
Abstract
We assessed the rates, trends, and factors associated with venous thromboembolism (VTE) diagnosis among hospitalizations of adults ≥60 years of age during the period 2001 to 2010. Data from the National Hospital Discharge Survey were used for this study. During the period 2001 to 2010, the estimated annual number of hospitalizations in which a VTE diagnosis was recorded, among adults ≥ 60 years of age, ranged from approximately 2 70 000 in 2001 to 4 23 000 in 2010. The rate of such hospitalizations per 1 00 000 US population ≥60 years of age ranged from 581 in 2001 to 739 in 2010. During the period 2001 to 2004, there was a significant increasing trend in the rate of hospitalizations with VTE among women ≥60 years of age. The factors positively associated with an increased risk of VTE diagnosis were female sex, summer and autumn seasons (compared with spring), venous catheterization, cancer, and greater length of hospital stay.
Introduction
Venous thromboembolism (VTE), which consists of deep vein thrombosis (DVT) or pulmonary embolism (PE) or both, is an important public health concern. 1,2 VTE is much more likely to affect people who are older. 3 –6 A 1999 population-based study among residents of Worchester, Massachusetts found that the annual VTE incidence was 57, 138, 348, and 600 per 1 00 000 population among those <55, 55 to 64, 65 to74, and ≥75 years of age, respectively. 4 A study among residents of Olmsted County in Minnesota found that between 1986 and 1990, the annual incidence rates of VTE among persons in age groups that were <60 years of age ranged between 0 and 132 per 1 00 000 population for women and 0 and 149 for men; the rates among persons in age groups that were ≥60 years age ranged from 169 to 829 per 1 00 000 population for women and 163 to783 for men. 3 Hospitalization is also a risk factor for VTE. 4,7,8 A substantial number of patients develop VTE during their hospitalization stay. 9,10 In addition, a large proportion of VTE that occurs in the outpatient settings is associated with recent hospitalization. 4,9 –11 Hospitalization may increase the risk of VTE through individual and synergistic effects of illness, injury, immobility, and surgery. 1,10
Reduction in VTE events among hospitalized older adults will improve patient outcomes. In this context, better epidemiologic understanding of VTE among hospitalized older adults, including identification of the rates of occurrence and demographic and comorbid risk factors, can help in the development and the assessment of effective prevention strategies. Using a large national sample, this study estimated the number and rates (per 1 00 000 population) of hospitalizations of older adults in which there was a recorded discharge diagnosis of VTE (as defined in this study), assessed trends in the rates for the period 2001 to 2010, and identified characteristics and comorbidities associated with an increased likelihood of a VTE diagnosis.
Methods
Data were used from the 2001 to 2010 National Hospital Discharge Survey (NHDS), which was conducted annually until 2010 by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention. A multistage complex sampling design was used to select a sample of hospitals throughout the United States that were short-stay hospitals (average length of patient stay <30 days), had ≥6 inpatient beds, and were not federal, military, or Veterans Administration hospitals. Data collected from sampled discharges from each hospital included patient age, sex, length of hospital stay, month of hospital discharge, and disposition of the patient as well as listed diagnoses and procedures that were indicated using International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) codes. The 2001 to 2009 NHDS recorded up to 7 diagnoses and up to 4 procedures; the 2010 NHDS recorded up to 15 listed diagnoses and up to 8 procedures. More information about the NHDS can be found at the following Web site: http://www.cdc.gov/nchs/nhds.htm.
