation is important not only in pathophysiology but also clinical outcomes of many diseases. The NLR is a widely available, easily derived, and reproducible marker of inflammation. Unlike many other inflammatory markers, the NLR is inexpensive and readily available and it provides additional risk stratification beyond conventional risk scores.
Introduction
Elevated levels of systemic inflammatory markers are associated with cardiovascular disease (CVD). 1 The white blood cell (WBC) count is a useful inflammatory biomarker in clinical practice. The neutrophil–lymphocyte ratio (NLR) can also be an indicator of systemic inflammation. 2 The NLR is calculated by dividing the neutrophil count by the lymphocyte count. 3 This ratio is easily accessible inflammatory marker with predictive power for death, myocardial infarction, and high risk of coronary artery disease (CAD). 4 –6 Furthermore, many epidemiological studies have highlighted that chronic low grade inflammation, as measured by the NLR, has also been linked to risk factors like diabetes mellitus (DM), hypertension, metabolic syndrome (MetS), obesity, hyperlipidemia, lifestyle habits, and endothelial dysfunction (Figure 1). 7,8
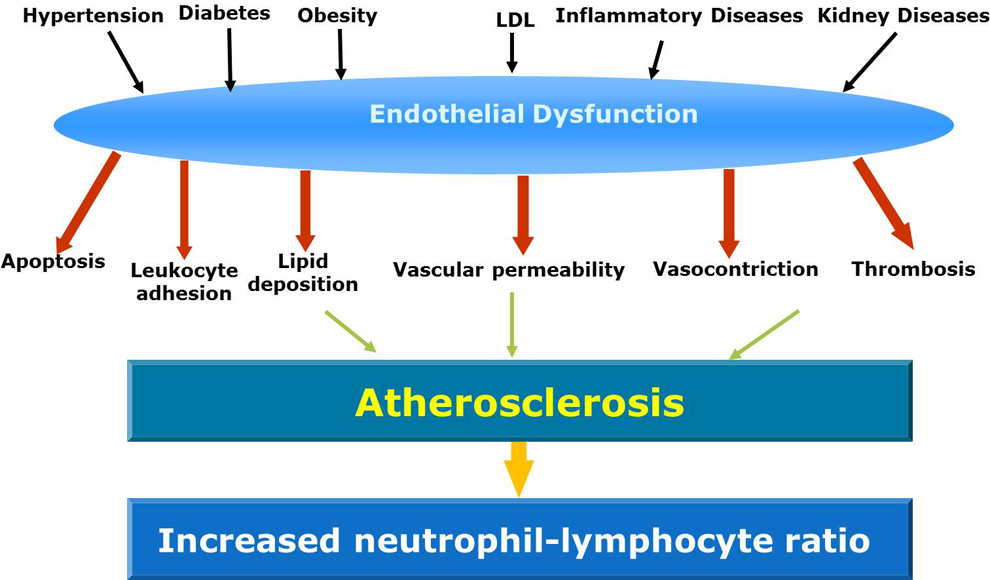
Endothelial dysfunction can be observed in several diseases. Endothelial dysfunction can lead to higher neutrophil–lymphocyte ratio.
