
Abstract
Objectives:
The American College of Chest Physicians recommends anticoagulant therapy for at least 3 months in children hospitalized for venous thromboembolism. The objectives of the study were to evaluate the medication utilization patterns and predictors of adherence to anticoagulant therapy in pediatric population.
Methods:
Texas Medicaid medical and prescription claims from September 1, 2007 to December 12, 2012 were extracted for children (<18 years) hospitalized for pulmonary embolism (PE) or deep vein thrombosis (DVT). The index date was defined as the date of the first prescription of an anticoagulant given within 14 days of discharge. Proportion of days covered (≥80% vs <80%) was used to assess adherence to anticoagulants while controlling for demographics, cause of hospitalization, history of nonsteroidal anti-inflammatory drug use, anticoagulant use, malignancy, drug type, and Charlson comorbidity index (CCI).
Key Findings:
The patients (n = 60) had a mean (± standard deviation [SD]) age of 14.2 (±4.8) years, were primarily female (56.7%), African American (55.0%), enoxaparin users (58.3%), and had a mean (±SD) CCI of 18.3 (±37.7). The mean (±SD) adherence rates for warfarin and enoxaparin were 85.5% (±22.7%) and 78.7% (±27.8%), respectively. Overall, 66.7% were adherent (≥80%) to anticoagulant therapy. Logistic regression showed that increasing age was significantly associated with adherence to anticoagulant therapy, after controlling for other covariates (odds ratio = 1.5, 95% confidence interval = 1.13-1.85).
Conclusion:
Nearly one-third of the pediatric patients on anticoagulant therapy after discharge from PE or DVT were still nonadherent. Further research is needed to highlight the factors responsible for nonadherence in pediatric patients.
Keywords
Introduction
Pulmonary embolism (PE) and deep vein thrombosis (DVT), collectively known as venous thromboembolism (VTE), have been on a constant rise in the past 2 decades. 1 –4 The rate of VTE among hospitalized children less than 18 years of age in the United States has increased from 34 to 58 hospital admissions per 10,000 patients from 2001 to 2007, a 70% increase in 6 years. 2
According to a report published by the surgeon general, VTEs are responsible for nearly 100,000 deaths each year, across population of all ages. However, most of the VTEs are often undiagnosed and the actual mortality is predicted to be higher. 4 The surgeon general’s office estimated that the actual number of deaths attributable to PE alone could be 82,800 cases (based on 2009 estimates). 5 In addition, recurrence is a major issue in patients with VTE. Patients who have their first episode of VTE are at an increased risk of a second VTE episode. Previous studies show that nearly 30% of the patients diagnosed with VTE will more likely have a recurrent episode in the next 10 years. 6 –9 In some cases, VTE could also lead to chronic venous insufficiency (CVI), also known as the post-thrombotic syndrome. Nearly 30% of the patients diagnosed with VTE will have CVI either immediately or within 10 to 20 years of their first VTE diagnosis. 8,10,11 Thus, controlling VTE, especially in pediatric patients, is important, given that early intervention may be associated with better treatment outcomes.
Overall, VTE imposes a significant burden on mortality, morbidity, and normal development of children, which makes therapeutic and prophylactic treatment of VTE a priority. 12 –14 Anticoagulants, such as warfarin and heparin, are the treatment of choice for patients hospitalized for VTE. 5 However, nearly half of the medications for VTE used in the pediatric patients are off-label and are prescribed based on the therapeutic regimen in adults. 15 Additionally, children have a different hemostatic system and different dose requirements, making it difficult to administer the medications effectively. 12 Thus, more recently, emphasis is being placed on prophylactic treatment of patients with a first episode of VTE in order to lower the likelihood of future events.
The American College of Chest Physicians (ACCP) Evidence-Based Clinical Practice Guidelines (eigth edition) recommend anticoagulant therapy for at least 3 months in neonates and children with initial VTE. 16 There is scant real-world evidence on the adherence to anticoagulants among pediatric patients. Several studies on adult patients have reported poor adherence to antithrombotic management guidelines. 17 –21 A study by Peng et al. is the only study among hospitalized pediatric patients which assessed the compliance to ACCP guidelines. This prospective chart audit including inpatient units at the Royal Children’s Hospital, Melbourne, Australia, evaluated the grading recommendations given by ACCP to measure compliant administrations. The study reported that only half of the antithrombotic administrations were completely adherent to the dosing recommendations given by the ACCP. 22 About a half of the administrations were not given for appropriate indications per the ACCP guidelines.
