
Abstract
Venous thromboembolism (VTE) is a recognized complication of hospital stay in young patients in many developed countries, but such an information is largely unavailable from a low middle-income country (LMIC). This study aimed at identifying the frequency, risk factors, treatment options and outcome of deep venous thrombosis/pulmonary embolism (DVT/PE) in pediatric population in a tertiary care center from a LMIC. International classification of disease, ninth revision (ICD-9) was used to identify VTE in patients aged 0-18 years during January 2011 to September 2019. In-house computerized system was used to collect data for demographics, clinical and laboratory details. SPSS version 19 was used to analyzed data. The study was approved by Institutional ethical review committee (3872-Pat-ERC-15). During the study period, 134617 pediatric patients were hospitalized, DVT/PE was observed in 77 unique patients (47 males and 30 females) with a median (IQR) age of 14 (5-16) years equivalent to 5.9 VTE events /10,000 hospital admissions. Malignancy, community acquired infections and autoimmune diseases were the predominant risk factors (75%) in adolescent age-group while surgery for congenital heart anomalies was the primary reason (71%) in infants. Overall, lower extremity thrombosis was the most frequent (51%) followed by pulmonary embolism (25%). and upper extremity thrombosis (24%). Enoxaparin and unfractionated heparin were mainly used to treat VTE and all-cause mortality was 13% in the cohort studied. We observed substantial VTE events in pediatric patients during their hospital stay in a tertiary care center of a low-middle income country.
Introduction
VTE is no longer considered a disease of adults because of its increasing recognition in the pediatric population. In the early 1990s, the reported incidence of VTE was only 5.3 events per 10,000 pediatric hospital admissions but rose dramatically to 30-58 events per 10,000 admissions as of 2017. 1 This increased risk may be attributed to improved survival of critically sick children subsequent to an increase usage of central venous catheters, complex interventions, advanced surgical procedures and increasing awareness of VTE among pediatricians. 2,3 Besides hospital risk factors, underlying chronic medical conditions like malignancy, inflammatory disorders and inherited thrombophilia may predispose to VTE in the younger population. 1,4
Situated in South Asia, Pakistan is the sixth most populous country in the world. Like any other developing country, national registry for venous thrombotic disorders is non-existent. Limited single-institutional data had addressed risk factors in hospitalized adult patients. For example, Soomro et al in 2014 described obesity and advancing age as significant risk factors for hospital- acquired-VTE in 170 patients. 5 Though a systematic review analyzed an incidence of 3-13% for hospital acquired VTE in adult patients in Pakistan, a low middle income country 6 but the information regarding epidemiology and risk assessment of pediatric VTE in our local setting is completely lacking. Therefore, this study aimed in assessing the incidence and risk factors of VTE in hospitalized children in a tertiary care center. Secondary aims included evaluating management and outcome of pediatric VTE. This information may assist in devising predictive models for pediatric VTE and need assessment for thromboprophylaxis in hospitalized children in low middle-income countries.
Material and Methods
Setting
The following study was carried out at the Aga Khan University Hospital (AKUH), Karachi- an academic tertiary care center, accredited with Joint Commission of International Accreditation (JCIA) in 2006. It is a 700- bedded combined adult and pediatric hospital with 136 dedicated beds for general peds and hematology-oncology patients along with facilities for neonatal (24 beds), pediatric (8 beds) and pediatric cardiac (4 beds) intensive care units. Clinical and diagnostic information is archived in an in-house computerized data system in a retrievable form.
Study Design, Duration and Data Collection
This was a retrospective study conducted during January 2011 to September 2019 at AKUH. ICD classification 9 was used to identify admitted patients who were diagnosed with VTE during their hospital stay. Pediatric patients of both genders aged 0-18 years were included. Data was retrieved from computerized hospital system and information was cross checked through laboratory and radiology diagnostic systems. Following data was collected for patients with radiologically proven DVT and PE: age at the time of diagnosis, gender, primary diagnosis, type of thrombosis, hospital stay, risk factors, co-morbidities management and outcome. H-VTE was considered if the patients had VTE events during hospital stay or within 90 days of their previous hospitalization. 7 This cutoff is based on the previous reports describing VTE events in surgical and medical patients within 90 days of their discharge from the hospital. 8 Possible risk factors considered for H-VTE were surgery, placement of intravenous lines or central venous catheters (CVC), immobility for ≥3 days, administration of chemotherapy or culture-proven infections during hospital stay. Time to resolution of a thrombus was taken as the interval between identification and resolution in radiological scans.
