
Abstract
Hospitalized medical patients are at risk of deep-vein thrombosis (DVT) and pulmonary embolism (PE). We evaluated inpatient and postdischarge DVT/PE and thromboprophylaxis rates in US medical patients, using patient admissions from January 2005 to November 2007 in the Premier Perspective™-i3 Pharma Informatics database. Among 15 721 patients with cancer, congestive heart failure, severe lung disease, and infectious disease, 39.0% received inpatient thromboprophylaxis, with the highest rate in patients with cancer (51.9%). In all, 3.4% received outpatient pharmacological prophylaxis. Mean ± SD prophylaxis duration was 2.2 ± 5.7 days. Overall, 3.0% of inpatients had symptomatic DVT/PE, and an additional 1.1% of patients were rehospitalized for DVT/PE or treated in the outpatient setting. Patients with infectious disease had the highest rate of DVT/PE (4.6%). Inpatient DVT/PE and prophylaxis rates of the different medical conditions had a negative correlation (R 2 = 0.72). This analysis demonstrates the burden of DVT/PE and highlights the underuse of thromboprophylaxis across the continuum of care.
Keywords
Introduction
In addition to the well-recognized high risk of deep-vein thrombosis (DVT) among surgical patients, hospitalized medical patients are also at substantial risk, with DVT prevalence estimated to be 10% to 20% in general medical patients without thromboprophylaxis. 1 In a population-based case-control study, hospitalization for medical illness accounted for 22% of all cases of DVT and pulmonary embolism (PE) recorded, and this was a similar proportion to that attributed to hospitalization for surgery (24%). 2 A recent large real-world study by Spyropoulos et al. 3 assessed DVT/PE rates in patients with different medical conditions. The total average DVT/PE incidence was 5.6%, with cancer patients having the highest DVT/PE incidence (7.6%), followed by congestive heart failure (5.6%), severe lung disease (5.0%), and severe infectious disease (4.9%). 3 Of those medical patients who developed a venous thromboembolic event, over a quarter were at risk of developing PE. Interestingly in this study, the median time to a DVT/PE event was 74 days, 3 suggesting that a substantial proportion of events occurred in the outpatient setting, 3 confirming the results observed in a study by Spencer et al. 4
To reduce the risk of DVT, current evidence-based guidelines from the American College of Chest Physicians (ACCP) recommend that acutely ill medical patients admitted to hospital with congestive heart failure or severe respiratory disease or those who are confined to bed and have 1 or more additional risk factors (including active cancer, previous venous thromboembolism, sepsis, acute neurological disease, or inflammatory bowel disease) receive pharmacological prophylaxis with either a low-molecular-weight heparin (LMWH), low-dose unfractionated heparin (UFH), or fondaparinux (Grade 1A). 1 American College of Chest Physicians guidelines provide no recommendations for the optimum duration of DVT prophylaxis in medically ill patients; however, standard regimens of 6 to 14 days have been found to be effective in clinical trials.5–7 The length of hospital stay has been declining in the United States in recent years, 8 and patients are often discharged from hospital before their baseline mobility level has returned. In this environment, only providing inpatient DVT prophylaxis will not reach 6 to 14 days of prophylaxis.
Despite the availability of thromboprophylaxis, several real-world studies have reported that DVT prophylaxis practices are currently suboptimal in medical patients. A large proportion of patients are not receiving any form of prophylaxis or receiving thromboprophylaxis that is inappropriate in terms of dose, duration, and/or type.3,9–13 In a recent US study that included over 200 000 medical patients, a third of at-risk medical patients did not receive any form of DVT prophylaxis during hospitalization, and only 12.7% of patients received appropriate prophylaxis (ie, applying recommendations from the ACCP guidelines). 11 Currently, required reporting of DVT-related performance measures is limited to all surgical procedures under the Surgical Care Improvement Program and reduced Centers for Medicare and Medicaid Services payments for DVT/PE events as a hospital-acquired condition in orthopedic surgical patients. 14 However, the National Quality Forum-endorsed core performance measure set for the prevention of DVT from The Joint Commission includes all hospitalized patients, including medical patients. 15
To gain a greater understanding of the current clinical burden associated with DVT and PE, and the extent of the improvements needed in prevention practices, further investigations are required regarding DVT prophylaxis prescribing patterns, and DVT/PE rates in hospital and in the outpatient setting, where fewer data exist. The transition of DVT preventative care from inpatient to outpatient has been underexposed in studies and is an issue that will be addressed in this study. The objective of this analysis was to evaluate rates of symptomatic DVT/PE events and provision of prophylaxis for DVT, across the continuum of care in a large population of US medical patients.
Methods
Data were extracted from Premier Perspective™-i3 Pharma Informatics-linked database, a large de-identified US hospital drug-utilization and financial database. Claims data drawn from a large national health plan were cross-matched on the individual patient level for both in-hospital and postdischarge records. Discharge records were included in the analysis if patients met the following criteria: index hospitalization between January 2005 and November 2007; age ≥18 years at the time of their index hospitalization; and ≥6 months of continuous plan enrolment prior to the index hospitalization. In addition, patients had to be hospitalized for specified medical conditions associated with DVT risk, and eligible patient records were identified using codes from the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The medical conditions included were: cancer (malignant neoplasms or carcinoma in situ, excluding central venous catheter procedures); congestive heart failure (heart failure, hypertensive heart disease with heart failure, and rheumatic heart failure); severe lung disease or chronic obstructive pulmonary disease (COPD; pneumocystosis, acute bronchitis and bronchiolitis, pneumonia, COPD and allied conditions, pneumoconioses and other lung diseases due to external agents, other lung diseases, and tracheostomy complications); and infectious disease (infectious and parasitic diseases [except pneumocystosis], skin infections, chronic infection, and postoperative infection). Patients were excluded if they were discharged or transferred to an acute-care facility, had length of hospital stay of 0 or >30 days, or if they were diagnosed with atrial fibrillation.