Thus, there is a paucity of data assessing the adherence to anticoagulant therapy guidelines in a pediatric population hospitalized for VTE. The objectives of the study are to evaluate the medication, demographic, and clinical factors associated with adherence to anticoagulant therapy guidelines in children hospitalized for PE or DVT using the Texas Medicaid data set.
Methods
The study used individual patient-level claims from September 1, 2007, to December 31, 2012, from the Texas Medicaid medical and prescription claims database. The study was approved by the Institutional Review Board of the University of Texas at Austin.
Inclusion and Exclusion Criteria
Patients included in the study were (1) <18 years of age at index date; (2) hospitalized for PE (International Classification of Disease Clinically Modified Version 9 [ICD-9] code = 415.xx) or DVT (ICD-9 code = 451.xx, 453.xx) and discharged between December 1, 2007, and September 31, 2012; (3) had continuous Texas Medicaid enrollment 3 months before and after the index date; (4) did not have air embolism (ICD-9 code = 958.0) or fat embolism (ICD-9 code = 958.1) as a cause of index hospitalization; (5) were not hospitalized for bleeding (ICD-9 code = 459.0) or coagulation disorder (ICD-9 code = 286.0) within 90 days of discharge; and (6) did not have a history of atrial fibrillation (ICD-9 code = 427.31) in the pre-index period. The index date was defined as the date of the first prescription of an anticoagulant (Enoxaparin and/or Warfarin identified based on AHFS codes) taken within 14 days of discharge from hospitalization with a primary diagnosis of PE or DVT.
Study Measures
Medication adherence was used as the proxy measure to assess adherence to guidelines, since the guidelines state that anticoagulants should be taken for at least 3 months after the initial VTE episode. In case of conditions such as VTE that require frequent monitoring of doses, medication adherence can be used to understand adherence to guideline recommendations. Previous studies by Chen et al. and Melfi et al. used medication adherence as a proxy to guideline adherence. 19,23 Medication adherence was assessed using the proportion of days covered (PDC) method. The PDC method counts each day within the study period to determine whether a patient was in possession of the dispensed study drugs based on the initial prescription fill dates and the days’ supply. A temporary dichotomous variable assigned a value of 1 or 0 to indicate the presence or absence of the study drugs for each study day. The PDC was measured by dividing the total days of supply of dispensed medication by the number of days of follow-up. 23 Based on literature, a cutoff of 80% was used to assess adherence to anticoagulant therapy. 23
The study assessed the association of demographic characteristics such as age, gender (male or female), African American (yes or no), and clinical characteristics such as type of medication (warfarin or enoxaparin), cause of index hospitalization (DVT or PE), history of anticoagulant use (yes or no), history of nonsteroidal anti-inflammatory drug (NSAID) use (yes or no), history of fall (yes or no), history of malignancy (yes or no), and comorbidity measure as predictors of adherence to anticoagulant therapy. The history of NSAID use and history of falls measured the contraindication to anticoagulant therapy, and history of malignancy measured the risk factor during pre-index period. The Dartmouth-Manitoba version of Charlson comorbidity index (CCI) score was used to measure the comorbidity burden. 24 The CCI comprises the sum of the weights of the comorbidities, which include myocardial infarction, congestive heart failure, peripheral vascular disease, dementia, cerebrovascular disease, chronic pulmonary disease, connective tissue disease, ulcer disease, mild liver disease, and diabetes, each with a weight of 1; hemiplegia, moderate or severe renal disease, any tumor, leukemia, and lymphoma with a weight of 2; moderate or severe liver disease with a weight of 3; and metastatic tumor with a weight of 6. Although, CCI is not directly applicable to the pediatric population, controlling for CCI score as a confounding variable is important because the comorbidity burden in patients with VTE is high and should be accounted for in the study model. 25 –27
Statistical Analyses
Descriptive statistics consisting of means, standard deviations (SDs), frequencies, and percentages were reported for the demographic and clinical characteristics. A logistic regression analysis was used to estimate the likelihood of adherence (PDC ≥ 80% vs <80%) to anticoagulant therapy while controlling for the confounders. All statistical analyses were conducted using SAS version 9.3 (SAS Institute Inc, Cary, North Carolina) with an a priori significance level of P < .05.