Statistical Analysis
SPSS version 19 was used for data analysis and statistical tests. The quantitative data was checked for normality through Shapiro-Wilk test. Parametrically distributed data were expressed as means ± SD, whereas non-parametric data were expressed as medians with interquartile ranges (IQR). Multiple regression analysis was used to identify the statistically significant risk factor(s) for pediatric thrombosis. The threshold of significance was a p-value <0.05. VTE rate was determined against total hospital admissions during the defined period.
Ethical Issues
Institutional review board of Aga Khan University (AKU_ERC) approved the study (ERC no 3872-Pat-ERC-15.
Results
Demographics
During the study period, 134617 pediatric patients were hospitalized including 53704 neonates and 27917 infants. ICD classification 9 identified 213 cases for VTE events but 65 patients (30%) did not qualify for further review because of having an alternative diagnosis including superficial femoral vein thrombosis (n = 4), iliac/axillary artery embolism (n = 2), acute respiratory distress syndrome/pulmonary infarction (n = 7), cellulitis of extremities (n = 14) non-occlusive mesenteric ischemia (n = 36) and incomplete information (n = 2). There were 148 unique patients having 153 radiologically-proven thrombotic events including DVT (n = 59), PE (n = 20), cerebral sinus thrombosis (n = 32), splanchnic vein thrombosis (n = 5), Budd-Chiari Syndrome (n = 11), portal vein thrombosis (n = 21) and miscellaneous venous thrombi (n = 5). Table 1 summarized the clinical details of 5 patients who had multiple thrombotic events. Overall incidence of all type-thromboses was 11 per 10,000 hospital admissions.
Characteristic of 5 Patients Having Multiple Venous Thromboembolic Events.
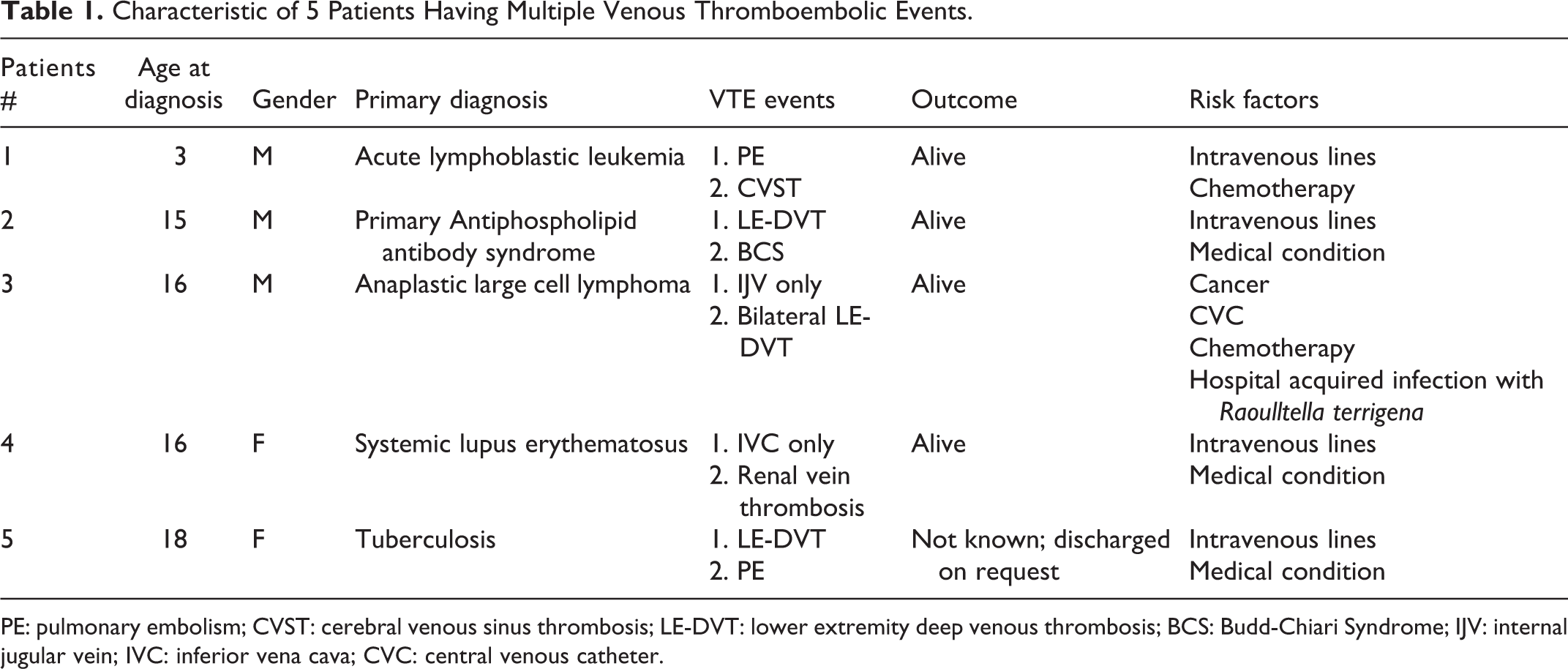
PE: pulmonary embolism; CVST: cerebral venous sinus thrombosis; LE-DVT: lower extremity deep venous thrombosis; BCS: Budd-Chiari Syndrome; IJV: internal jugular vein; IVC: inferior vena cava; CVC: central venous catheter.
Risk Factors for DVT/PE
Patient-related
There were 77 unique patients with DVT/PE including 47 males (61%) and 30 females (39%) with a median (IQR) age of 14 (5-16) years equivalent to a VTE- incidence of 5.9/10,000 hospital admissions in children (Figure 1). Age-trend showed that majority of the patients (57%) were adolescents (Figure 2) while only 3 neonates (of 53704) and 7 infants (of 27917) were below the age of 2 years. Therefore, the incidence of symptomatic VTE per 10,000 respective admissions was 0.5 in neonates and 2.5 in infants. Overall, lower extremity thrombosis was most common VTE (51%) followed by pulmonary embolism (25%) and upper extremity thrombosis (24%). DVT of lower extremity was the commonest VTE-type in each age group as well (Figure 2). None of the patients had a history of thrombosis in first-degree relatives at a young age.