Inpatient use of mechanical and/or pharmacological DVT prophylaxis was captured via charge codes during hospitalization. Outpatient pharmacological prophylaxis was assessed as prescriptions during the 14 days prior to index admission and the 14 days following index discharge; outpatient pharmacological prophylaxis was allowed to be initiated up to 14 days before the index admission to reflect that some patients might have received their anticoagulation prescriptions prior to prescheduled hospitalizations. Inpatient and outpatient pharmacological prophylaxis was identified via charge codes or pharmacy claims for the following medications: UFH; an LMWH (enoxaparin, dalteparin, or tinzaparin); and fondaparinux. For outpatient prophylaxis, warfarin charge codes were also included. Pharmacological agents were considered prophylactic if they were used at prophylaxis dosages and prior to any DVT/PE event. Mechanical prophylaxis was identified via charge codes for graduated compression stockings and charge codes indicating use of intermittent pneumatic compression devices and/or venous foot pumps. Rates of combination prophylaxis were also analyzed, which was defined as use of more than one product/type of prophylaxis across the entire duration of the hospitalization or in the outpatient setting. The presence or absence of prophylaxis, and the type used, were calculated descriptively for the medical conditions overall and for each condition separately. The mean ± SD length of hospital stay and the duration of inpatient and outpatient prophylaxis were also calculated for all patients; the prophylaxis duration was included as 0 for patients receiving no prophylaxis.
For analysis of rates of symptomatic DVT/PE events, patients were followed up to 30 days following index discharge and were censored administratively in December 2007 or at plan disenrolment, whichever occurred first. The DVT/PE events were defined as the first diagnosis according to ICD-9-CM codes and were categorized as: index events (primary or secondary diagnosis during the index admission); readmission events (primary or secondary diagnosis during a hospital admission following the index hospitalization); or outpatient events (diagnosis in an outpatient setting accompanied by anticoagulant treatment within 14 days of diagnosis). The correlative relationship between DVT/PE event rates and prophylaxis rate or duration for the different medical conditions was also analyzed.
Results
A total of 15 721 medical patients were included in the analysis (Figure 1 ); 5488 patients (34.9%) were diagnosed with infectious disease, 5141 (32.7%) with severe lung disease, 3759 (23.9%) with cancer, and 1333 (8.5%) with congestive heart failure. Overall, the mean age was 54.0 years (Table 1 ). The majority of patients were white (69.4%), commercially insured (93.7%), and treated in urban hospitals (93.5%).
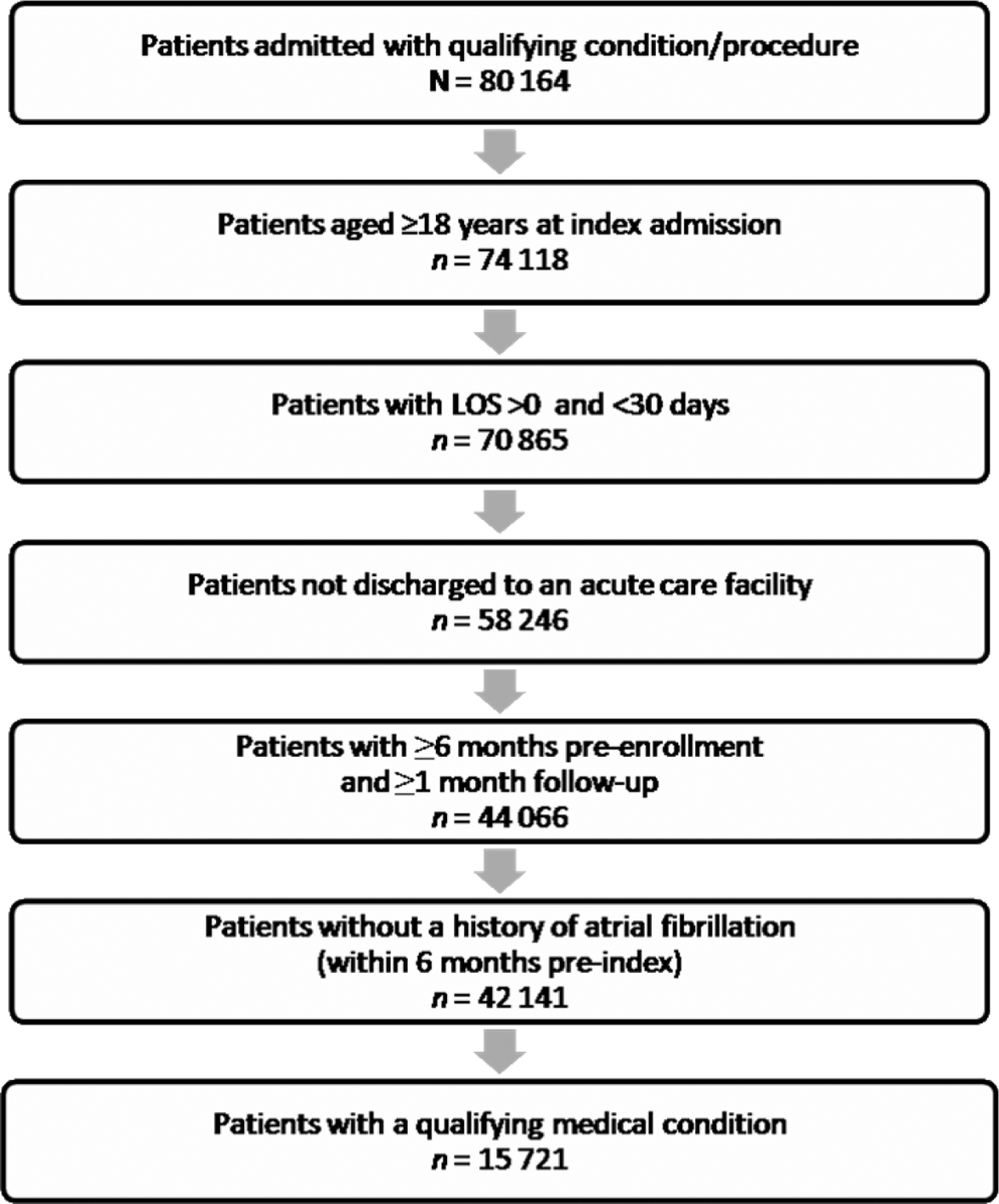
Flow diagram of patient inclusions. LOS indicates length of stay.
