
Abstract
To investigate the associations between soluble Lectin-like Oxidized Low-density lipoprotein receptor-1 (sLOX-1) and clinical prognosis, especially infarct volume in patients with acute atherosclerosis-related ischemic stroke. We recruited acute ischemic stroke patients within 3 days after onset. Patients were stratified into 3 groups by sLOX-1 level. Initial stroke severity was assessed using the National Institutes of Health Stroke Scale scores, and infarct volume was measured using DWI by ITK-SNAP software. The clinical prognosis was evaluated by DWI volume, clinical response at discharge, and functional outcome at 90 days. Spearman rank correlation analysis was used to examine associations between circulating sLOX-1 levels and infarct volumes. Logistic regression was used to explore the relationship between sLOX-1 levels and clinical prognosis. A total of 207 patients were included in our study. The median DWI volume in the lowest sLOX-1 tertile was 1.98 cm3, smaller than 4.26 cm3 in the highest sLOX-1 group. The Spearman rank correlation coefficient between sLOX-1 levels and DWI volume was 0.47 (P < .01). Compared with the highest sLOX-1 tertiles, patients in the lowest sLOX-1 tertile had a higher risk of favorable functional outcome at 90 days (OR = 3.47, 95% CI, 1.21-9.96) after adjusting traditional risk factors. However, there was no difference between sLOX-1 level and clinical response at discharge. For patients with acute atherosclerosis-related ischemic stroke, circulating sLOX-1 level is correlated with DWI volume in the acute phase and favorable functional outcome at 90 days, but not with the clinical response at discharge.
Keywords
Introduction
Stroke is a leading cause of serious disability in the world. 1 Atherosclerosis is the main pathological mechanism of stroke. Although oxidative stress and inflammation have been recognized as the pivotal pathological processes of atherosclerosis, the cellular and molecular mechanisms that lead to the formation and rupture of atherosclerotic plaques remain unclear. 2 Therefore, understanding of these processes is required to provide novel biomarkers to explore the potential predictors of prognosis after stroke.3,4
Lectin-like Oxidized Low-density lipoprotein receptor-1 (LOX-1) has been identified as the dominant receptor of oxidized low-density lipoproteins (ox-LDLs) in mediating the development of atherosclerosis. 5 LOX-1 is expressed on the surface of cells involved in atherosclerosis, such as endothelial cells, macrophages, and smooth muscle cells. 6 The LOX-1–ox-LDL interaction induces endothelial dysfunction, leukocyte adhesion, macrophage-derived foam cell formation, smooth muscle cell proliferation and migration, and platelet activation, 7 implicating the initiation, progression, and destabilization of atheromatous plaques, contributing to the plaques rupture and acute cardiovascular events onset eventually.6,8 LOX-1 is demonstrating a key role in determining outcomes following ischemia/reperfusion injury in animal experiments,9,10 blocking LOX-1 gene expression may decrease both stroke volume and neurological impairment. 9 Although LOX-1 can be proteolytically cleaved into a soluble form (soluble LOX-1, sLOX-1) and can be detected in the circulation,11,12 the associations between sLOX-1 and acute atherosclerosis-related ischemic stroke were limited relatively, especially infarct volume. Therefore, the objective of this study is to investigate it.
Methods
Study Population
This study was approved by the ethics committee of Shanghai Fifth People's Hospital. Signed informed consents were obtained from the patients or their representatives, and the protocols complied with the Declaration of Helsinki. As an observational and longitudinal study, we recruited acute ischemic stroke patients within 3 days after onset consecutively. According to the purpose of this study, only patients with large artery atherosclerotic or small-artery atherosclerotic occlusion cerebral infarction were included in our analysis finally(based on trial of org 10172 in Acute Stroke Treatment criteria. 13 Patients who met any one of the following criteria were excluded: history of stroke, no cerebral MRI, cardioembolism, determined etiology cerebral infarction, undetermined etiology cerebral infarction, intravenous thrombolysis, and arterial thrombectomy.
Clinical and Laboratory Variables
Baseline data on patient demographics and clinical characteristics were obtained after admission through face-to-face interviews by the neurologist. Venous fasting blood samples were taken on the second day after admission. A set of blood samples were used for routine blood examination, the other samples were centrifuged (2000 g for 5 min) immediately after collection, and were stored in a –80℃ refrigerator for the detection of sLOX-1 concentrations. sLOX-1 level was tested by a sandwich enzyme-linked immunosorbent assay kit (RapidBio Laboratory, USA) by following the manufacturer's instructions.