Cardiovascular Disease and NLR
The relationship between the NLR and CVD is not fully defined; systemic factors like inflammation, endothelial dysfunction, and oxidative stress may play a role. 9 The interaction between neutrophils and endothelial tissue has been hypothesized to cause increased damage to the endothelium. Severe inflammation is present in cases of ischemic tissue damage, in which leukocytes play a key role. 10 Chronic inflammation in the arterial wall plays a crucial role in the initiation and progression of atherosclerosis. Several processes have been postulated, including plaque disruption caused by neutrophil infiltration and increased neutrophil platelet adhesion. Direct visualization in recent studies conducted in animal models has shown that there is a neutrophil invasion of the atherosclerotic plaque. 11 In addition, neutrophils may make plaques more vulnerable through the release of proteolytic enzymes, arachidonic acid derivatives, and superoxide radicals. 11 Neutrophils also secrete inflammatory mediators and are associated with an acute inflammatory response to tissue injury. 11
A higher NLR, even within the normal WBC count range, has been associated with atherosclerotic events. 4 The NLR also has prognostic importance in CVD. The relation between atherosclerosis progression and leukocyte subtype was evaluated. 12 The NLR was a more accurate marker of cardiac adverse events rather than the differential leucocyte count. 12 A high NLR is a predictor of progression of atherosclerosis. 10 Admission NLR is an independent predictor of in-hospital and 6-month mortality in patients with acute coronary syndromes (ACSs). 13 The NLR was also recently shown to be an independent predictor of death/myocardial infarction in patients undergoing coronary angiography. The NLR has been investigated as a predictor of long-term mortality in patients undergoing percutaneous coronary intervention (PCI). 12 The NLR was a strong independent predictor of long-term mortality after ST-segment elevation myocardial infarction (STEMI) treated with very early revascularization. 14 Also, Soylu et al 15 investigated the relationship between the NLR and coronary flow velocity after PCI in patients presenting with STEMI. They concluded that the NLR was an independent indicator for no-reflow development in these patients. 15 The NLR may predict contrast-induced nephropathy in patients undergoing PCI. 16 Gibson et al investigated leukocyte subtypes such as the NLR in patients undergoing coronary artery bypass graft (CABG). 17 The authors concluded that an elevated NLR is associated with a poorer survival after CABG. Moreover, they found that the prognostic utility is independent of other recognized risk factors. 17 Among patients with higher NLR, minimally invasive CABG was associated with a significantly improved survival compared with sternotomy CABG. 18
The NLR has been associated with poor outcomes in patients with CVD. Hartaigh and coworkers 19 found a significant relationship between the NLR and cardiovascular (CV) deaths. In-hospital major adverse cardiac events (MACEs) were significantly higher in patients with no reflow, and there was a significant and positive correlation between high sensitivity C-reactive protein (hsCRP) and the NLR. 20 The NLR is also an inflammatory marker of MACEs in both ACSs and stable CAD. Patients with the lowest NLR had fewer MACEs compared with the highest NLR. 21
Cardiovascular Disease Risk Factors and NLR
The NLR has been proposed as a useful biomarker to predict CV risk. 22 Inflammation is present in MetS, 23 and there is evidence that the NLR in MetS may be an early marker of developing CV events. 24
The vascular inflammatory process plays a role in the pathophysiology of hypertension, 25 and a high NLR may reflect vascular inflammation in these patients. 8 Antihypertensive treatment may improve CV outcomes and decrease biomarkers such as the NLR. 26
Several studies have suggested that chronic, subclinical inflammation plays a role in the development of insulin resistance, which may then proceed to overt DM. 27 Risk factors for DM, such as obesity, smoking, and physical inactivity, are associated with chronic low-grade inflammation. 27 Patients with DM have worse long-term outcomes after acute myocardial infarction (AMI) than nondiabetics. 28 Increased NLR post-AMI is an independent predictor of MACEs in diabetics. 28 In another study, patients with DM had significantly higher NLRs than those of the healthy control group, and also the NLR of the patients with diabetic retinopathy (DR) was higher than those of the patients without DR with DM. 29 Furthermore, there was a statistically significant difference between NLR in diabetic patients with and without complications. 30 The NLR is a significant independent predictor of MACEs in diabetic patients. 21 Furthermore, an increased NLR may be associated with microvascular complications of DM in the elderly patients. 30
