
Abstract
An upregulation of platelet CD40 ligand (CD40L) and CD62P has been described in atherosclerotic cardiovascular diseases and among patients with acute cerebral ischemia. Correlation between platelet and monocyte activation and the etiology of ischemic stroke were examined in 41 patients with acute ischemic stroke. Compared to 10 controls, all patients with stroke showed a significantly elevated platelet expression of CD40L (P < .001) and had significantly higher amounts of platelet–monocyte aggregates (P = .002). Plasma levels of interleukin 7 were significantly lower in patients with stroke compared to controls (P = .006). Patients with small artery disease had a significantly higher platelet CD40L expression than patients with cardioembolic stroke (P = .029). Plasma levels of soluble CD40L were significantly higher in patients with large artery disease compared to patients with cardioembolic stroke (P = .047). In conclusion, patients with acute ischemic stroke show an upregulation of platelet CD40L and an activation of cellular coagulation with highest activation in the large artery disease subgroup.
Introduction
Acute ischemic stroke represents a common and challenging disease with increasing morbidity despite decreasing mortality.1,2 Subgroups of atherosclerotic ischemic stroke include large artery disease (20%-25%), small artery disease (15%-20%), and cardioembolic stroke (25%-35%), often due to distinct or overlapping mechanisms. 2
Atherosclerosis as the major underlying disease entity in patients with stroke is a chronic inflammatory disease with a considerable involvement of platelets and monocytes in the initiation and progression of atherosclerotic lesions.3–8 Vascular pathology is affected by the expression and release of several factors upon platelet stimulation and subsequent aggregation as well as monocyte activation. These factors include P-selectin, an α-granule protein that mediates platelet rolling, leukocyte adhesion and coagulation, tissue factor expression on monocytes, platelet–monocyte aggregates, and CD40L, a member of the tumor necrosis factor-α (TNF-α) family of proteins.6,9–12
Within the last years, an activation of monocytes and platelets with an upregulation of platelet CD40L not only has been described among patients with atherosclerotic cardiovascular diseases but was also increasingly observed among patients with acute cerebral ischemia.9,13–20 Elevated platelet activation markers, particularly CD62P and CD40L, are directly associated with ischemic stroke21,22 and platelet activation, and platelet–monocyte interactions seem to play a proven role in cerebrovascular ischemia. 23
Vascular plaque destabilization is supported by inflammatory conditions and at least partially is due to an upregulation of the platelets CD40L and CD62P system as well as an activation of cellular coagulation.16,21
However, still little is known about the decisive role of platelets and monocytes in acute ischemic stroke with regard to ischemic stroke subtypes and in view of a possible correlation between platelet and monocyte activity markers and stroke etiology. Therefore, the aim of the present study was to assess the correlation between platelet and monocyte activation and the etiology and extent of ischemic stroke in patients with cardioembolic stroke and in patients with atherosclerotic ischemic stroke originating from large and small artery diseases.
Methods
Study Participants
Whole blood samples of 41 patients with acute ischemic stroke (mean age 66.4 ± 14.2 years) were obtained and analyzed. Based on individual disease etiology, stroke types were subdivided into 3 groups. Group 1 included 17 patients (mean age 63.4 ± 16.2 years) with cardioembolic ischemic stroke. Group 2 included 11 patients (mean age 65.5 ± 16.6 years) with atherosclerotic ischemic stroke originating from large artery disease. Group 3 included 13 patients (mean age 71.1 ± 7.3 years) with atherosclerotic ischemic stroke originating from small artery disease.
In 10 controls (mean age 64.6 ± 12.9 years) relevant coronary atherosclerosis was excluded by coronary angiography and all controls were free of neurological symptoms such as cognitive impairment, sensomotor deficits, or psychomotor slowing as well as deficits in attention and executive functions.
Demographic data and concomitant medication of all patients with stroke and controls are displayed in Table 1 . Patients and controls did not differ with regard to risk factors and current treatment. Written informed consent for the participation in the study was obtained from each participant. The study was approved by the local ethics committee.