Hospitalizations in which a discharge diagnosis of VTE was recorded were defined in this study as those having 1 or more of selected ICD-9-CM codes indicating a diagnosis of DVT or PE or both. Because there were changes in ICD-9-CM codes for DVT during the period 2001 to 2010, there were some differences in the ICD-9-CM codes used to identify DVT diagnoses as per our study definition during the selected time periods in this study. The ICD-9-CM codes used for different time periods are presented in Table 1. We assessed the associations between VTE diagnosis and selected patient- and hospitalization-related characteristics, including age group, sex, length of hospital stay, season of hospitalization (based on the discharge month), venous catheterization, and the medical conditions of cancer (all types, including those indicated to be in remission), heart failure, stroke, chronic obstructive pulmonary disease, diabetes, hypothyroidism, autoimmune and/or inflammatory diseases (inflammatory bowel disease, systemic lupus erythematosus, rheumatoid arthritis, or inflammatory polyarthropathy, or any combination of these), infection (selected categories of infectious and paracytic diseases), injury, paralysis of limb, and varicose veins. The reasons for assessing these characteristics included that they had been reported previously as possibly being associated with VTE 12 –16 ; information on these was available in the data source, and there were ≥30 observations of hospitalizations with the characteristic and VTE diagnosis. Diagnoses of the selected medical conditions and venous catheterization were identified using the ICD-9-CM coded information (the ICD-9-CM codes are presented in Appendix A).
The ICD-9-CM Codes Used As per the Study Definition to Identify Hospitalizations in Which a Deep Vein Thrombosis or Pulmonary Embolism Diagnosis or Both, Were Recorded.
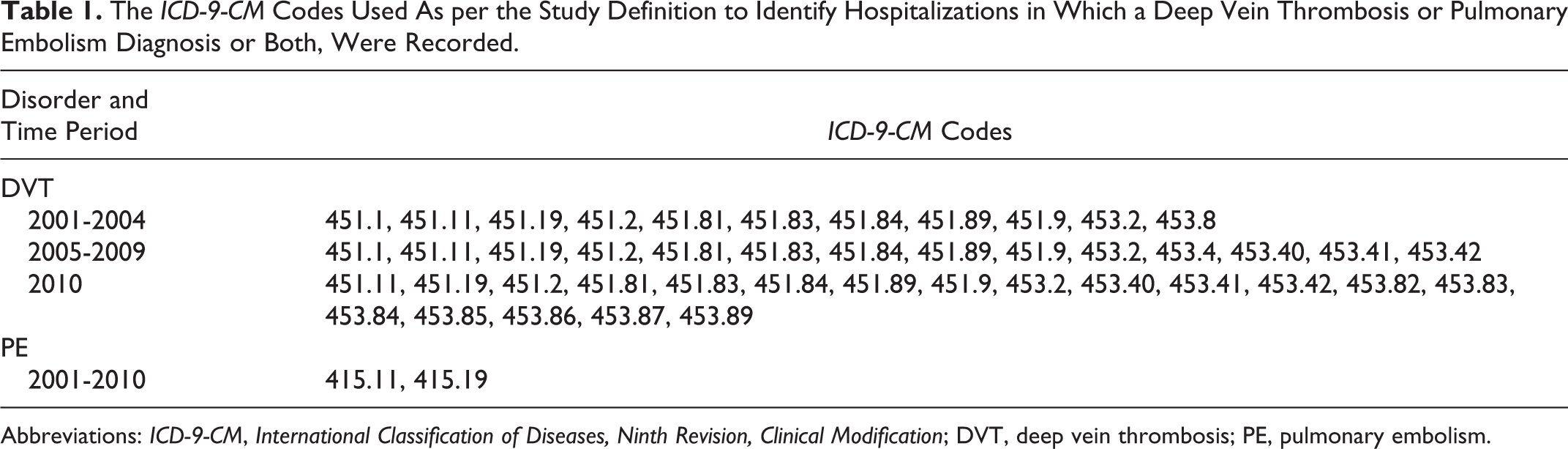
Abbreviations: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; DVT, deep vein thrombosis; PE, pulmonary embolism.
Analysis
The analysis was weighted to represent all hospitalizations of patients ≥60 years of age occurring nationally during the period 2001 to 2010 in the types of hospitals included in the NHDS survey. The estimated annual number of hospitalizations with a diagnosis of VTE was applied to the US Bureau of Census’ mid-year population estimates to derive the annual rates of such hospitalizations per 1 00 000 population ≥60 years of age. Information about the methodology used by the Census Bureau in developing population estimates can be found at the following Web site: http://www.census.gov/popest/index.html. The year-wise trend in the rate of hospitalizations in which a VTE diagnosis was recorded was assessed by linear regression modeling using the estimated annual rates as the outcome variable and year as the predictor variable. Because the set of ICD-9-CM codes used to identify DVT diagnosis in this study changed in 2005 and 2010, the year-wise trends in the rate of hospitalizations in which a VTE diagnosis was recorded was also assessed separately for the time periods 2001 to 2004 and 2005 to 2009.