The NLR was negatively correlated with high-density lipoprotein (HDL), which has anti-inflammatory activity. The NLR is significantly elevated in patients with low HDL-cholesterol when compared with control participants. 31
In a landmark clinical study, increased inflammation was found to be common in patients with chronic kidney disease (CKD) and associated with increased adverse CV events. 32 The authors demonstrated that the NLR is independently related to endothelial dysfunction and could predict composite CV end points independent of traditional confounding factors in patients with moderate to severe CKD. 32 Overall and CVD-free survival rates were compared according to NLR in peritoneal dialysis patients. The NLR was a strong predictor of overall and CV mortality in these patients. 33 The NLR might provide significant information regarding inflammation in CKD including predialysis and dialysis patients. 34
The WBC count is an independent predictor of CV events and mortality, and the NLR is independently associated with CAD severity and 3-year clinical outcome. The NLR appears additive to conventional risk factors and commonly used biomarkers. 35 The NLR also relates to the SYNTAX score (an index of the severity of coronary artery lesions). The NLR was significantly correlated with angiographic severity of ACS assessed by SYNTAX score. In patients with STEMI, an NLR ≥4.5 independently predicted an occluded infarct-related artery on initial angiography. 36
The preoperative NLR identifies patients at increased risk of death within 2 years of major vascular surgery. 37 This simple index demonstrates the balance of neutrophils, the active inflammatory component, with lymphocytes the regulatory and “protective” component. 37 Therefore, a higher NLR represents a greater level of inflammation. A study determined whether the NLR is related to atherosclerosis as measured by brachial-ankle pulse wave velocity and coronary calcium score (CCS). A higher NLR was independently associated with arterial stiffness and CCS. 38 An elevated NLR is associated with a poorer limb survival after embolectomy. 39 Moreover, the preoperative NLR is an independent predictor of saphenous vein graft patency in patients after CABG. 40 Also, a preoperative NLR >5 may be a significant predictor of 30-day mortality and long-term outcome in elective and urgent open abdominal aortic aneurysm repair. The NLR may have identified patients with subclinical CV disease. 41
Chronic inflammation was found to be correlated with coronary (coronary artery calcification) and thoracic periaortic calcification. 42 The NLR may also be associated with troponin levels in patients with ACS. 43
An increased NLR is significantly associated with patients at high risk of critical limb ischemia and other vascular end points. 44 In patients with peripheral arterial disease, after adjustment of several vascular risk factors, an NLR >3 was an independent predictor of long-term CV mortality. 45
A meta-analysis showed that the NLR is a predictor of all-cause mortality and CV events in patients undergoing angiography or cardiac revascularization. 46 Also, the NLR can reclassify upward patients at intermediate-risk category according to the Framingham risk score. 47
Other Inflammatory Diseases and the NLR
Behçet disease (BD) is a chronic, multisystemic, and inflammatory disorder characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions. 48 It is a systemic immunoinflammatory vasculitis. 49 Several studies have reported indirect evidence of endothelial dysfunction in BD. 50 We assessed the relationship between NLR and BD. There were statistically significant differences in NLR between the patients with BD and controls. 51 Receiver–operating characteristic curve analysis suggested that the optimum NLR cutoff point for patients with BD was 1.29, with a sensitivity, specificity, negative predictive value, and positive predictive value of 97%, 77%, 96%, and 75%, respectively (P < .001; Figure 2). 51 We concluded that the higher NLR may be related to endothelial dysfunction and may reflect disease activity in patients with BD.