Patient (blue bar) and hospital (red bar) related risk factors for venous thromboembolism in 77 patients.
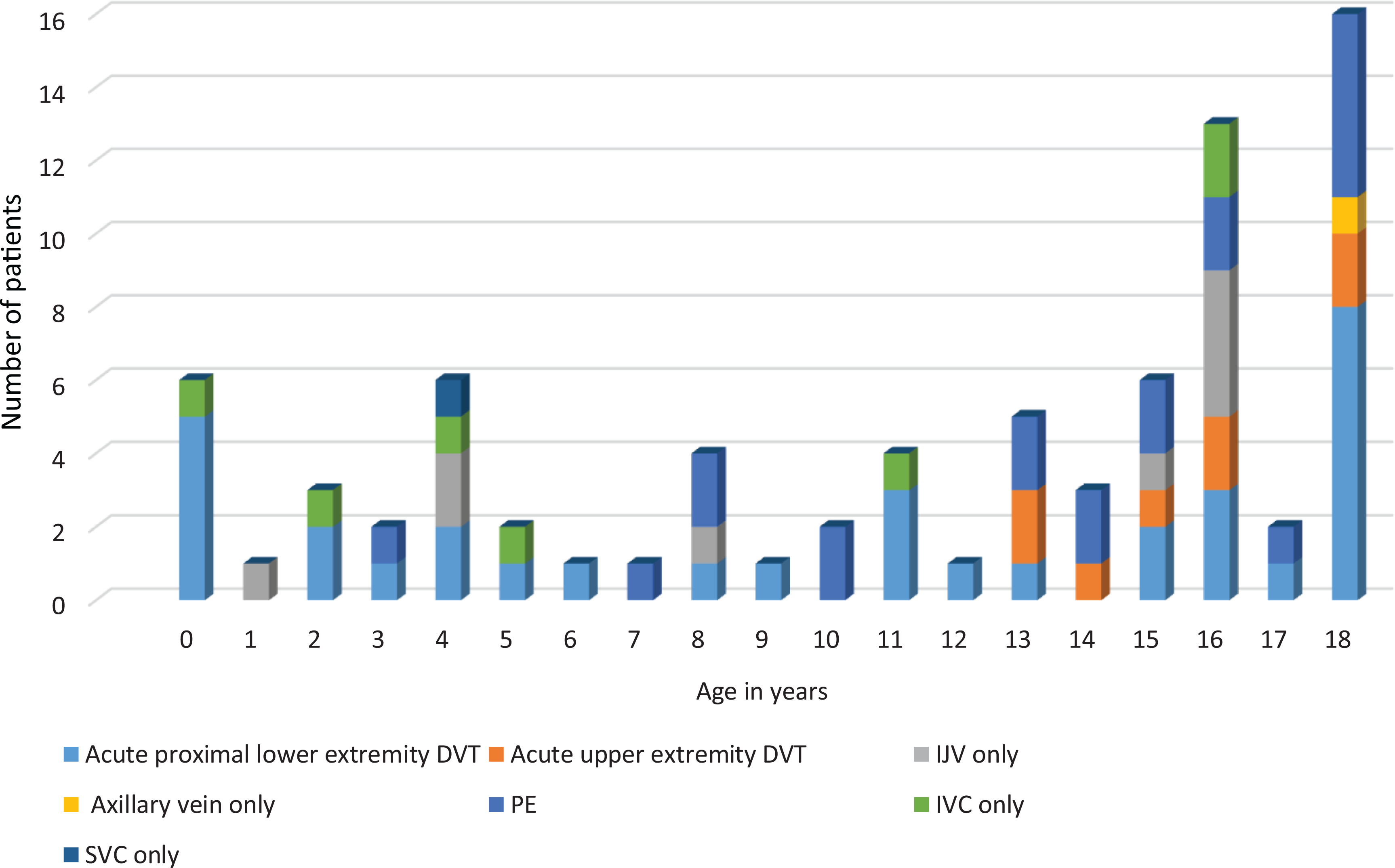
Frequency of various types of venous thromboembolism in 77 pediatric patients at different age groups. DVT: deep venous thrombosis; IJV: internal jugular vein thrombus, IVC: inferior vena cava thrombus; PE: pulmonary embolism and SVC: superior vena cava thrombus.
Table 2 shows that predominant medical conditions were malignancy, community acquired infections and autoimmune diseases in the adolescents while congenital heart anomalies were the frequent reason of hospital admission in infants. Of 27 patients with cancer, there were 12 patients who had hematological neoplasms and 15 had solid organ tumors. In contrast to patients with leukemia/lymphoma who had predominantly upper extremity DVT (57%), majority of patients with solid organ tumors had lower extremity DVT (53%). Community acquired infections included tuberculosis (n = 7), infective endocarditis (n = 3), viral hepatitis (n = 2), osteomyelitis (n = 2), pneumonia (n = 2), sepsis (n = 2) and dengue fever (n = 1).
Demographics of 77 Unique Pediatric in-Patients Having Radiologically Proven Upper (UE) and Lower Extremities (LE) Deep Venous Thrombosis (DVT) and Pulmonary Embolism (PE).