The associations between hospitalizations in which a VTE diagnosis was recorded and selected patient- and hospitalization-related characteristics were assessed using combined data for the years 2001 to 2010. The frequency of hospitalizations with a recorded VTE diagnosis (per 1000 hospitalizations) was estimated by these characteristics, and the statistical significance of differences was assessed by the chi-square test. Characteristics associated with VTE, chi-square P < .05, were entered in a multiple logistic regression model to assess independent association with VTE. SAS software (release 9.3, SAS Institute, Inc., Cary, NC, USA) was used for the yearly trend analysis. The remainder of the analysis was conducted using SAS-callable SUDAAN (release 10.0.1, Research Triangle Institute, Research Triangle Park, NC, USA). The analysis was adjusted for the complex survey design when estimating variances using design variables accessed through the NCHS’s Research Data Centers.
Results
The study sample had an unweighted total of 1.137 million observations of hospitalizations among patients ≥60 years of age. Of these, 25 753 had a VTE diagnosis recorded. The estimates presented hereafter are nationally weighted estimates. The estimated yearly number of hospitalizations in which a VTE diagnosis was recorded ranged from approximately 2 70 000 (95% confidence interval [CI] 2 39 000-3 00 000) in 2001 to 4 23 000 (95% CI 3 24 000-5 22 000) in 