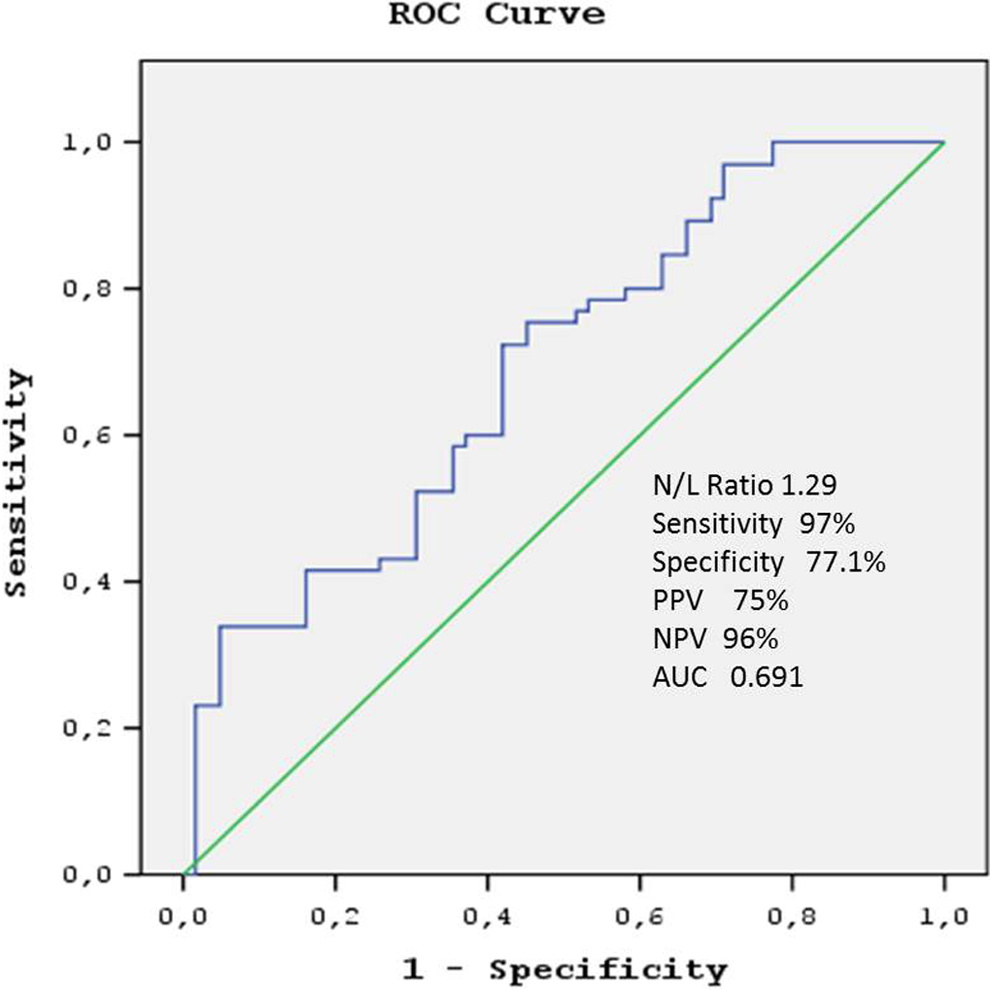
Receiver–operating characteristic curve of the neutrophil–lymphocyte ratio for predicting Behcet disease. PPV indicates positive predictive value; NPV, negative predictive value; AUC, area under the curve.
Inflammatory Markers and the NLR
In a large mortality study, 52 involving patients with STEMI who underwent primary PCI, an elevated NLR on admission was strongly correlated with hsCRP levels. In another study, correlation analysis revealed a positive correlation between hsCRP and NLR in patients with BD. 51 Some studies investigated the correlation between NLR and another indirect inflammatory marker, the carotid intima–media thickness (cIMT). We reported a positive correlation between the cIMT and NLR in patients with BD. 51 We also showed that the NLR was positively and moderately correlated with cIMT in slow coronary flow and control participants. 53
In addition to the NLR, a full blood count can include measurements such as mean platelet volume (MPV), platelet distribution width (PDW), red cell distribution width (RDW), and platelet–lymphocyte ratio (PLR). 54 These indices have also been used as inflammatory markers and are independent predictors of CVD and have been compared with the NLR in various clinical situations. 10,54 –57 The results have been variable but the NLR has been usually the best marker of disease progression. One key issue is to establish whether combinations of these markers are more effective predictors of the progression of several diseases compared with using a single marker.