Demographic Data and Concomitant Medication of all Patients With Stroke and Controls a
Abbreviations: ACE, angiotensin-converting enzyme; SD, standard deviation; AT1, Angiotensin 1.
a Values are means ± SD.
b P value indicates data of all patients versus controls.
c P value indicates data of stroke subgroup comparison.
Experimental Design
Flow Cytometric Analysis
Blood samples of heparinized blood (15 IE heparin per mL blood; Sarstedt AG & Co, Nuembrecht, Germany) were obtained. To avoid aggregation and activation of platelets, the blood samples were shaken over the time. All whole blood samples were subsequently investigated on activation of monocytes and platelets as well as platelets binding on monocytes.
For the analysis of platelets, 100 μL of each sample were stained for 30 minutes at room temperature with 10 μL aliquots of mouse anti-human CD62P-PE antibodies (CLB-Thromb/6; Coulter Immunotech, Krefeld, Germany) and mouse anti-human CD40L-FITC antibodies (P2; BD Pharmingen, Heidelberg, Germany). For the analysis of monocytes, 100 μL of each sample were stained for 30 minutes at room temperature with 10 μL aliquots of Phycoerythrin (PE)-conjugated murine antibody against CD41 (Coulter Immunotech) and murine fluorescein isothiocyanate (FITC)-conjugated antibody against tissue factor (American Diagnostica, Pfungstadt, Germany). Isotype-matched mouse anti-human immunoglobulin 1 (IgG1) PE/FITC antibodies (Beckman Coulter, Marseille, France) were used as control. After incubation, erythrocytes were lysed with 500 μL Optilyse C (Coulter Immunotech). After 15 minutes, cells were resuspended in 500 μL phosphate-buffered saline (PBS) and were then ready for flow cytometric analysis.
For the measurement of CD62P and CD40L on platelets, a gating for forward and sideward scatter was performed. For measurement of CD41 on platelets adherent to monocytes to determine platelet–monocyte aggregates and for measurement of membrane-bound tissue factor, a gating for CD14 positivity (mouse anti-human CD14-ECD [RM052] from Coulter Immunotech) and sideward scatter was performed to identify monocytes. Platelet–monocyte aggregates were defined by a combined flow cytometric CD41 and CD14 positivity.
All flow cytometric analyses were performed on an EPICS XL-MCL machine (Coulter Immunotech) equipped with an argon laser tuned at 488 nm. Mean fluorescence intensity (MFI) was measured and all Fluorescence Activated Cell Sorting (FACS) data are expressed as MFI in this article. System II Version 3.0 software was used for data acquisition and evaluation. Compensation of the 4-channel fluorescence was precisely adjusted using Cyto-Comp reagents and Cyto-Trol control cells (Coulter Immunotech).
Enzyme-Linked Immunosorbent Assay
Plasma levels of soluble CD40 ligand (sCD40L), interleukin 6 (IL-6), and IL-7 were measured with an enzyme-linked immunosorbent assay (ELISA) kit (Quantikine) from R&D Systems GmbH (Wiesbaden-Nordenstadt, Germany), according to the manufacturer’s instructions.
Statistical Analysis
The calculations were performed using SPSS for Windows Version 11.5.1. Numerical data were expressed as means ± SD. Normal distribution of parameters was tested by Kolmogorov-Smirnov procedure. For data with normal distribution, a Student t test was applied; and for data without normal distribution, a Wilcoxon test was applied as a nonparametric test. A chi-square test was applied to compare demographic data and concomitant medication between the patients with stroke (subgroup) and controls. A 2-tailed probability value <.05 was considered significant.
Results
All patients with ischemic stroke showed significantly increased platelet and monocyte activation with a significant upregulation of platelet surface expression of CD40L (1.22 ± 0.08 vs 1.89 ± 0.09; P < .001; Figure 1A) and significantly increased platelet–monocyte aggregates (7.84 ± 1.45 vs 14.86 ± 1.40; P = .002; Figure 1B) compared to controls. Additionally, plasma levels of IL-7 were significantly lower in patients with stroke compared to the control group (1.87 ± 0.19 pg/mL vs 4.16 ± 0.64 pg/mL; P = .006; Figure 1C). Tissue factor binding on monocytes, CD62P surface expression on platelets and plasma levels of IL-6 and soluble CD40L did not differ significantly between patients with stroke and controls.