Summary of Patient Demographics and Characteristics
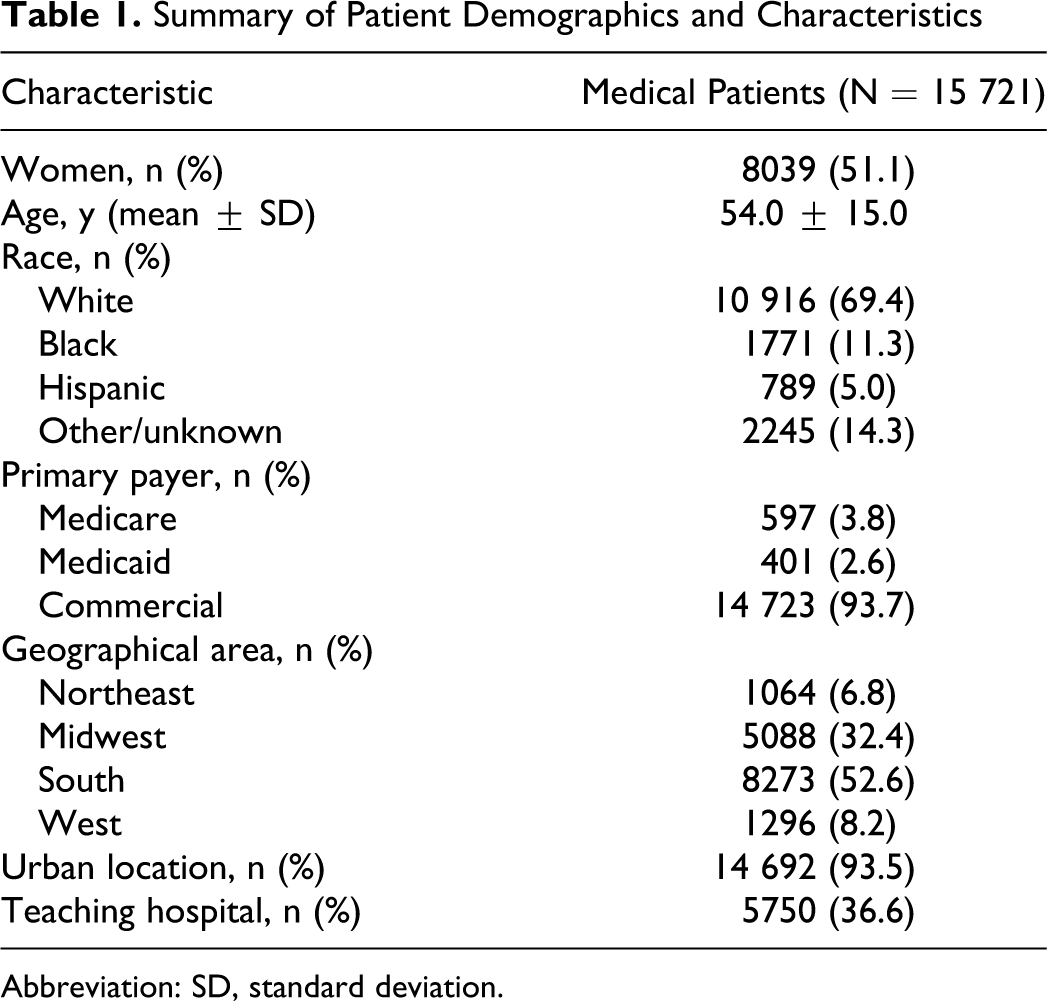
Abbreviation: SD, standard deviation.
Less than half of all the medical patients analyzed received DVT prophylaxis, with 39.0% of patients receiving any pharmacological or mechanical prophylaxis during their index hospitalization. The highest inpatient prophylaxis rate was in patients with cancer (51.9%) and the lowest was in patients with infectious disease (31.1%; Figure 2 ). The LMWH, enoxaparin, was the most commonly used form of DVT prophylaxis in patients with congestive heart failure (21.3%), infectious disease (16.3%), and severe lung disease (24.6%; Table 2 ). In patients with cancer, mechanical prophylaxis was the most frequently used method overall (40.0%), and UFH was the most commonly used pharmacological prophylactic agent (13.8%). Few medical patients in the analysis received fondaparinux (n = 25) or LMWHs other than enoxaparin (n = 42).