Results
A total of 94 patients met the study inclusion criteria and were identified with PE or DVT as their index hospitalization in the Texas Medicaid data set. Of these, 29.8% (n = 28) patients were without a prescription of an anticoagulant agent within 14 days of their discharge and were excluded. Patients (n = 6) with missing values on any of the covariates were excluded. The remaining 60 patients were included in the final study cohort. Of the total patient population included in the study, majority of the patients were female (n = 34, 56.7%), African American (n = 33, 55.0%), were on enoxaparin (n = 35, 58.3%), and had DVT as their index hospitalization (n = 43, 71.7%). In the case of clinical characteristics, majority of the patients had no history of NSAID use (n = 46, 76.7%), had no history of anticoagulant use (n = 46, 76.7%), and no history of malignancy (n = 52, 86.7%; Table 1). There were no patients with a history of fall in the study period.
Demographic and Clinical Characteristics of Patients With Venous Thromboembolism.
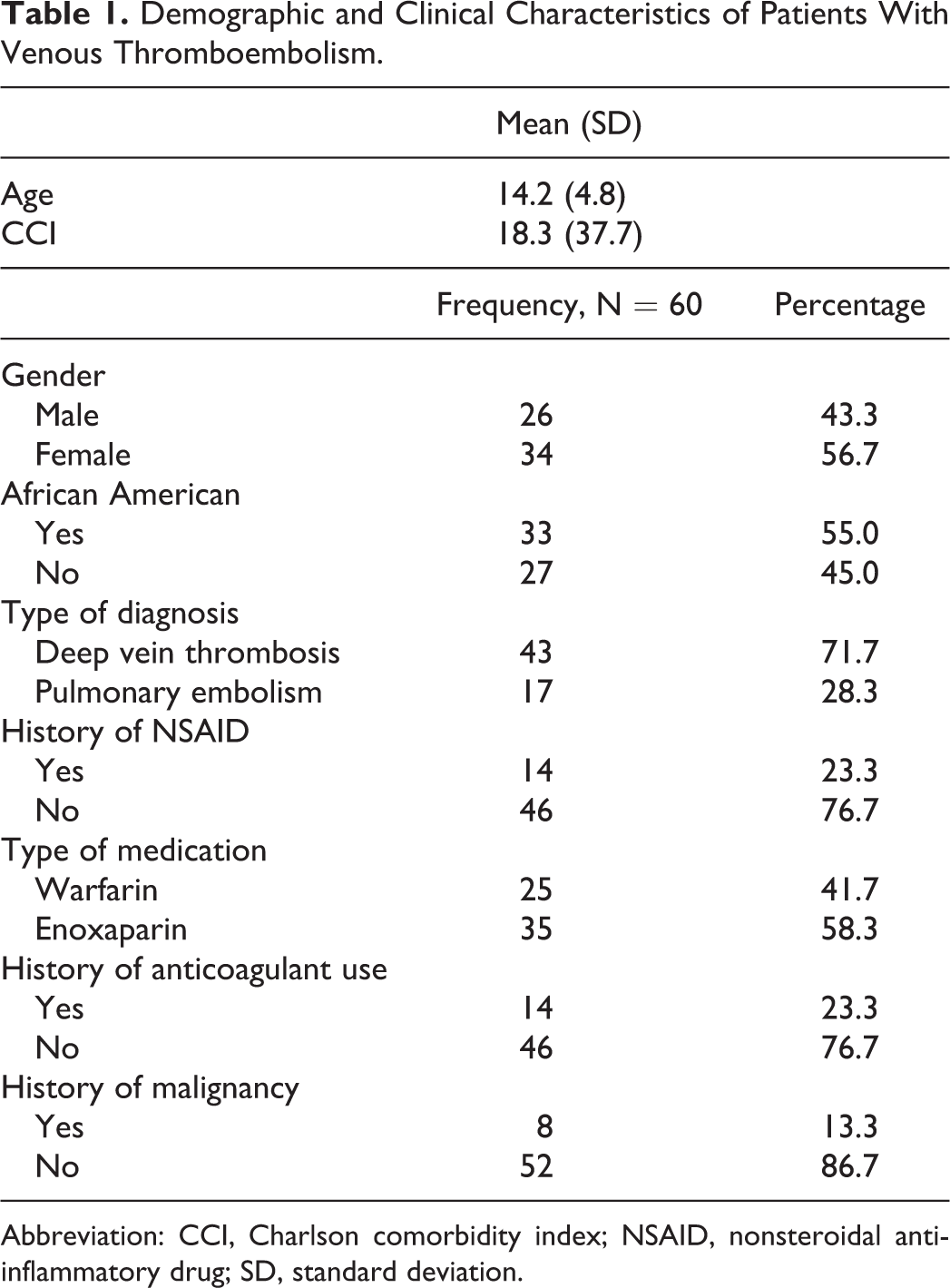
Abbreviation: CCI, Charlson comorbidity index; NSAID, nonsteroidal anti-inflammatory drug; SD, standard deviation.