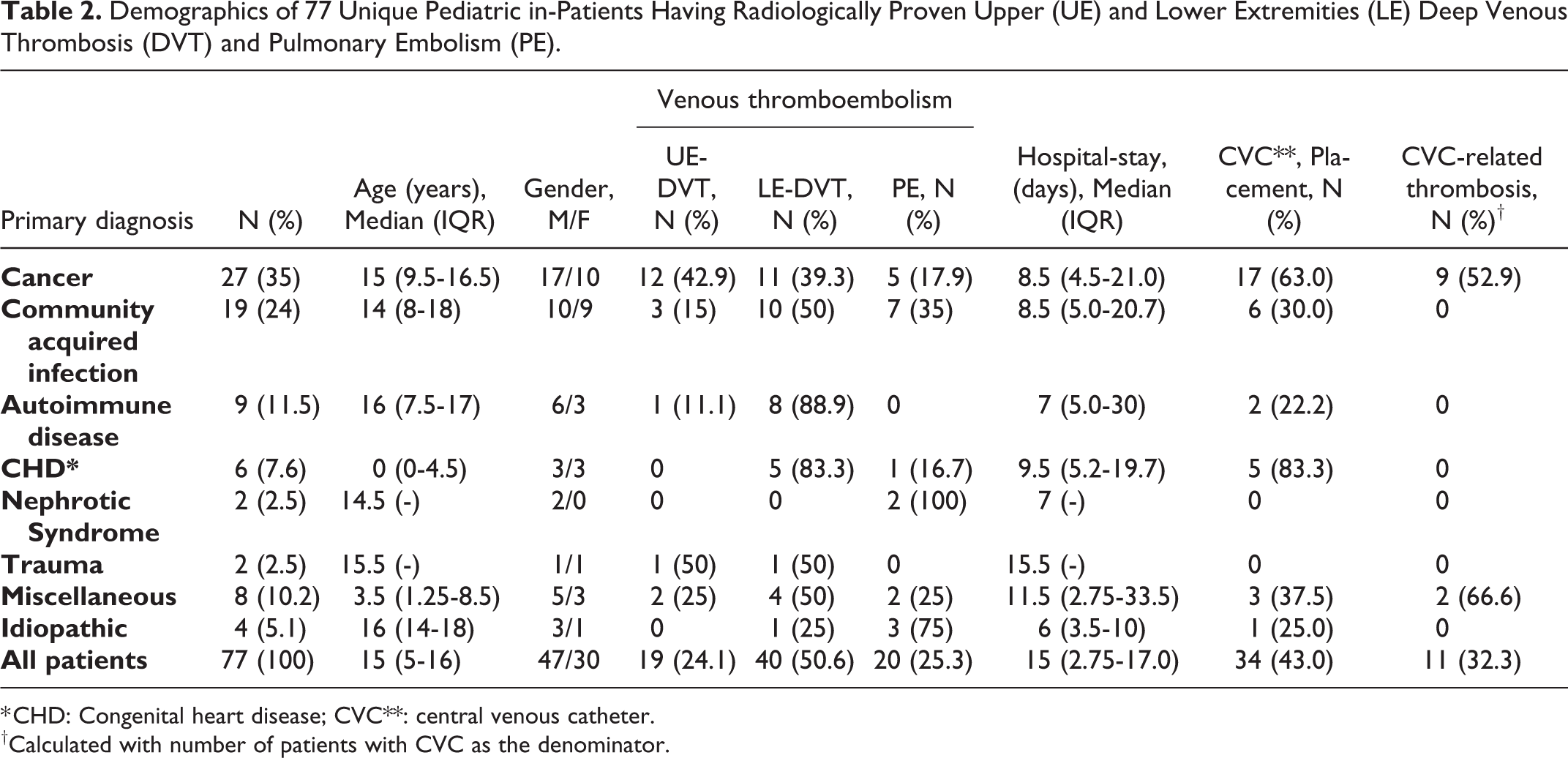
* CHD: Congenital heart disease; CVC**: central venous catheter.
†Calculated with number of patients with CVC as the denominator.
Hospital related
Median hospital stay of all patients was 15 days (IQR 2.75-17) and the most frequent VTE risk factors were placement of intravenous lines (n = 45) or CVCs (n = 34), hospital acquired infections (n = 22), chemotherapy (n = 20) and surgery (n = 14). CVCs were inserted for administration of chemotherapy (n = 15) or intravenous antibiotics/fluids (n = 8), extracorporeal circulation (n = 5), CVP monitoring (n = 3), hemodialysis (n = 2) and cardiac catheterization (n = 1). Catheter related thrombosis occurred in 11 patients (32%) and primarily confined to upper extremity DVT. Nosocomial infection was observed in 21 patients (27.3%) with blood culture-proven gram-positive cocci (n = 14), gram-negative rods (n = 4), gram-positive rods (n = 1) and yeast (n = 2). Staphylococcus was isolated in 62% of patients with CVCs. Majority of patients had 2 or 3 risk factors leading to DVT or PE (Figure 3).