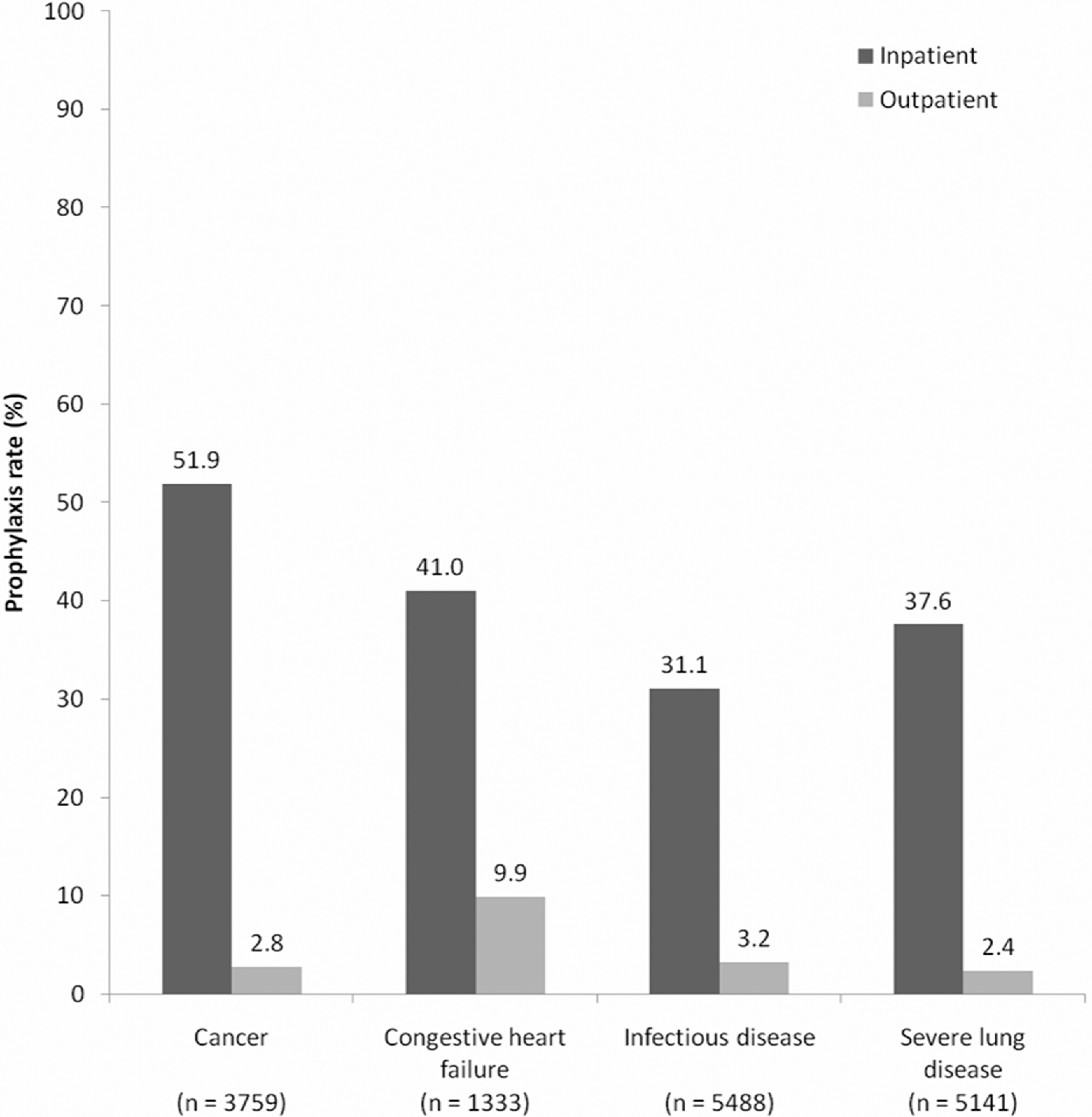
Rates of any prophylaxis received during the index hospitalization and in the outpatient setting (14 days postdischarge).
Deep-vein thrombosis Prophylaxis Type During Hospitalization and in the Outpatient Setting (14 Days Postdischarge)
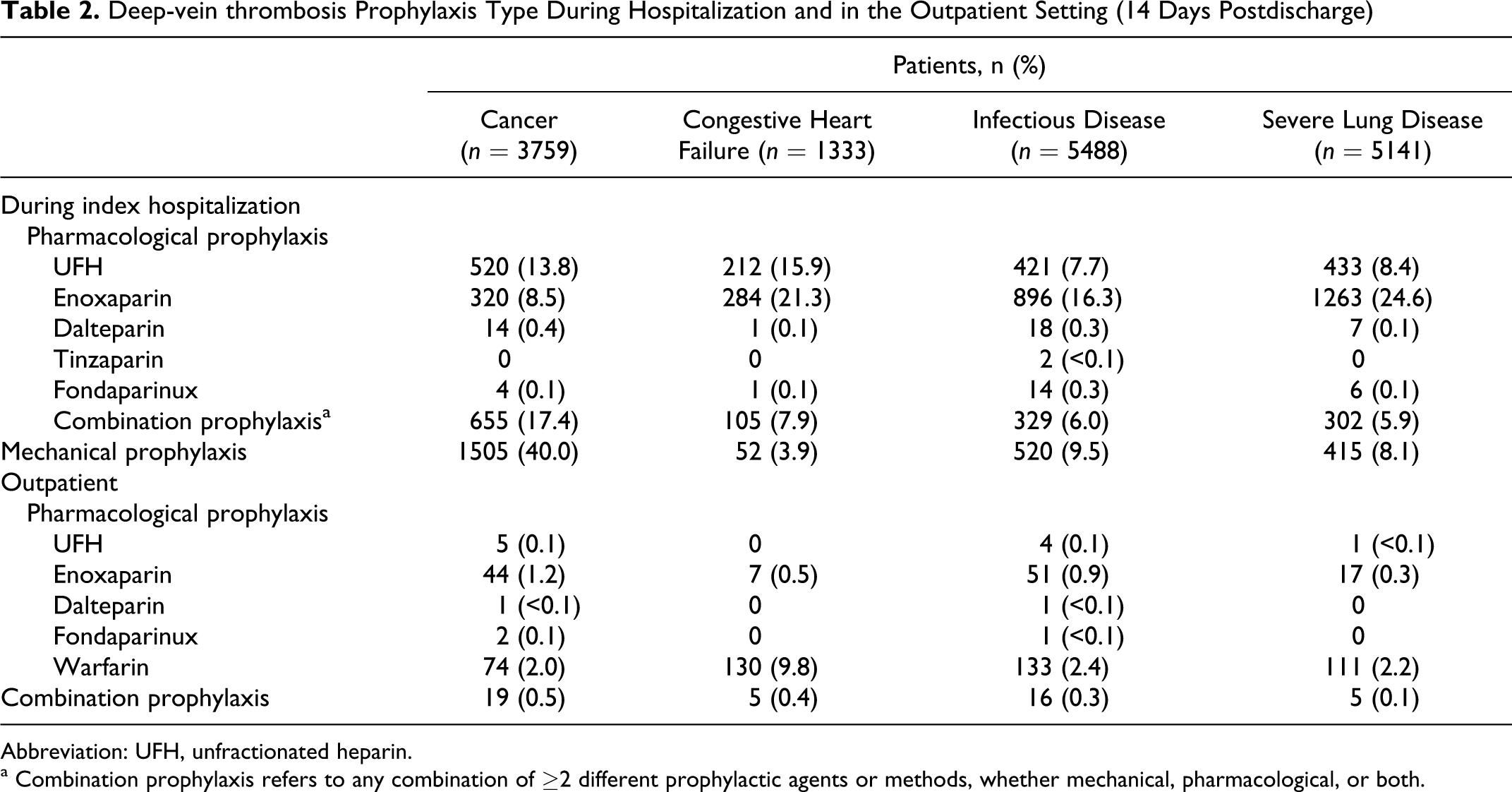
Abbreviation: UFH, unfractionated heparin.