2010. The rate of hospitalizations in which a VTE diagnosis was recorded per 1 00 000 population of all adults ≥60 years of age increased from 581 (95% CI 515-646) in 2001 to 739 (95% CI 567-912) in 2010 (Figure 1). For men ≥60 years age, this rate increased from 534 (95% CI 453-616) in 2001 to 822 (95% CI 603-1041) in 2010; for women, the increase was from 615 (95% CI 547-684) in 2001 to 673 (95% CI 520-826) in 2010.
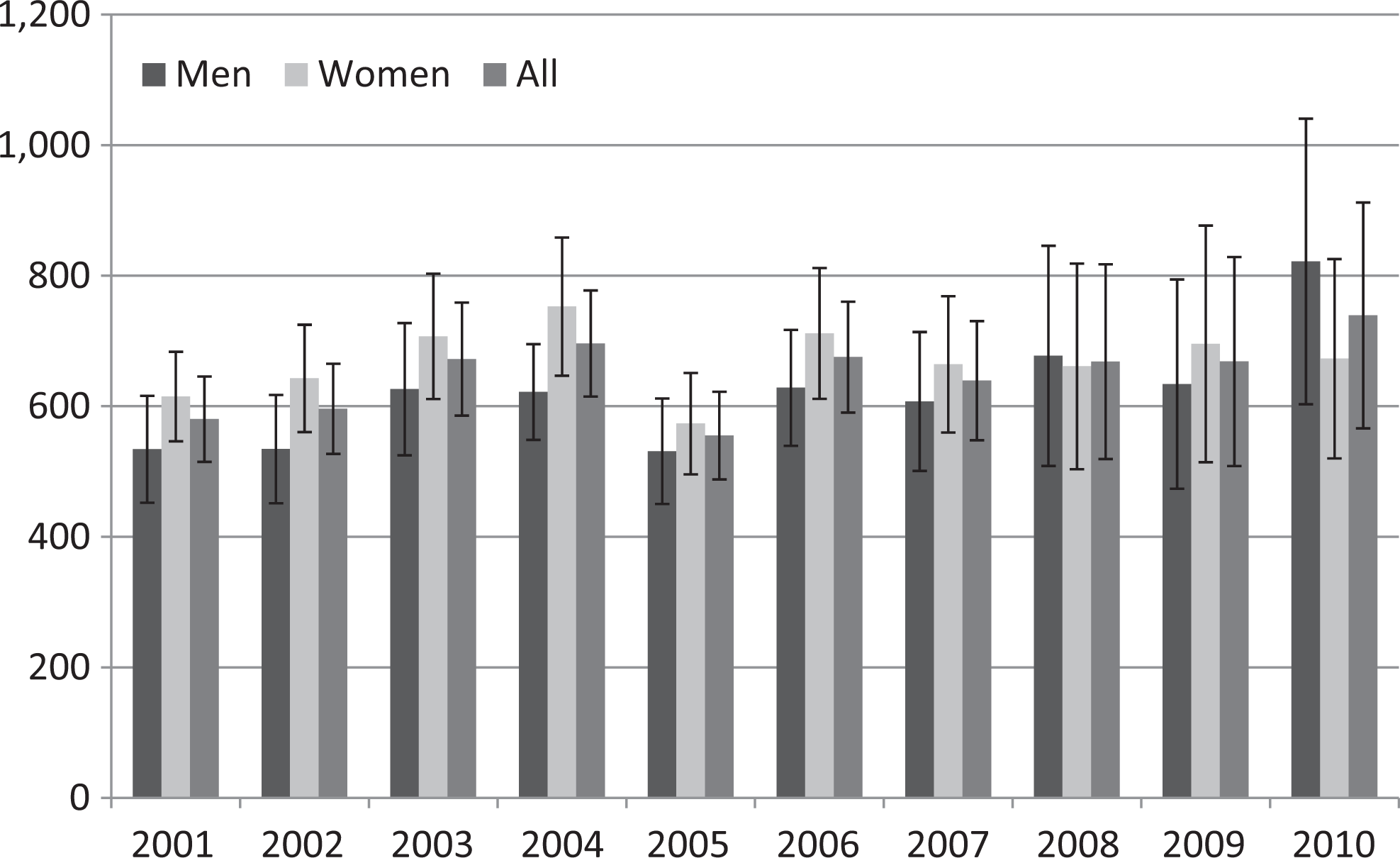
Estimated number of hospitalizations in which a diagnosis of venous thromboembolism (VTE) was recorded per 1 00 000 population ≥60 years of age, from 2001 to 2010. Note: Error bars indicate 95% confidence intervals.
During the period 2001 to 2010, there was a significant increase in the rate of hospitalizations in which a VTE discharge diagnosis was recorded per 1 00 000 for men ≥60 years of age (P = .010) and a close to significant increase in all adults ≥60 years of age (P = .064; Table 2). During the period 2001 to 2004, there was a significant increase in the rate for all adults ≥60 years age (P = .035) and women ≥60 years age (P = .010). There was no significant increase in the rate during the period 2005 to 2009.
Year-Wise Trends in the Rate of Hospitalization in Which a Venous Thromboembolism Diagnosis Was Recorded per 1 00 000 Population of Adults >60 Years of Age.
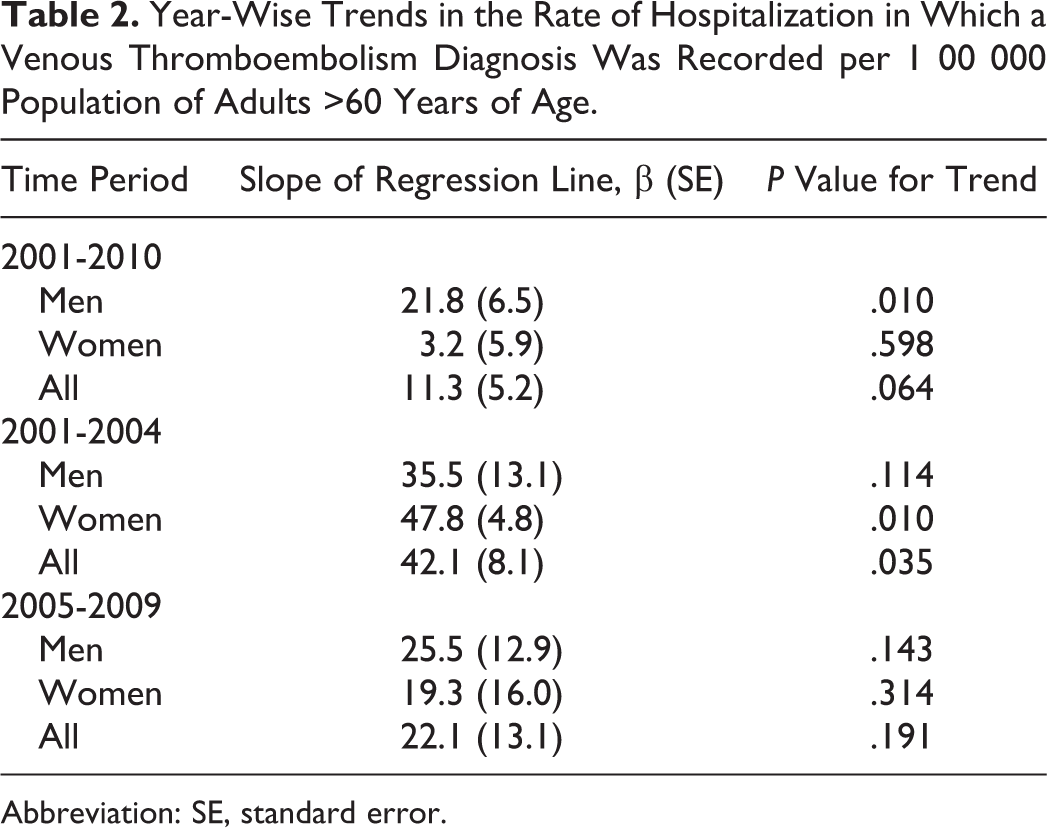
Abbreviation: SE, standard error.