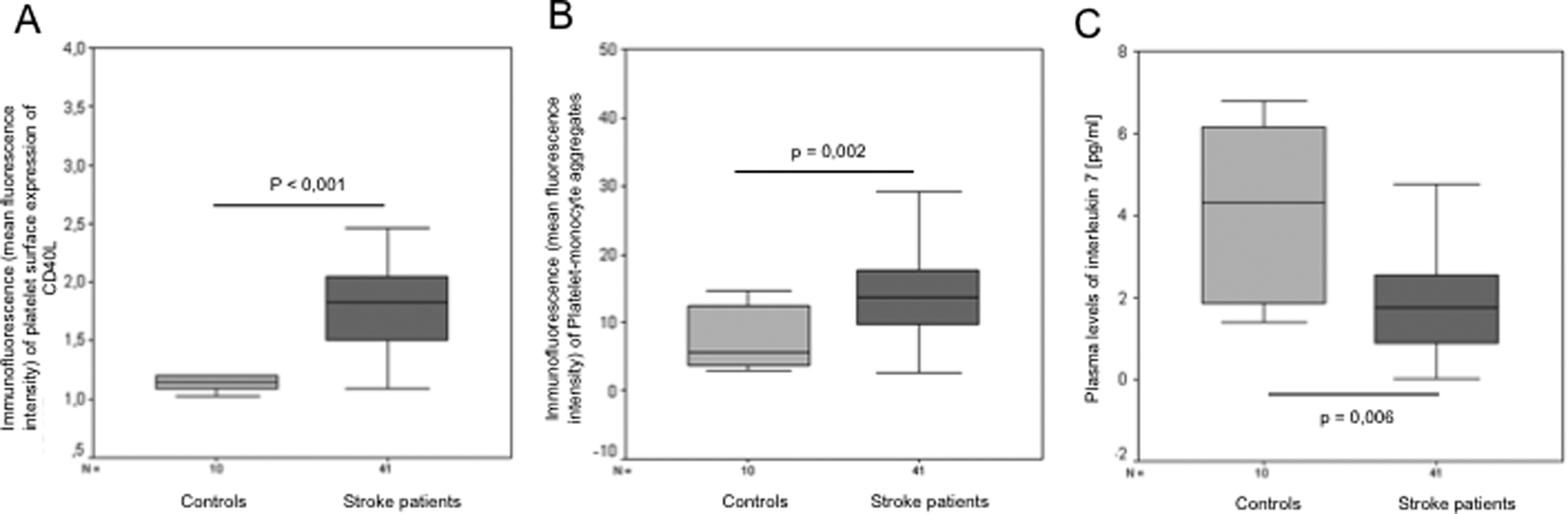
Platelet surface expression of CD40L (A) and the amount of platelet–monocyte aggregates (B) were significantly higher in patients with stroke compared to controls. Plasma levels of interleukin 7 (pg/mL) (C) were significantly lower in patients with stroke compared to controls. Data are presented as medians, 25th and 75th percentiles (boxes), and 10th and 90th percentiles (whiskers).
Subgroup analysis comparing the group of 3 patients with stroke revealed that plasma levels of soluble CD40L were significantly lower in patients with cardioembolic stroke compared to patients with large artery disease stroke (75.33 ± 30.72 pg/mL vs 165.01 ± 73.76 pg/mL; P = .047; Figure 2A). Plasma levels of soluble CD40L did not differ significantly between patients with cardioembolic and small artery disease stroke.