The calculated mean (±SD) adherence rates for warfarin and enoxaparin were 85.5% (± 22.7%) and 78.7% (± 27.8%), respectively. In all, 66.7% of the patients were adherent (PDC ≥ 80%) to anticoagulant therapy. Multivariate logistic regression showed that increasing age was significantly associated with adherence to anticoagulant therapy (odds ratio = 1.45, 95% confidence interval = 1.13-1.85; Table 2).
Predictors of Adherence to Anticoagulant Therapy in Patients With Venous Thromboembolism.a
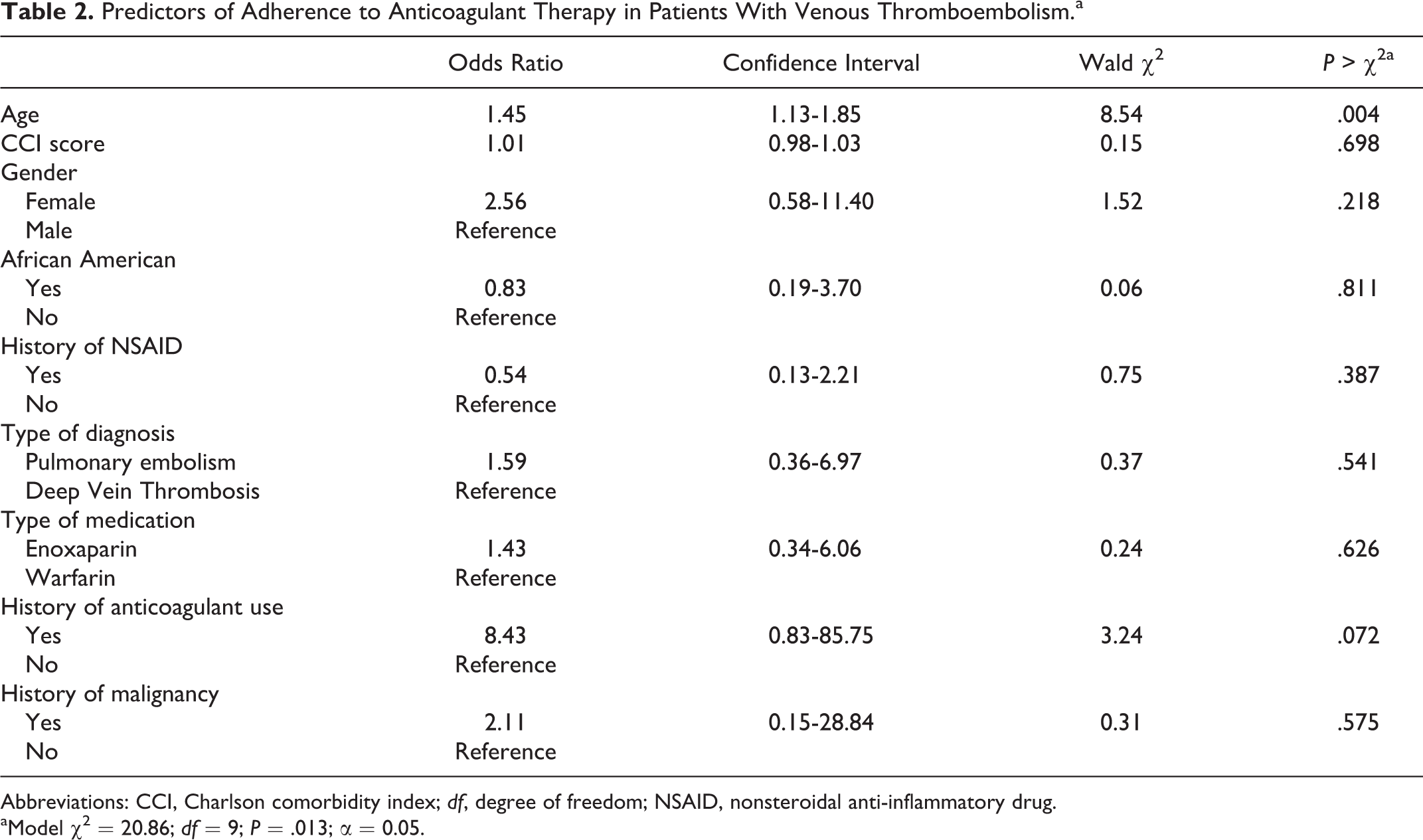
Abbreviations: CCI, Charlson comorbidity index; df, degree of freedom; NSAID, nonsteroidal anti-inflammatory drug.
aModel χ2 = 20.86; df = 9; P = .013; α = 0.05.