Clinical Prognosis
The clinical prognosis was evaluated by DWI volume in the acute phase, the clinical response at discharge, and functional outcome at 90 day.
DWI volumes in the acute phase were measured with reference to the methods of Yang et al 2021. 14 All patients underwent multimodal MR imaging within 96 h of admission. MR imaging examinations were performed using 3.0-tesla (Magnetom Skyra, Siemens, Germany). ITK-SNAP software (Version 3.8.0) was used to measure the acute infarct volumes indicated by DWI (http://www.itksnap.org/pmwiki/pmwiki.php). 15 The images were independently rated by 2 blinded stroke neurologists (Chen Li and Xiaoli Yang). A subset of images was reviewed by them to assess inter-rater agreement, and inter-rater reliability was 0.88. The average infarct volume of 2 neurologists was used for analysis.
Neurological deficit was assessed by the National Institutes of Health Stroke Scale (NIHSS) scores. 16 According to a common consensus of neurological practitioners, the degree of neurological deficit at the time of presentation was divided into 3 grades: mild, NIHSS score ≤ 4; moderate, 5 ≤ NIHSS < 10; severe, NIHSS ≥ 10. Compared with the NIHSS score at the time of presentation, the clinical response at discharge was divided into 3 grades, NIHSS of 0 or ≥ 4 points of remission was defined as neurological improvement, 17 and ≥ 2-point increase was defined as neurologic worsening. 18 Modified Rankin scale (mRS) score was used to evaluate functional outcome at 90 days, where 0 to 2 (able to look after own affairs without assistance) was defined as a favorable outcome and 3 to 6 (unable to look after own affairs or death) was defined as a poor outcome with reference to other previous studies.
Statistical Analyses