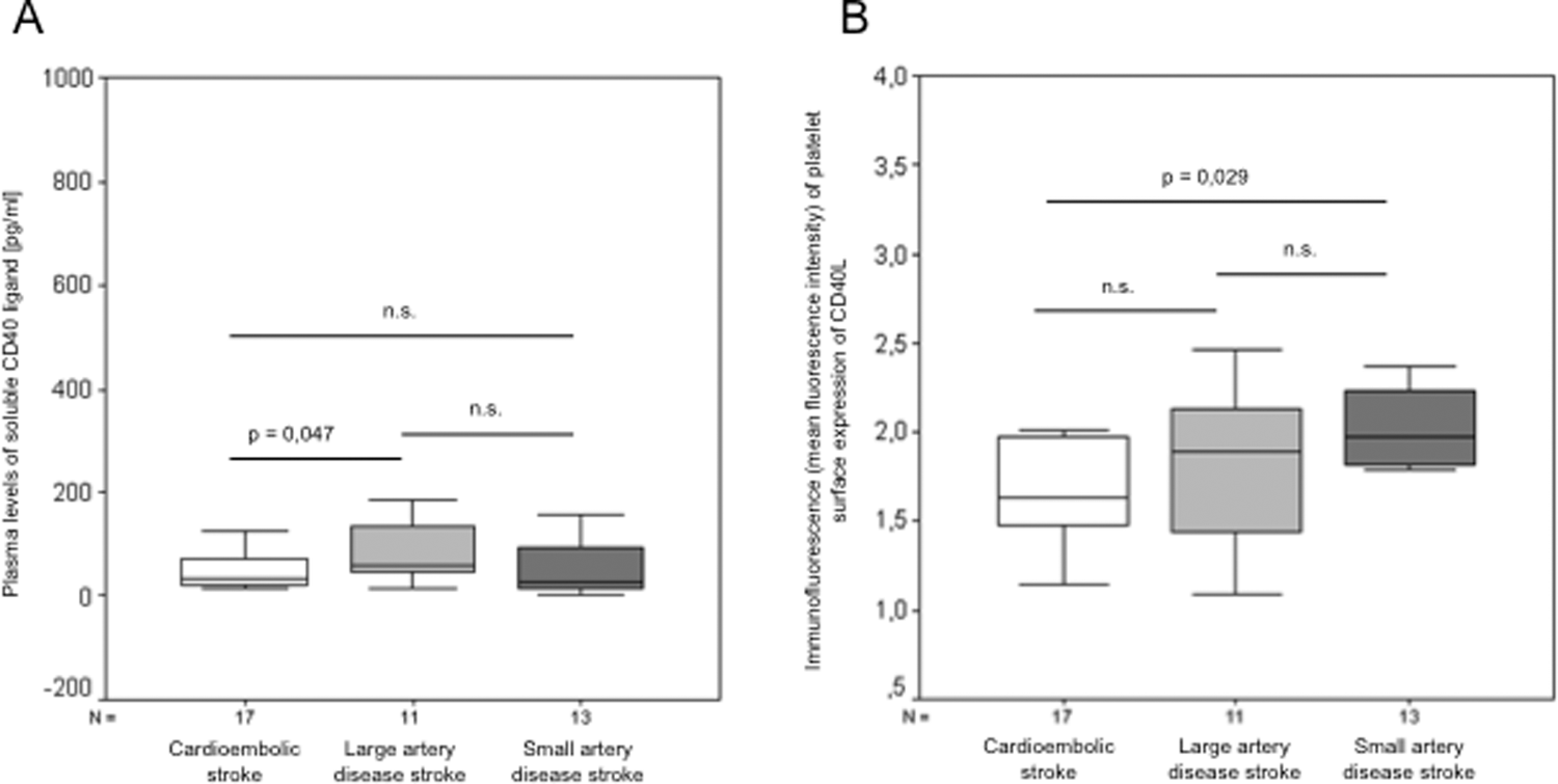
A, Plasma levels of soluble CD40 ligand (pg/mL) were significantly lower in patients with cardioembolic stroke compared to patients with ischemic stroke originating from large or small artery diseases. B, Platelet surface expression of CD40L was significantly higher in patients with small artery disease stroke than in patients with cardioembolic stroke but did not differ significantly between patients with cardioembolic stroke and large artery disease stroke. Data are presented as medians, 25th and 75th percentiles (boxes), and 10th and 90th percentiles (whiskers).