Discussion
The primary objective of this study was to determine the adherence to evidence-based treatment guidelines in pediatric patients hospitalized for PE or DVT. The current study estimated that 70.2% of the pediatric patients were prescribed an oral or injectable anticoagulant medication within 14 days of their discharge.
In the present study, two-third of the patients prescribed an anticoagulant within 14 days of discharge were adherent (PDC ≥ 80%) to anticoagulant therapy for 3 months. The low anticoagulant adherence in the pediatric patients with VTE may be attributed to multiple factors. First, most of the drugs used in the pediatric patients with VTE are administered off-label. Thus, administration of anticoagulants in the pediatric population is strictly based on evidence recommendations and clinical judgment. 28 Majority of VTE prophylaxis recommendations within pediatric ACCP guidelines are “weak” recommendations, which suggest physicians’ lack of confidence in the evidence recommendations. Future studies assessing the long-term benefits of VTE prophylaxis in the pediatric population may be needed to strengthen the existing evidence-based guidelines. 16,22 Second, the pediatric population differs from adults in terms of their pharmacokinetic and pharmacologic profile, making it challenging for the physician to start therapy in pediatric patients. 12 In addition, administration of anticoagulants in the pediatric patients requires careful dose monitoring. 29 Third, increasing age of the patient could affect a patient’s ability to comprehend the benefits of the treatment, thus leading to a better compliance rate. 15 The current study showed that none of the demographic characteristics or clinical factors, except age, were found to be significant predictors of adherence to anticoagulant therapy. The study showed that increasing age led to better adherence in these patients. As the administration of medications in pediatrics is usually by the caregiver, the level of understanding of the caregivers may have an impact on medication adherence. 30 Also, dose adjustments may be required on an individual basis, per the guideline. Fourth, evidence-based guidelines recommend that pediatric patients with life-threatening conditions should not be started on anticoagulant therapy. A study by Shetty et al. using Kid’s Inpatient Dataset reported that majority (76.2%) of patients diagnosed with VTE had at least one chronic illness and/or life-threatening condition, thus patient factors should be assessed before starting administration of anticoagulants in the population. 4 Physicians also have to be aware of the dietary modifications and adequate vitamin K level requirements in pediatrics. Future studies evaluating alternative antithrombotic management options in the real world are also required.
Nearly one-third of the entire cohort was nonadherent to anticoagulant therapy, who may also be at a higher risk of recurrence. Previous studies have estimated the recurrence rate of VTE from 10% to 15% in the pediatric population. 17 Also, the cost attributable to a recurrent episode of VTE in the pediatric population is estimated at US$20,000. 17 Thus, reducing recurrence rates is also vital from a financial standpoint.
One of the primary limitations of the study was that it included patients in Texas Medicaid data set only, which may limit the generalizability of the study to other settings. Although the incidence of VTE in pediatric patients has increased in the recent past, it is still largely a rare condition with an incidence rate of 18.5 cases per 10,000 pediatric admissions. 4 Irrespective of the small sample size, this study provides valuable insights into the treatment of VTE in children. Also, we only included factors available in the data set and could not control for factors clinically relevant to patients with VTE. Additionally, dose titrations based on international normalized ratio values are especially important in patients with VTE and are an integral part of their therapy. This variability introduced by clinical parameters could not be accounted in the study, as clinical markers and laboratory values are seldom included in claims database.
Conclusion
In conclusion, this study indicates that VTE in pediatric patients, although a rare condition, is still prevalent. Evidence-based treatment guidelines for these patients are outlined, however, nearly one-third of the patients are still nonadherent to prophylactic anticoagulant therapy. Given that hospitalized patients are at an increased risk of recurrence of VTE, it is crucial to understand their treatment patterns. Future research exploring the factors associated with lower adherence rates for children diagnosed with VTE are needed.
Footnotes
Authors’ Notes
Rakesh R. Singh and Komal R. Gupte-Singh had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Rakesh R. Singh is responsible for research conceptualization, data collection, analysis, result interpretation, and writing of manuscript. Komal R. Gupte-Singh is responsible for research conceptualization, result interpretation, and writing of manuscript. James P. Wilson and Brady S. Moffett are responsible for research conceptualization and review of manuscript. The research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors for the purpose of this research.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: James P. Wilson received grant from Novartis pharmaceuticals, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.