a Combination prophylaxis refers to any combination of ≥2 different prophylactic agents or methods, whether mechanical, pharmacological, or both.
When outpatient prophylaxis was assessed, 3.4% of medical patients received any prophylaxis in the 14-day postdischarge period, ranging from 9.9% in patients with congestive heart failure to 2.4% in patients with severe lung disease (Figure 2). Warfarin was the most commonly used form of outpatient prophylaxis across all medical diagnosis groups, followed by enoxaparin (Table 2).
The mean ± SD total duration of prophylaxis was 2.2 ± 5.7 days for all medical patients (n = 15 721) and 5.3 ± 8.0 days if limited to those medical patients who received some form of prophylaxis (n = 6385). The longest total mean length of prophylaxis was observed in patients with congestive heart failure (Table 3 ). Mean inpatient prophylaxis duration for all patients was slightly over 1 day for all medical conditions and around 3 days if limited to those patients who received any prophylaxis. Mean ± SD outpatient prophylaxis duration was 2.9 ± 8.9 days for all patients with congestive heart failure (n = 1333) and 6.2 ± 12.2 days if limited to those patients with congestive heart failure who received prophylaxis (n = 624). The mean outpatient prophylaxis duration for the other medical conditions was less than 1 day for all patients and less than 2.5 days if limited to those patients with any prophylaxis (Table 3). The mean ± SD length of hospital stay ranged from 3.9 ± 4.0 days in patients with cancer to 4.5 ± 3.5 days in patients with infectious disease or severe lung disease (Table 3).
Durations of Hospital Stay and Prophylaxis
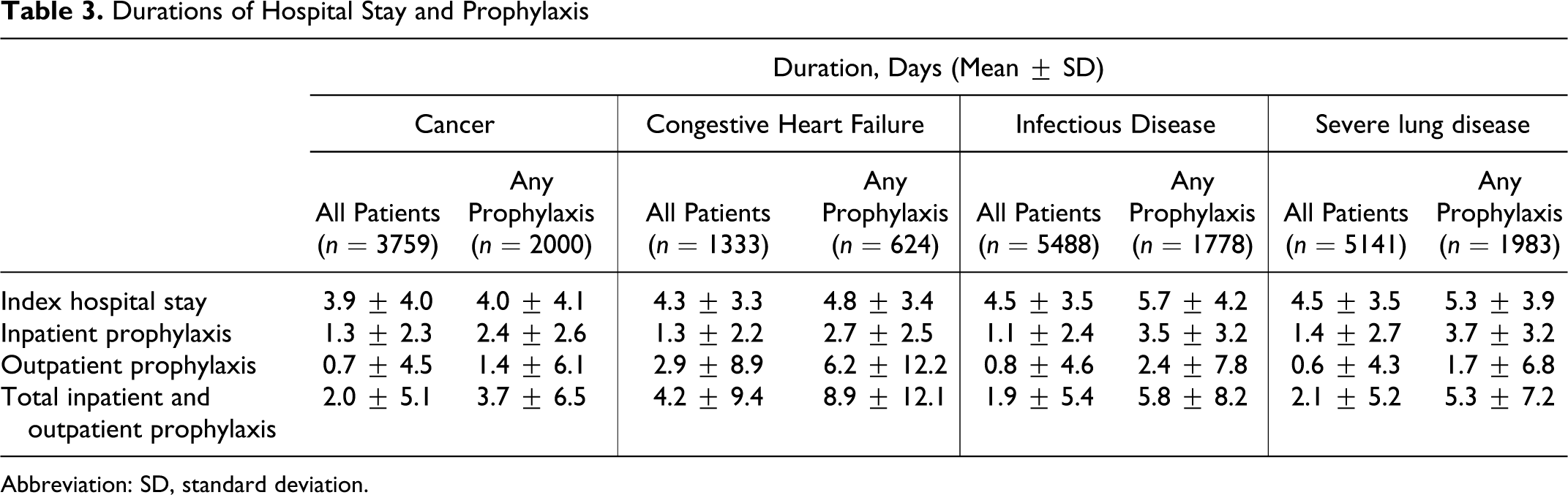
Abbreviation: SD, standard deviation.
A symptomatic DVT or PE event was experienced by 646 medical patients (4.1%). During their index hospitalization, 475 (3.0%) of all medical patients experienced a DVT/PE event, with 323 cases of DVT and 152 cases of PE. In the 30-day period postdischarge, 123 patients (0.8%) were readmitted for DVT/PE, with 77 cases of DVT and 46 cases of PE. A total of 48 patients (0.3%) were treated in the outpatient setting for DVT/PE; DVT in 36 patients and PE in 12 patients. When analyzed by medical condition, both the highest total DVT/PE rate and the highest inpatient DVT/PE rate occurred in patients with infectious disease (4.6% and 3.6%, respectively; Figure 3 ). The highest postdischarge DVT/PE rate was in patients with cancer, with 1.3% of patients readmitted for DVT/PE and 0.3% receiving outpatient DVT/PE treatment. Indeed, outpatient DVT/PE accounted for the highest proportion of the total DVT/PE events in patients with cancer (40.5%) compared with the other medical diagnosis groups (~20%).