Platelet surface expression of CD40L did not differ significantly between patients with cardioembolic and large artery disease stroke and between patients with large and small artery disease stroke but was significantly higher in patients with small artery disease stroke than in patients with cardioembolic stroke (2.08 ± 0.16 vs 1.81 ± 0.16; P = .029; Figure 2B). Individual subgroup analysis primarily regarding stroke dimension rather than stroke etiology revealed a significant difference between lacunar (mainly based on small artery disease) and territorial (mainly based on large artery disease) stroke patients with regard to platelet surface expression of CD40L (2.04 ± 0.16 vs 1.55 ± 0.08; P = .014).
Discussion
Activated platelets and monocytes play an essential role in atherogenesis and are regarded cellular mediators of atherosclerosis.18,24–26 Predominantly under chronic inflammatory conditions, the release of several factors affecting vascular pathology is observed upon platelet and monocyte activation.19,25–28 However, most previous studies on platelet and monocyte activation in atherosclerosis mainly studied patients with cardiovascular diseases. Particularly in patients with acute coronary syndromes, significantly increased platelet and monocyte activation is common and well described.5,16 But beyond that, cerebrovascular atherosclerosis with acute ischemic stroke represents a common and challenging disease with high morbidity and mortality.1,2 Since the etiology of acute ischemic stroke varies distinctly, this study attempted to investigate platelet and monocyte activation with particular interest in acute ischemic stroke subtypes.
Garlichs et al were among the first to demonstrate that patients with acute stroke had higher levels of CD40L than controls. 16 In a more recent study by Tuttolomondo et al, in which patients with stroke were examined on TNF-α, plasminogen activator inhibitor 1 (PAI-1) and tissue plasminogen activator (tPA), Interleukin-1 beta (IL-1β), TNF-β, IL-6 and IL-10, E-selectin, P-selectin, soluble intercellular adhesion molecule 1 (sICAM-1), and soluble vascular cell adhesion molecule 1 (sVCAM-1), the authors could show an upregulation of various immunoinflammatory and prothrombotic markers. 29
Basically, in the present study a significant increase in platelet surface expression of CD40L and a significantly higher amount of platelet–monocyte aggregates were observed among patients with acute ischemic stroke compared to controls, thereby confirming these previous studies. Although the number of patients included with different stroke subtypes was small, the present study provides some interesting evidence inasmuch as platelet activation identified with different stroke etiologies. In stroke subgroup comparison, best association between stroke etiology and platelet activity was demonstrated by means of platelet CD40L. Highest platelet surface expression of CD40L was observed in patients with large artery disease stroke, significantly differing from patients with cardioembolic stroke. With regard to soluble CD40L, large artery disease stroke patients had significantly higher plasma levels, too.
Primarily surprising seem to be measurements of plasma levels of IL-7 in our study since plasma levels of IL-7 were significantly lower in patients with ischemic stroke than in controls. In ostensible contradiction, Cagnin and Damas demonstrated that IL-7 is upregulated among patients with cardiovascular atherosclerosis, in particular among patients with acute myocardial infarction and angina pectoris in comparison to controls.30,31 Appraising our results with lower IL-7 levels in patients with acute ischemic stroke, the role of IL-7 among cerebrovascular diseases and in cardiovascular diseases possibly seems to be contradictory. Whether this reflects a different pathomechanism or an artifact due to the small sample of patients studied needs further exploration.
In a study by Tsai et al, comparing levels of CD62P, CD63, and CD40L in acute stroke patients with patients in a convalescent stage and with controls, patients with large vessel cerebral infarction and diabetes mellitus showed a higher platelet activation and platelet–leukocyte interaction compared to patients with small vessel infarction. 22 Apparently contradictory to this publication, in our study no significant differences in platelet surface expression of CD40L between patients with large artery and small artery disease stroke were observed. Subgroup analysis regarding stroke dimension however, revealed a significantly higher platelet surface expression of CD40L in patients with lacunar stroke (based on small artery disease) than in patients with territorial stroke (based on large artery disease), probably on the basis of the fact that Tsai et al only included patients without cardioembolic stroke.
In conclusion, the results of the present study confirm and substantiate the importance of platelets and monocytes in acute ischemic atherosclerotic stroke and provide some evidence that platelet and monocyte activation differ with stroke etiology. Whether this activation is causative for or rather a consequence of different ischemic stroke etiology remains unclear and has to be further assessed in future studies.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.