Statistical analyses were performed using the SPSS21.0 software. Patients were classified into 3 groups by sLOX-1 level. For each demographic and clinical feature, normal distribution continuous variables were presented as mean ± standard deviation and compared by an independent sample t-test. Abnormal distribution continuous variables were presented as median (interquartile range) and compared by a nonparametric test. Categorical variables were expressed as frequency (percentage) and compared by χ2 test or Fisher exact test. Associations between circulating sLOX-1 levels and DWI infarct volumes were examined using Spearman rank correlation analysis. The association between circulating sLOX-1 levels and clinical outcome was performed by logistic regression. For all regression models, age, sex, and variables showing P < .2 on the respective univariate analyses were included in the models. A P < value .05 was considered significant.
Results
Demographic and Clinical Characteristics of the Study
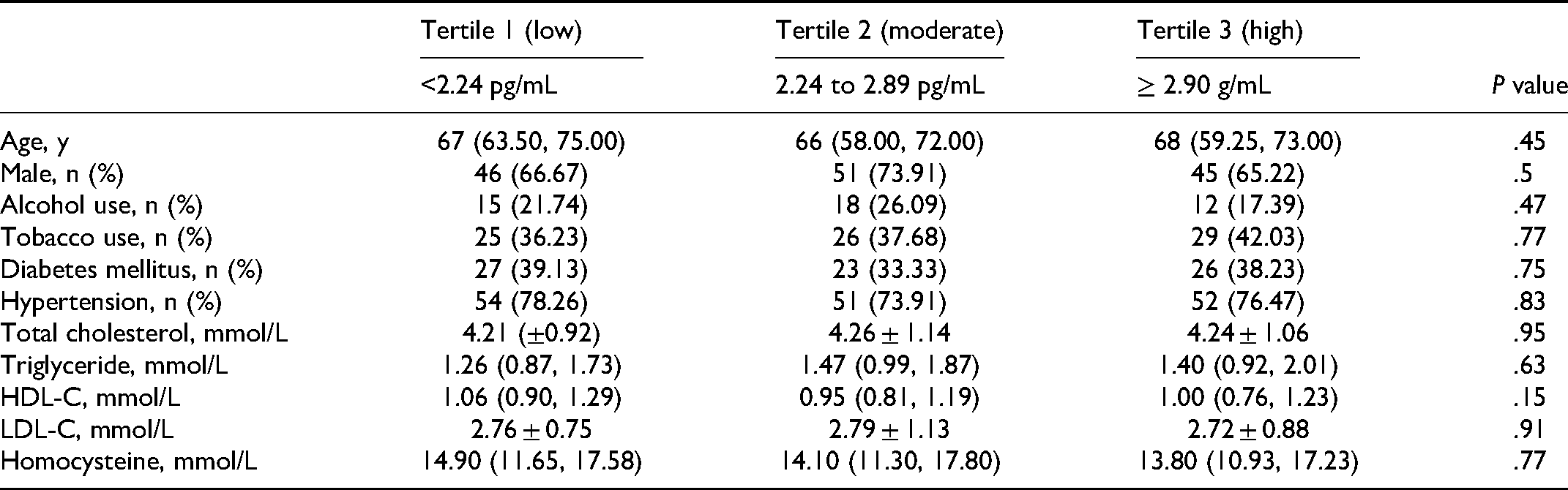
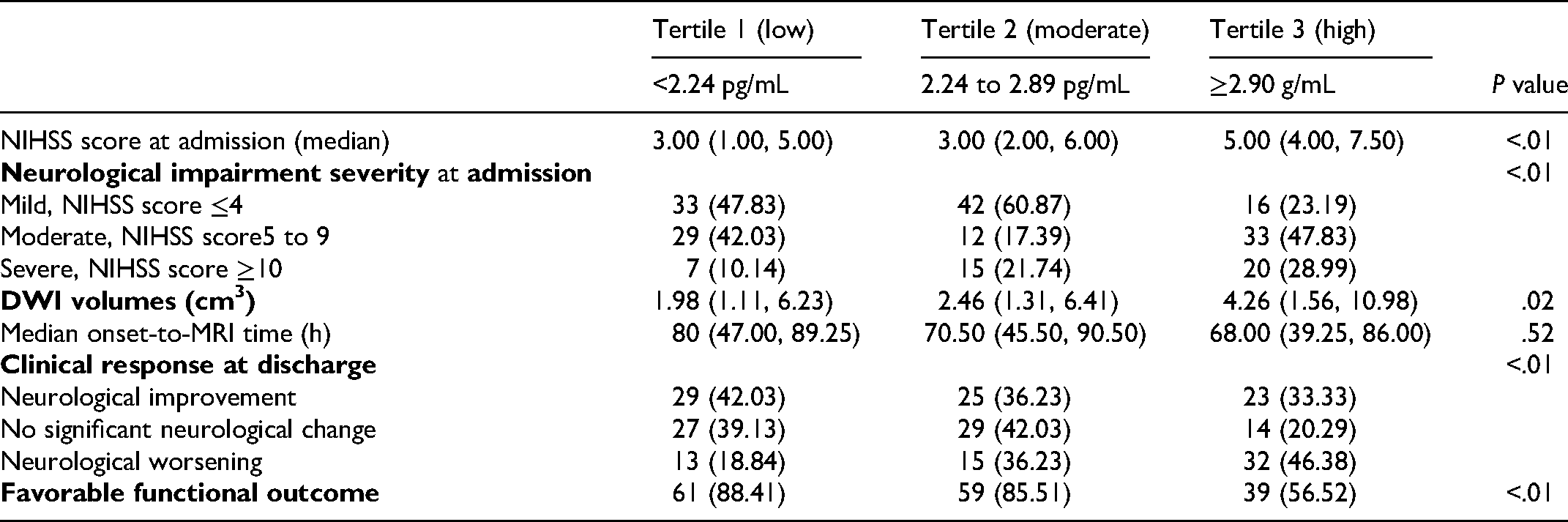
A total of 207 patients were included in our study. According to the circulating sLOX-1 level, the patients were stratified into 3 groups: Tertile 1, sLOX-1 level <2.24 pg/mL; Tertile 2, sLOX-1 level was 2.24 to 2.89 pg/mL; Tertile 3, the sLOX-1 level ≥2.90 pg/mL. Demographic and baseline clinical characteristics of patients in different circulating sLOX-1 level groups were provided in Table 1. There were no significant differences in age, hypertension, diabetes mellitus, LDL-C, and total cholesterol in patients with different sLOX-1 level groups (P ≥ .05). The proportion of severe neurological deficit at admission in patients with the lowest sLOX-1 tertile was10.14%, much lower than the other 2 groups (21.74% for Tertile 2 group and 28.99% for Tertile 3 group) (Table 2).
Demographic and Clinical Characteristics According to Different Circulating sLOX-1 Level Groups.