Platelet activation is a link in the pathophysiology of diseases prone to thrombosis and inflammation. Numerous platelet markers, including MPV and PDW, have been investigated in connection with both thrombosis and inflammation. Ma et al 58 have investigated that whether MPV is independently associated with the cIMT in normotensive, euglycemic, and normolipidemic middle-aged and elderly adults. Mean platelet volume is independently associated with carotid atherosclerosis in normotensive, euglycemic, and normolipidemic males. The MPV could be an easily measured marker of atherosclerosis for males. In addition, it is well known that platelet volume indices are associated with adverse outcomes undergoing PCI. Kim et al 59 investigated whether the association between platelet size and clinical outcomes is the result of high residual platelet reactivity after antiplatelet therapy in patients with large platelets. They concluded that platelets with a higher volume are associated with high residual platelet reactivity after conventional dual antiplatelet therapy. Mean platelet volume was independently and significantly associated with adverse CV outcome in patients with asymptomatic carotid atherosclerosis. 60 Mean platelet volume is also a predictor of cardiac death after PCI. 61 Mean platelet volume is positively associated with the GRACE risk score, and it may complement the scoring system in predicting CVD events in patients with ACS. 62 Platelet distribution width measures the variability in platelet size and is a marker of platelet activation. Platelet distribution width may be used as a novel inflammatory marker. Admission PDW and MPV are independent correlates of no reflow and in-hospital MACEs among patients with STEMI undergoing primary PCI. 63 The PDW is a readily available platelet index that can predict coronary total occlusion. 64
Recent studies have reported increased RDW has been associated with adverse outcomes in CAD. 65 In a previous study, we have investigated RDW level in patients with cardiac syndrome X (CSX) and compare patients having CAD and normal subjects. Patients with CSX and CAD had significantly higher RDW measurements compared with controls. The relationship between CSX and higher RDW level suggests that endothelial dysfunction may also contribute to the etiopathogenesis of the CSX as it does with CAD. 66 Also, RDW is closely related to the poor prognosis and adverse events of CVD. Kurtul et al 67 have investigated the association of serum RDW levels and in-stent restenosis (ISR) after coronary stenting with bare-metal stent in patients with stable CAD. They concluded that increased serum RDW levels were independently associated with bare-metal ISR in patients with stable CAD. The RDW has been shown to predict not only CV mortality but also all-cause mortality. 68 The RDW has been described to be a stronger biomarker for CHD death than widely used inflammatory markers like hsCRP. 69
Furthermore, in addition to the NLR, some ratios like the PLR have been shown to be an inflammatory marker. A recent study 70 investigated the relationship between the PLR and in-hospital mortality in patients with ST-elevated AMI. They showed that the PLR is an independent predictor of CV mortality in patients with ST-elevated AMI. Yildiz et al 71 evaluated the utility of the preprocedural PLR and NLR for predicting no reflow in patients undergoing PCI for the treatment of STEMI. They concluded that high preprocedural PLR and NLR are significant and independent predictors of no reflow in patients undergoing primary PCI. 71 In addition to this study, Ciçek et al 72 have investigated the effect of combination of NLR and PLR in predicting in-hospital and long-term mortality in patients undergoing primary PCI. The combination of PLR and NLR can be useful for the prediction of in-hospital and long-term mortality in patients undergoing primary PCI.
Major Confounding Factors
The NLR may be related to nonvascular conditions associated with inflammation. For example, several types of cancer and their progression have been linked to the NLR. 73 –75 Cancer is a common condition that may coexist with CVD. Cancer itself may be associated with an increased risk of thrombosis.
In addition, some medications may affect the NLR. The NLR significantly decreased after statin therapy. 76 Antihypertensive therapy like nebivolol significantly lowered the NLR. 26 In this context, medication should be considered, when the NLR is assessed.
Conclusions
The NLR can be easily calculated from the differential WBC count, which is widely available and routinely performed. Unlike many other inflammatory markers, the NLR is inexpensive and readily available and provides additional risk stratification beyond conventional risk scores (eg, to predict in-hospital and long-term mortality).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.