The disposition in 6.6% of the hospitalizations in which a VTE diagnosis was recorded among patients ≥60 years age was that the patient died. The case fatality rate among hospitalizations with a PE (with or without a DVT) diagnosis was 9.5%; among hospitalizations with a DVT (but not a PE) diagnosis, it was 4.4%.
In bivariate analyses, the frequency of VTE diagnosis varied significantly (chi-square P < .05) by a number of the factors assessed (Table 3). Factors associated with an increased frequency of VTE diagnosis included female sex, venous catheterization, diagnosis of cancer, season (summer and autumn), and greater length of hospital stay. In multivariable analysis, factors positively associated with a VTE diagnosis were female sex (odds ratio [OR] 1.08, 95% CI 1.02-1.14), increased length of hospital stay (OR 2.42, 95% CI 2.23-2.62 for 4 to 6 days of hospital stay and OR 3.40, 95% CI 3.12-3.70 for ≥7 days), date of discharge during summer and autumn seasons (compared to spring; OR 1.08, 95% CI 1.01-1.15 and OR 1.13, 95% CI 1.05-1.21, respectively), having venous catheterization (OR 1.43, 95% CI 1.28-1.59), and diagnosis of cancer (OR 1.64, 95% CI 1.51-1.79).
Frequency of a Venous Thromboembolism (VTE) Diagnosis Recorded per 1000 Hospitalizations by Selected Patient Characteristics and Comorbidities and the Independent Association of These Characteristics With a VTE Diagnosis Being Recorded Among Hospitalizations of Adults ≥60 Years of Age, 2001 to 2010.