Circulating sLOX-1 Levels and Infarct Volume in the Acute Phase
There were differences in infarct volume in different sLOX-1 level groups (P = .02). The median DWI volumes in patients with the low sLOX-1 level group were 1.98 cm3, in the moderate group was 2.46 cm3, and in high group was 4.26 cm3 (Table 2). With the increase of sLOX-1 level, the infarct volume increased gradually. The Spearman rank correlation coefficient (rho) between sLOX-1 levels and DWI volumes was 0.47 (P < .01).
Clinical Course and Outcome Features Between Different sLOX-1 Level Groups.
Circulating sLOX-1 Level and Neurological Functional Prognosis
There were differences in clinical response at discharge among the 3 groups. With the increase of sLOX-1 level, the proportion of neurological worsening ascended (18.84%, 36.23%, and 46.38%, respectively), but the ratio of neurological improvement descended gradually (42.03%, 36.23%, and 33.33%, respectively). A higher prevalence of favorable functional outcome at 90 days was found in patients with the lowest sLOX-1 tertile compared to the other 2 groups (88.41% vs 85.51% vs 56.52%, P < .01) (Table 2).
We assessed the association between sLOX-1 level and other cardiovascular risk factors with acute ischemic stroke prognosis by multivariable logistic regression. After adjusting traditional risk factors, sLOX-1 level was negatively associated with favorable functional outcome at 90 days (P = .02). Compared with the highest sLOX-1 tertiles, patients in the lowest sLOX-1 tertile had a higher risk of favorable functional outcome at 90 days (OR = 3.47, 95%CI, 1.21-9.96), but there was no difference between sLOX-1 level and clinical response at discharge (Table 3).
Logistic Regression Model for Predictors of Neurological Functional Prognosis.

Abbreviations: LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; NIHSS, National Institutes of Health Stroke Scale; T, tertile.
Discussion
In our study, we found that in patients with acute atherosclerosis-related ischemic stroke, sLOX-1 level is correlated with DWI volume and favorable functional outcome at 90 days, but not with the clinical response at discharge.
OxLDL has proatherogenic and proinflammatory properties, and has been identified as involved in the initiation and progression of atherosclerosis.6,19 LOX-1 is the receptor of oxLDL, expressed extensively on the surface of cells involved in atherosclerosis. 6 Its expressed level was low in basal conditions but increased when exposure to proinflammatory cytokines, pro-oxidative and biomechanical stimuli environment.20–22 LOX-1 can be proteolytically cleaved into a soluble form (sLOX-1) and be detected in the circulation,11,12 it has been assumed that sLOX-1can reflects the cellular and atherosclerotic plaque expression of LOX-1.21,23 In the field of cardiovascular, sLOX-1 appears to have potential as a prognostic biomarker among patients with coronary artery disease. 24 Given the pathophysiological mechanisms of coronary and cerebrovascular atherosclerosis are considered similar, whereas the association between sLOX-1 and acute atherosclerosis-related ischemic stroke is limited relatively, especially the infarct volume in the acute phase, so we investigate it.
One of the major findings of this study was that circulating sLOX-1 level is correlated with DWI volume in the acute phase. With the increase of sLOX-1 level, the infarct volume increased gradually, and the Spearman rank correlation coefficient (rho) between sLOX-1 levels and DWI volume was 0.47 (P < .01), which was confirmed with the results of basic research further.9,10 A series of studies have demonstrated that blocking LOX-1 gene expression could decrease both stroke volume and neurological impairment,9,10 considering which was related to ischemia/reperfusion injury. Because arterial ischemia-reperfusion injury can induce the expression of LOX-1 being upregulated, leading to lipid peroxidation and apoptosis. On the contrary, LOX-1 gene knockout or the administration of an anti-LOX-1 antibody can inhibit these effects. 10 However, some clinical studies found that there was no significant difference in the level of serum sLOX-1 between different infarct volume groups. 25 This may be related to the different study design. Li et al's 25 study included acute stroke of various subtypes, and the infarct volume was calculated by the manual method, whereas our study just focused on large artery atherosclerotic and small artery atherosclerotic occlusion cerebral infarction, in addition, the infarct volume was calculated by ITK-SNAP software.