Deep-vein thrombosis (DVT) and/or pulmonary embolism (PE) rates during the index hospitalization, and rates of readmission to hospital or treatment in the outpatient setting for DVT/PE in the 30-day period after discharge.
When the type of inpatient DVT/PE event was analyzed, patients with infectious disease had the highest frequency of DVT (3.0%), whereas patients with severe lung disease had the highest frequency of PE (1.5%; Figure 4 ). In the outpatient setting, patients with cancer had the highest percentage of DVT (1.1%). A relatively large number of cases of PE occurred in outpatients with cancer and those with severe lung disease (both 0.5%).
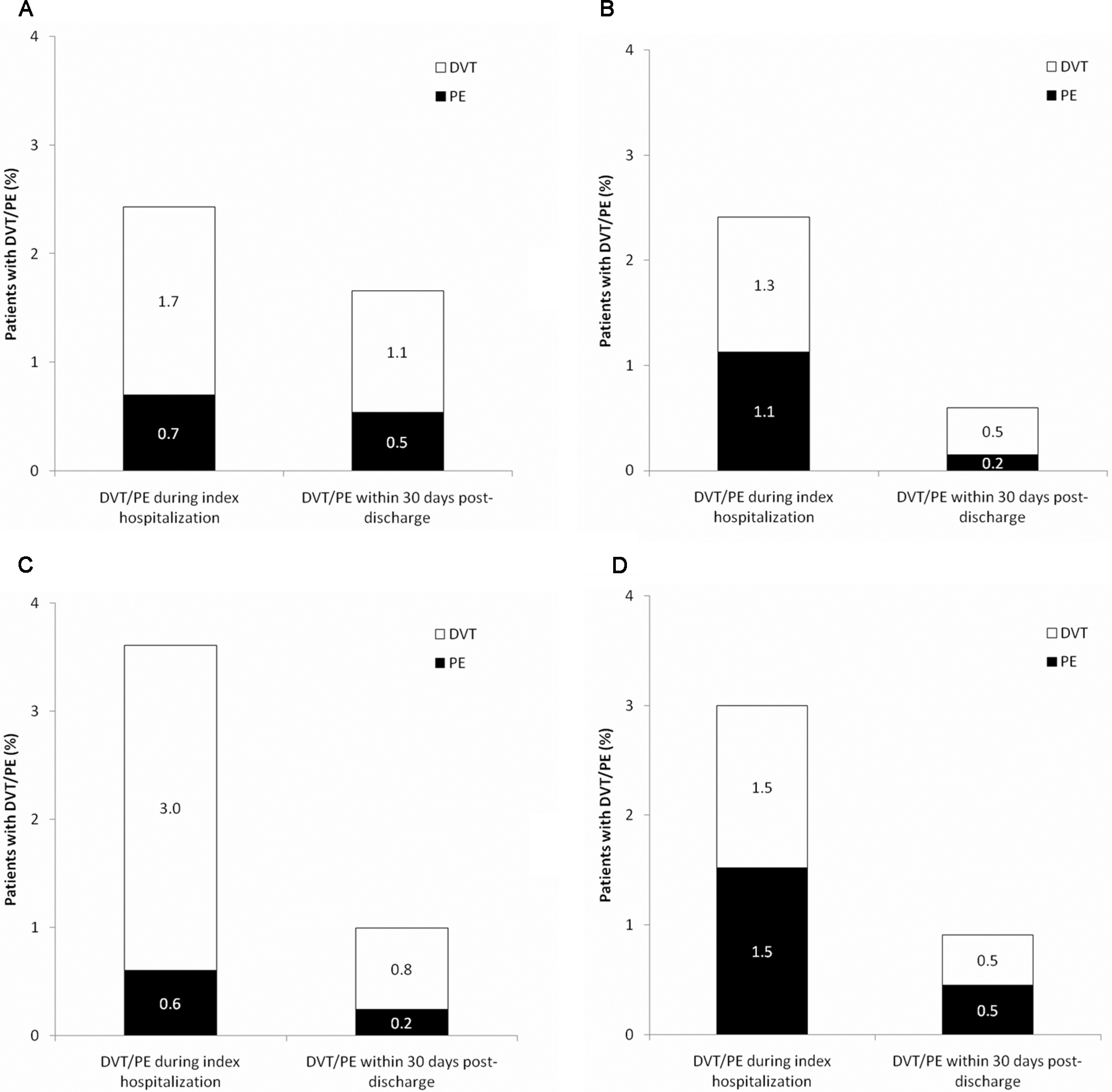
Breakdown of Deep-vein thrombosis (DVT) and/or pulmonary embolism (PE) events by medical condition: (A) cancer, (B) congestive heart failure, (C) infectious disease, and (D) severe lung disease.
In a correlation analysis, a negative correlation between the inpatient DVT/PE event rate and the inpatient prophylaxis rate was found, with a correlation coefficient (R 2 ) of 0.72 (Table 4 ). A negative correlative relationship between the inpatient DVT/PE event rate and inpatient prophylaxis duration had an R 2 of 0.19 (Table 4). Negative correlative relationships were also observed between the postdischarge DVT/PE rate and either outpatient prophylaxis rate or outpatient prophylaxis duration (R 2 = 0.42 and R 2 = 0.43, respectively; Table 4).