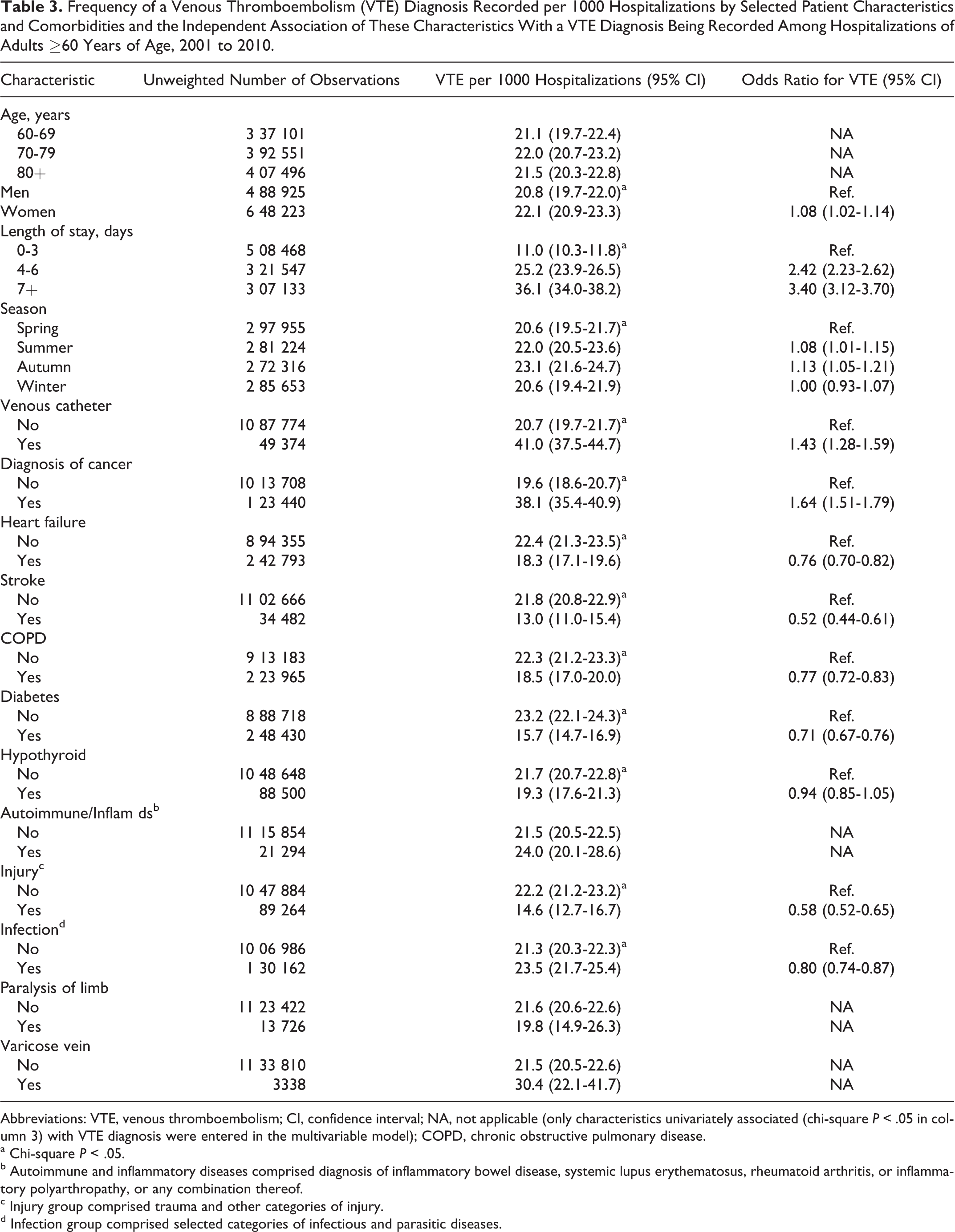
Abbreviations: VTE, venous thromboembolism; CI, confidence interval; NA, not applicable (only characteristics univariately associated (chi-square P < .05 in column 3) with VTE diagnosis were entered in the multivariable model); COPD, chronic obstructive pulmonary disease.
a Chi-square P < .05.
b Autoimmune and inflammatory diseases comprised diagnosis of inflammatory bowel disease, systemic lupus erythematosus, rheumatoid arthritis, or inflammatory polyarthropathy, or any combination thereof.
c Injury group comprised trauma and other categories of injury.
d Infection group comprised selected categories of infectious and parasitic diseases.
Discussion
It is important to assess hospitalizations with a VTE diagnosis and associated factors among older adults, because older adults are at higher risk of VTE occurrence in general. Research has well established that VTE rates are substantially higher among this group. 1 –4 Our study findings indicated that a substantial number of hospitalizations with a recorded diagnosis of VTE, as per our study definition, occurred among older adults. Rates of hospitalizations in which a VTE diagnosis was recorded increased during the period 2001 to 2004. In addition, risk factors associated with a VTE diagnosis among hospitalized older adults may include venous catheterization and selected comorbidities or conditions.