Number of risk factors for pediatric venous thromboembolism in 77 patients.
Overall, 54 patients (70%) developed thrombosis either during their hospital stay or had a history of hospitalization within past 90 days and were classified as H-VTE. These patients had a longer median stay in the hospital compared to 23 patients in whom VTE was unrelated to the hospital admission (11 vs. 5.5 days; p 0.007).
Thrombus Resolution
Serial follow-up scans were done in 31 patients to review the status of thrombus for a median of 39 days (IQR 22.5-81.5). Overall partial/complete resolution of VTE was observed in 26 patients (84%) while thrombosis remained unresolved or extended further in 5 patients (16%). There was no statistically significant difference in the duration of clot resolution in survivors vs. non-survivors (p-value 0.596) and in patients with or without H-VTE (p-value 0.802)
Management and Outcome
All patients were treated primarily with low molecular weight heparin or unfractionated heparin except 7 adolescents who received either warfarin (n = 5) or rivaroxaban (n = 2). Overall, 8 patients were lost to follow up and 9 patients (13.0%) died after a median hospital stay of 7 days (1.5-25) equivalent to a mortality rate of 0.7/10,000 hospital admissions. The characteristic of patients who had a fatal outcome is summarized in Table 3. However, it is difficult to predict the true contribution of VTE to fatality as post-mortem examinations were not performed in any case.
Summary of 9 Patients Having a Fatal Outcome During Hospital Stay.

IVC: Inferior vena cava thrombus; LE-DVT: lower extremity deep venous thrombosis; IJV: Internal jugular vein thrombus and AML: acute myeloid leukemia.
Discussion
Our study indicated some striking differences in pediatric VTE in a LMIC when compared with the similar events in HICs. Firstly, this study showed an incidence of 5.9 VTE events for every 10,000 pediatric admissions in the hospital, which is close to an initial Canadian Registry report (1994) from 15 pediatric tertiary care centers with an incidence of 5.3/10,000. 9 In the later reports (from 2001to 2007), VTE incidence scaled up to 34 to 58 cases per 10,000 hospital admissions as per US data bases for pediatric health information system. 2 This upward trend in childhood VTE is proportional to the advancing interventions and growing recognition of VTE among pediatricians in the developed world. We believe that incidence of pediatric VTE in a LMIC will follow a similar trend in the years to follow.
Secondly, in contrast to bimodal age distribution (infants and teenagers) accounting for majority of VTE admissions in most registries from high-income countries, 2,10 our study showed that only 9% of the patients were neonates. Under representation of neonatal VTE in our study may be related to the fragile infra structure of health system at Pakistan with 70% of births occurring at homes by untrained staff, 11 a high neonatal mortality of 49 per 1000 live births 12 coupled with the poverty, ignorance and sub-optimal availability and access to newborn health services 13 with consequential deaths of newborns prior to any hospitalization.
Approximately 95% of our pediatric patients had underlying medical or surgical conditions like cardiac diseases, cancers, infections and autoimmune disorders that triggered VTE events. These risk factors have similarities with reports from HICs. For example, a study in 76 subjects aged 12-17 years from 8 tertiary UK centers reported reduced mobility (45%), thrombophilia (24%), malignancy (20%), surgery (18%), intake of combined oral contraceptive pill (12%) and congenital venous anomaly (5%) as main risk factors for developing VTE in adolescents. 14 Parallel to the cardiac surgery as the principal risk factor for neonatal VTE in our study, a report from Canada observed post-operative thrombotic complications in 18% of 369 neonates due to cyanosis, surgery, anticoagulant/antiplatelet therapy and blood transfusions. 15 One of the striking risk factors for VTE was the presence of community acquired infections (tuberculosis, viral hepatitis, sepsis etc.) in a quarter of pediatric patients. Though generally not reported in this young age group, community acquired bacteremia was considered as a risk factor in 4213 hospitalized adults in Denmark with an adjusted odds ratio of 1.9 (95% CI 1.4-2.7) compared to the hospital controls. 16 Today, there is enough evidence to believe that infection leads to endotheliopathy, molecular dysfunction and release of inflammatory cytokines to generate intravascular microthrombi. 17
We found lower extremity-DVT as the most frequent VTE and adolescents were principally affected. In contrast, Brown et al in 2020 described VTE in 18 unique neurosurgical patients during 9149 hospitalizations (0.22%) and found an equal distribution of upper and lower extremity DVT while PE was least common. 18 The findings in this study reconcile the significance of defining the risk factors in one’s own setting for designing preventive strategies of VTE.