sLOX-1 is a biomarker of atherosclerotic-related diseases.21,23,24 In the field of cardiovascular, it is well-known that sLOX-1 levels can reveal the severity of acute coronary syndrome and is related to the prognosis of coronary artery disease.20,24 In the research of cerebrovascular disease, sLOX-1 levels were elevated in patients with ischemic stroke and transient ischemic attack,26–28 and the elevated were more significantly in severe patients compared to the mild stroke group. 28 Which was confirmed in our study further, we found the proportion of severe neurological deficit at admission in patients with the low level of sLOX-1 was10.14%, much lower than the other 2 groups (21.74% for moderate level of sLOX-1 group and 28.99% for the high level of sLOX-1group). Secondly, sLOX-1 was supposed to be a novel biomarker for the prognosis of large-artery atherosclerotic stroke.25,27 Markstad et al's 21 study demonstrated that subjects in the highest tertile of sLOX-1 had a stroke hazard ratio of 1.75 compared with those in the lowest tertile after adjusting risk factors. In our study, circulating sLOX-1 level was negatively associated with favorable functional outcome at 90 days. Compared with the high sLOX-1 level group, the low sLOX-1 level group was 3.47 times more likely to have a favorable functional outcome at 90 days (OR = 3.47, 95% CI, 1.21-9.96), which was consistent with previous studies. To understand the close relationship between sLOX-1 levels and the clinical prognosis of acute atherosclerosis-related ischemic stroke, except for the well-known LOX-1–ox-LDL interaction that promotes plaque formation and triggers disease progression via several mechanisms, we proposed several possible explanations as follow.
One explanation is that LOX-1 participates in the pathogenesis of neuron apoptosis. 29 It has been demonstrated that LOX-1 can increase Bax/Bcl-2 ratio or through caspase-3 and caspase-9 pathways to promote neuron apoptosis, whereas the elevated Bax/Bcl-2 ratio is a parameter to determine the cell susceptibility of apoptosis. 30 The second is that LOX-1 can cause blood-brain barrier (BBB) disturbance through endothelial cells pathways.6,31 Endothelial cells are an important part of the BBB, its dysfunction may contribute to the BBB disturbance, an increase of the permeability of the BBB, leakage of proteases, immunoglobulins, complement components, and cytokines into brain tissue, damaging to brain tissue further. 32 On the contrary, deficiency of LOX-1 has a protective effect on brain damage. 32 Liang et al's 32 study performed an analysis of miRNAs for ischemic brain damage, supporting a potential involvement of LOX-1 in BBB disruption after cerebral ischemia. Third, LOX-1 was identified to interact with immune activity and oxidative stress in the brain tissue of mice. 33 In-vivo experiments in mice, LOX-1/NADPH oxidase/ROS/P38 MAPK/NF-kB/autophagy axis was demonstrated to play an important role in the activation of TLR4 that regulates inflammatory responses in the brain. 33
There are some limitations of the present study that need to be considered. First, we measured sLOX-1 levels, not LOX-1 level, but studies demonstrated that patients undergoing carotid endarterectomy had a significant association between plasma sLOX-1 and the plaque content of sLOX-1. 21 Second, we measure the baseline sLOX-1 level only at the acute stage of stroke, the dynamic change of sLOX-1 at different stages could not be presented in this study, further studies with repeated measurement intervals are needed.
Conclusions
Overall, we confirmed that for patients with acute atherosclerosis-related ischemic stroke, sLOX-1 level is correlated with DWI volume in the acute phase and favorable functional outcome at 90 days, but not with the clinical response at discharge. Further studies should be conducted to evaluate the use of LOX-1 as a therapeutic target to modify atherosclerosis and related diseases.
Footnotes
Acknowledgment
We sincerely thank the patients, families, general practitioners, and hospital colleagues who participated into our study.
Author Contributions
XY and CL measured acute infarct volumes. TW rated MR imaging, disagreement was resolved by consensus with WL. WS measured circulating sLOX-1 level. DH, JL, YL, LS were responsible for collecting data. XY and DW analyzed data. XY wrote the article, DW and WL polished the final manuscript. All authors read and approved the final manuscript.
Ethical Approval
This study was performed according to the principles of the Declaration of Helsinki and was approved by the ethics committee of Shanghai Fifth People's Hospital. Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Informed Consent
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by grants from Shanghai Municipal Commission of Health and Family Planning (20184Y0178), Shanghai Minhang District Health and Family Planning Commission for constructing big disciplines (2020MWDXK01), Minhang District High Level Specialist Backbone Physician Training Plan (2020MZYS09), Beijing Bethune Public Welfare Foundation (AX083CS).