In 2010, there were an estimated 4 23 000 hospitalizations of adults ≥60 years of age with a recorded diagnosis of VTE, leading to a rate of 739 per 1 00 000 population in this age group. The findings of this study indicated that the rate of hospitalizations in which a VTE diagnosis was recorded increased during the period 2001 to 2010 among men ≥60 years of age. When trends in the rates were assessed separately for the periods 2001 to 2004 and 2005 to 2009 (because of the use of common sets of ICD-9-CM codes in this study to identify DVT during these periods), we found an increase in the rate during the period 2001 to 2004 among women ≥60 years of age, with the rates being comparatively stable for both men and women during the period 2005 to 2009.
Several factors might explain the increase in the rate of hospitalizations in which a VTE diagnosis was recorded during the period 2001 to 2004. One reason may be newer diagnostic technology, the availability, and the use of which has increased during this period. 17 –19 For example, research focusing on emergency departments during the period 1996 to 2007 reported a 5 times increase in the use of computed tomography (CT) scans among patients with chest pain and shortness of breath, both common symptoms of PE. 17 Studies have also reported increased CT use among inpatients with these kinds of symptoms. 18,19 Other factors that possibly could have contributed to an increased rate of VTE diagnosis included older average age of the general US population; possible changes in the prevalence of VTE risk factors, such as obesity; increased awareness of VTE among patients, providers, and the public in general; and better documentation of VTE.
A substantial percentage of hospitalized patients with a VTE diagnosis died during hospitalization. It is not known what percentage of the deaths among patients ≥60 years of age was attributable to a PE event. The PE-related case fatality rate among patients ≥60 years of age found in this study (9.5%) was higher than the rate reported previously among all non-newborn patients (7.1% during the period 2007-2008). 20 Research assessing case-fatality rates among hospitalized patients have found that case-fatality rates among patients with PE increase with advancing age. 21
In the current study, a number of the characteristics or comorbidities assessed were associated with an increased likelihood of a VTE diagnosis among hospitalizations of older adults. Cancer is an important risk factor for VTE. 10,14 In a study using a patient information database that included patients from 374 hospitals in the United States, the relative risks of VTE among patients aged 18 to 49, 50 to 64, and ≥65 years with cancer were 2.17, 3.64, and 4.62, respectively, compared to patients aged 18 to 49 years without cancer. 22 In another study assessing VTE risk among hospitalized patients of all ages with cancer, the investigators found that an increased risk of VTE was associated with almost all of the 19 different types of cancer studied; however, the magnitude of the increased risk varied by the type of cancer. 23 In the current study, hospitalizations of older adult patients with cancer had a substantially increased likelihood of having a recorded VTE diagnosis compared with hospitalizations of older adult patients without cancer. Our finding of the greater risk of VTE associated with venous catheterization is consistent with previous reports. 10,24
Other studies have reported a possible seasonal variation in VTE occurrence, with increased incidence during winter. 25,26 Hypotheses on why VTE risk may be higher during winter include that the risk is affected by seasonal variation in biochemical markers, including coagulation-related markers (eg, fibrinogen). 25 The findings of the current study did not indicate VTE risk to be higher during the winter with the OR being slightly higher among discharges during autumn and summer, compared to spring. Previous research has also indicated that increased length of hospital stay might be associated with a higher VTE risk. 11,21 However, VTE occurrence during hospitalization can itself increase the length of stay, and our finding could be—at least partially—because of this. In addition, it might be that the observed association is partly because longer length of stay increases the time for diagnosis of VTE. Although age group was not significantly associated with VTE diagnosis in this study, other studies have reported increased rates and incidences of VTE by increasing age categories among older adults. 3,5,8
We do not know why a number of factors, such as heart failure, stroke, and injury, that have been previously reported to be risk factors for VTE were not associated with VTE in this study and, in fact, appeared to be negatively associated with (ie, have a protective effect against) VTE. Several previous studies using hospital discharge data that included broader adult age groups have reported increased risks of VTE associated with several conditions including HIV infection, inflammatory bowel disease, hypothyroidism, diabetes mellitus, rheumatoid arthritis, nephrotic syndrome, chronic obstructive pulmonary disease, and heart failure; however, a number of studies also found that the risk of VTE associated with the respective comorbiditiy assessed tended to be lower among older age groups compared to younger adults (14, C-J). 14,27 –34 Our findings do not necessarily mean that these factors are not associated with an increased risk of VTE among hospitalized older adults. Our conjectures on possible reasons include that because of the perceived VTE risk, patients with these risk factors may have been more likely to receive VTE prevention measures, and this, at least partially, could have affected our findings. It may also be possible that these risk factors have different effects on VTE risk (for example they may increase VTE risk to a lesser extent) among the cohort older adults assessed in this study than groups assessed in some other studies.