We found an incidence of 32% for catheter-related thrombosis in our study which is substantially low compared to a multi-institutional Children’s Hospital-Acquired Thrombosis (CHAT) Registry where 73% of the 825 H-VTE cases were CVCs related. 19 Similarly, an Italian study reported CVC as the most important risk factor accounting for 55% of H-VTE events. 20 The use of CVCs results in vascular endothelial damage and direct vascular obstruction both of which contribute to the pathophysiology of thrombosis. 21 Main risk factors for catheter-related thrombosis were identified as male gender, multiple lumen CVCs and upper extremity location. 22 The lower incidence of catheter related thrombosis compared to related studies may be due to less frequent use of central catheters in our setting as supported by a previous report from our institute describing the placement of only 36 CVCs during a duration of 2 ½ years in pediatric oncology patients. 23
Anticoagulants prescribed in our study were primarily enoxaparin (70%) and unfractionated heparin (24%). The management of pediatric VTE is principally derived from treatment guidelines for adult VTE 1 and the choice of LMWH in pediatric population is based on less laboratory monitoring and ease of administration as proven in a number of clinical studies. 2,20,24 Unfractionated heparin is mostly used for children with VTE who are at a high risk of bleeding or who require urgent procedural intervention as it is readily reversible and has other favorable properties. 25 New oral anticoagulants have been shown to be safe and efficacious anti-thrombotic agents in adults but their use in pediatric population is limited. Compared to standard anticoagulants, a recent report from an open labeled randomized clinical trial demonstrated safety and efficacy of rivaroxaban in treating acute VTE in 335 children age 0 to 17 years by reducing thrombotic burden (p 0.012) without increasing the risk of bleeding (HR 1.58 95%CI 0.51-6.27). 26 We observed partial or complete thrombus resolution in more than 80% of the patients in parallel with the previous reports from HMIC where complete vascular canalization was seen in 60 to 74% of children following cardiac surgery 27 and in 42 to 63% of children having underlying medical conditions. 28
The overall mortality of 13% observed in this study, with 78% of deaths occurring within 30 days of VTE diagnosis is consistent with databases of various registries that reported all-cause mortality in the range of 9 – 17%. 29 Hospital or community acquired infection was the predominant risk factor as observed in 50% of pediatric patients who died. Similar findings were reported by Sabapathy et al in 2016 where critical illnesses such as cancer, autoimmune diseases and sepsis were the primary contributors toward mortality in patients with VTE. 30
Though the guidelines for thromboprophylaxis in hospitalized adult patients are well established, the safety and efficacy of such strategies for pediatric population are not clear. 31 However, prophylactic approaches directed at peri- and post pubertal patients with moderate and high risk of thrombosis are like adults with VTE. 32
Strengths and Limitations
The study demonstrated that VTE is frequent in pediatric population admitted in hospitals even in a low middle-income country like Pakistan. It gives an insight of the risk factors and possible interventions that may be designed to prevent thromboses in children. Some of the limitations of our study were its retrospective nature, a short follow-up and single institution-based study. Moreover, initial thrombophilia workup performed during acute thrombotic event was not repeated to see the consistency of the results.
Conclusion
We are beginning to recognize pediatric venous thromboembolism as a complication of hospital stay in a LMIC like Pakistan. Based on an individual risk assessment, a comprehensive thromboprophylaxis plan should be devised to prevent morbidity and mortality associated with VTE in young patients.
Footnotes
Authors’ Note
Data can be provided by corresponding author on request. The study was designed and supervised by BM. Data was collected by MWS, RDU, AA, IA. Initial draft was written by BM, MWS, RDU, AA and IA and critically reviewed by SA. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.