Correlative Relationship Between DVT and/or PE Rates in Hospital or Postdischarge, and Prophylaxis Rate or Duration
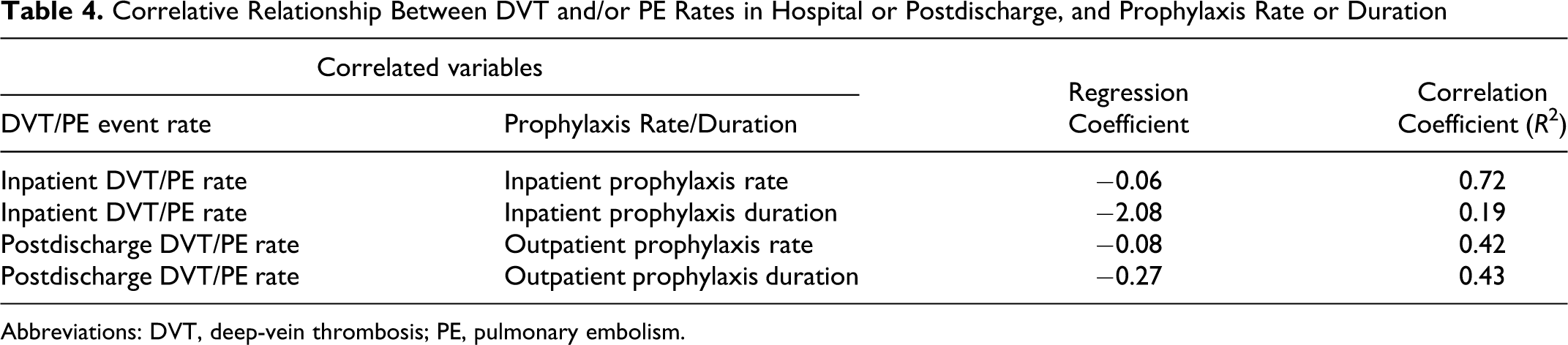
Abbreviations: DVT, deep-vein thrombosis; PE, pulmonary embolism.
Discussion
Our study demonstrated a substantial clinical burden of DVT/PE in medical patients, with 3.0% of inpatients developing clinical DVT/PE. The overall rate of postdischarge DVT/PE of 1.1% seen in the present study, representing 27% of all DVT/PE events, contributes to the growing evidence-base regarding the persistent risk of DVT/PE after hospitalization.3,4 In a study of 1897 medical and surgical patients with a confirmed episode of DVT/PE, 74% of patients developed DVT/PE in the outpatient setting. 4 In a study by Spyropoulos et al., 3 DVT/PE events in medical patients occurred most frequently postdischarge, with a median time to event of 74 days, ranging from 62 days in patients with severe infectious disease to 126 days in patients with congestive heart failure. The current study assessed outpatient DVT/PE events over a 30-day period, thus the true extent of postdischarge DVT/PE may be underestimated. About half of all readmissions to hospital for thromboembolic events after initial hospitalization for a medical condition occur within a 30-day period, 16 and this period is generally used as an appropriate period for assessment of postdischarge DVT/PE events.1,2,17
Despite the risk of DVT and evidence-based guidelines recommending thromboprophylaxis, data from our study indicate that more than half of real-world medical patients did not receive any form of prophylaxis. These results are consistent with recent studies, where the low level of inpatient prophylaxis prescribing has also been demonstrated.3,11–13 A subanalysis of the Epidemiologic International Day for the Evaluation of Patients at Risk for Venous Thromboembolism in the Acute Hospital Care Setting (ENDORSE) study demonstrated that only approximately half of all medical patients received any form of prophylaxis. 13 The current study only determined whether any form of prophylaxis was prescribed and did not assess whether prophylaxis was appropriate according to evidence-based guidelines in terms of type, dose, or duration. 1
In the current study, inpatient prophylaxis rates were highest in patients with cancer (51.9%) and lowest in patients with infectious disease (31.1%). In our recently published large-scale US study of discharge records from medical inpatients, the highest rates of prophylaxis were in patients with congestive heart failure (59.4%) and cancer (52.3%) and lowest in patients with infectious disease (40.4%). 12 The consistency of the prophylaxis rates that were observed in both studies indicates face validity of the study results. Although patients with cancer had the highest rate of inpatient prophylaxis, the primary method was mechanical prophylaxis, which is not the ACCP-recommended prophylaxis method for these patients unless they are actively bleeding or at high risk for bleeding. 1 The low rate of prophylaxis in patients with infectious disease suggests that physicians caring for these patients need to be made particularly aware of the risks of DVT/PE and the need for adequate prophylaxis. In line with the correlation analysis, patients with infectious disease, who had the lowest prophylaxis rate, had the highest total inpatient DVT/PE rate (4.6%). The ACCP guidelines do not specifically identify patients with infectious disease as patients at risk of DVT/PE, other than those with sepsis. 1 However, a subanalysis of the Prophylaxis in MEDical patients with ENOXaparin (MEDENOX) trial demonstrated that acute infectious disease was independently associated with increased risk of DVT/PE (odds ratio 1.74, 95% confidence interval 1.12 to 2.75). 18 Further, in-hospital efforts for improvement of DVT prevention are required across all medical specialties.
Only 3.4% of medical patients received anticoagulants on an outpatient basis. Even among patients with congestive heart failure, who had the highest outpatient rate, only 1 in 10 patients received anticoagulants postdischarge. These findings are consistent with the study by Spyropoulos et al, 3 where postdischarge prophylaxis was provided to 13.1% of patients with congestive heart failure and <5% of patients from the other diagnosed medical groups. As our study assessed outpatient use of anticoagulants, and warfarin was used most commonly, the rate reported here may be an overestimation of the true outpatient thromboprophylaxis rates, as patients with congestive heart failure may have received warfarin for reasons other than DVT prevention, such as decreased left ventricular ejection fraction.