Limitations of this study included that ICD-9-CM coded diagnoses in discharge survey data are not always accurate in identifying patients with VTE; however, research has indicated that the positive predictive values associated with many of the VTE-related ICD-9-CM codes used in this study may be between 75% and 95%. 35 It is likely that for a large proportion of the hospitalizations in which a VTE diagnosis was recorded, the VTE occurred prior to hospitalization. 9,10 However, because of unavailability of adequate information, this study did not distinguish these separately. Because of the unavailability of information, this study could not assess other possible risk factors for VTE, such as smoking or recent hospitalization, or the risk of VTE associated with specific types of venous catheterization.
The administration of VTE prophylaxis during or before hospitalization would have reduced the risk of VTE and, thus, could have affected the findings of this study; however, because we did not have information on whether or not the patients received VTE prophylaxis, we do not know to what extent this may have occurred. It is possible that in recent years, more patients with VTE were treated in the outpatient setting than before, which could have affected our findings related to trends in hospitalizations with a VTE diagnosis. However, we do not know to what extent this may have occurred. In addition, findings related to the trends in the rates of hospitalizations during the period 2001 to 2010 should be interpreted in the context of the changes in the ICD-9-CM codes used to define VTE over the study period. We do not know to what extent the changes ICD-9-CM codes we used affected the findings of lower point estimates of rates of VTE diagnosis in 2005 (the beginning of a period with new codes) compared to 2004 (the end of the period with older codes). However, there were no changes in the codes used for the years 2001 to 2004 and 2005 to 2009 time periods.
Many episodes of VTE could possibly be prevented through the use of pharmacological prophylaxis and other strategies. 36,37 Possible adverse events from anticoagulants include bleeding, the risk of which has been reported to be higher among older adults compared with those who are younger. 38,39 Such bleeding complications could include serious events such as hemorrhagic stroke and other life-threatening events. Clinical considerations related to VTE prophylaxis include the benefits and risks of anticoagulants and other measures. The VTE prevention guidelines from professional bodies can help guide VTE prophylaxis decisions. Increased knowledge and understanding of VTE occurrence among older adults is also needed. In this context, the findings of this study can help to increase awareness of VTE and improve understanding of its effects, time trends, and risk factors among hospitalized older adults. Improved implementation of VTE prevention strategies as appropriate may help to reduce VTE occurrence and improve patient outcomes.
Footnotes
Appendix A
International Classification of Disease, 9th Revision, Clinical Modification codes used for identifying hospitalizations with diagnoses of selected medical conditions (diagnosis codes) and venous catheterization (procedure code) Cancer: 140.xx-208.xx, 209.0x-209.3x Heart failure: 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, 428.xx Stroke: 431, 434.xx, 436 COPD: 491.2x, 492.x, 493.2x, 496 Diabetes: 250.xx Hypothyroid: 244.x Autoimmune/inflammatory diseases: 555.x, 556.x, 710.0, 714.xx Injury: 800.xx-908.xx, 910.xx-959.xx, E800.x-E848.x, E880.x-E929.x, E950.x-E999.x Infection: 001.xx-139.xx Paralysis of limb: 342.xx, 344, 344.0x, 344.1, 344.2, 344.3x, 344.5 Varicose vein: 454.x, 456.xx Venous catheterization: 38.93
Acknowledgments
The authors thank Ajay Yesupriya, MPH, at the Research Data Center, National Center for Health Statistics, Centers for Disease Control and Prevention, for his help with accessing the restricted data for this project.
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official policy of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.