In the current study, the mean length of hospital stay ranged from 3.9 to 4.5 days, thus the majority of patients who were prescribed in-hospital prophylaxis alone will not have received the standard period of 6 to 14 days prophylaxis found to effectively reduce DVT in clinical trials.5–7 With the shortening of hospital stays, increased use of outpatient prophylaxis will likely be required to ensure that medical patients receive prophylaxis of adequate duration. In our study, mean postdischarge prophylaxis duration was 2.9 days in patients with congestive heart failure and <1 day in patients with other medical conditions. Correlations assessed in our study showed that the medical conditions with the lowest inpatient prophylaxis rate had the highest in-hospital DVT/PE event rate; however, caution should be exercised in the interpretation of this finding, as patient groups of different medical conditions were compared.
As is being increasingly recognized, there is a need to implement quality improvement measures to increase prophylaxis rates and thus reduce DVT/PE event rates. Multiple active interventions in the form of educational programs, risk stratification, critical pathways, and alert tools have been found to be effective at increasing rates of thromboprophylaxis in hospital.19–22 In one study, a message alert was incorporated into the institution’s computerized prescriber-order entry system to act as a reminder to assess patients' DVT/PE risk factors and the need for prophylaxis. 22 Extensive education about the program was provided to hospital staff, pharmacists, physicians, and nurses. Following implementation of the program, prophylaxis prescribing increased from 49% of medical patients to 93% (P < .001). 22 Another study assessed implementation of a multifaceted prophylaxis quality improvement intervention combining regular education, dissemination of a decision support tool, and regular audit and feedback. 19 At baseline, 47% of medical patients received any prophylaxis, with prophylaxis inappropriately prescribed as often as it was appropriately prescribed (43%). Eighteen months after implementation, the proportion of patients receiving prophylaxis significantly increased to 86% (P < .01) and the rate of appropriate prophylaxis increased to 85% (P < .01). 19 Further strategies may need to be adopted to increase outpatient prophylaxis, and this is an area requiring additional attention and investigation.
The current study is unique in that it assessed both in-hospital and postdischarge rates of DVT/PE as well as prophylaxis from real-world databases that were cross-matched at the individual patient level. The results on rates of in-hospital DVT/PE, rehospitalization for DVT/PE, and outpatient treatment of DVT/PE extend on previously reported findings, where we reported only on DVT prophylaxis rates in-hospital and post-discharge from similarly matched databases. 23
There are a number of caveats to using claims data in the current analyses. The Premier Perspective™-i3 Pharma Informatics-linked databases, representing a managed care population, may not be representative of the US population as a whole. Basic patient demographics in our population (49% males; 69% white; mean age 54 years) appear similar to those reported by the US Census Bureau for the overall US population based on 2008 data (49% males; 75% white; median age 37 years). 24 Our population, however, is older than the overall US population reported by the US Census Bureau, but this may reflect the fact that only patients ≥18 years of age were included in our study. As the contribution of patients <18 years of age to the medical conditions included in this study is minor, it is unlikely that this will have affected the outcomes of this analysis. Conversely, our population is relatively young compared with the clinical trials, which have used age cutoffs of >40 or ≥60 years; this may have led to lower rates of DVT/PE in the current study and lower thromboprophylaxis rates as young patients are less likely to receive (postdischarge) prophylaxis. A large number of patients (n = 12 619) were excluded from this study because they were discharged or transferred to an acute-care facility. Had these patients been included, the rate of outpatient prophylaxis would have been artificially low, as prescriptions for anticoagulants for those patients would have been unavailable from the databases used. Similarly, we would not have captured DVT/PE readmissions for these patients due to treatment in the other facilities.
The reliability of the scoring of DVT/PE events and other diagnoses relies on the coding accuracy of the physicians in the hospitals. Inaccurate coding has the potential to lead to both overestimation and underestimation of total DVT/PE events. Furthermore, studies that have examined the positive and negative predictive value of using ICD-9-CM codes from administrative data to identify DVT/PE events have reported a high level of false-positives,25–27 which may have led to an overestimation of the total DVT/PE events in the current study.
Another limitation is that outpatient use of mechanical prophylaxis, such as graduated compression stockings, was not captured due to over-the-counter availability. Therefore, only the use of pharmacological prophylaxis was measured among outpatients, which is an underestimation of the total use of any prophylaxis in the outpatient setting. Patients on chronic warfarin were not excluded from the study, except for those with atrial fibrillation. Therefore, some patients may have received anticoagulants (especially warfarin) for reasons other than prevention of DVT. The current study only determined whether any form of prophylaxis was prescribed and did not assess whether prophylaxis was appropriate according to evidence-based guidelines in terms of type, dose, or duration. Therefore, the prophylaxis rates may have been overestimated in this study.
To conclude, our analysis demonstrates the substantial burden of DVT/PE in medical patients both in-hospital and postdischarge and highlights the current underuse of thromboprophylaxis in both settings. There is a need for improved thromboprophylaxis prescribing across the continuum of care in order to reduce the burden of preventable DVT/PE events.
Footnotes
Acknowledgments
sanofi-aventis U.S., Inc provided funding to Quintiles Consulting to perform this study. The authors received editorial/writing support in the preparation of this manuscript, which was provided by Hester van Lier, PhD, of Excerpta Medica and funded by sanofi-aventis U.S., Inc. All authors had full access to the data and contributed to the drafting of the paper.
The author(s) declared a potential conflict of interest as follows: Alpesh Amin has received research honorarium and is on the speakers bureau for sanofi-aventis U.S., Inc. Jay Lin is an employee of Bruce Wong and Associates, which received research funding from sanofi-aventis U.S., Inc. Stephen Thompson is an employee at sanofi-aventis U.S., Inc. Daniel Wiederkehr is an employee at Quintiles Consulting, which received funding to carry out this work from sanofi-aventis U.S., Inc.
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: sanofi-aventis U.S., Inc provided funding to Quintiles Consulting to perform this study. The authors received editorial/writing support in the preparation of this manuscript funded by sanofi-aventis U.S., Inc