
Abstract
Pharmacists were found to play a key role in anticoagulation care. In order to make an appropriate selection and counselling regarding direct oral anticoagulants (DOACs), pharmacists should be knowledgeable and abiding by evidence-based practice. We aim in this study to assess the knowledge and practices of practicing hospital and community pharmacists in Qatar regarding DOACs and their reflection on the dispensing and patient education. A prospective cross-sectional survey was developed. It included questions on demographic and professional characteristics. Additionally, it evaluated the awareness regarding safety, efficacy, and dispensing of DOACs. Lastly, a separate question was used to address the participant’s satisfaction with their knowledge. A total response were received from 211 pharmacists participating in the survey. Overall awareness score was moderate (41.6% ± 26%). These scores were in alignment with participants’ self-satisfaction with knowledge on DOACs (72% of participants were not satisfied). Being a clinical pharmacist, of male gender, and with a board certification were factors associated with increased awareness on DOACs. Results from this survey point to the importance of having more educational activities in order to improve pharmacist’s knowledge of DOACs.
Introduction
Warfarin, which is a vitamin-K antagonist (VKA), has been the mainstay oral anticoagulant (OAC) used in both treatment and prevention of various thromboembolic disorders for more than 7 decades. 1 Warfarin has a wide range of food and drug interactions, unpredictable pharmacokinetics, narrow therapeutic index, and inter- and intra-patient variability. All these factors have made warfarin a very challenging medication and one that requires frequent monitoring. 2 Anticoagulation management services (AMS) were developed to improve warfarin management. Pharmacist-led AMS has been shown to improve patient’s quality of life, reduce anticoagulation monitoring, and provide a high level of anticoagulation control and patient’s satisfaction. 3 –5
Direct oral anticoagulants (DOACs) were introduced in 2010 and are still considered a relatively new class of non-VKA OACs. Dabigatran, a direct thrombin inhibitor, was the first DOAC to be introduced and was followed by four-factor Xa inhibitors (rivaroxaban, apixaban, edoxaban, and betrixaban). 1 Having rapid onset of action, predictable therapeutic effect, fixed-dose regimens, and less frequent monitoring made DOACs an attractive therapeutic option for both health care providers and patients. 6 Direct oral anticoagulants, however, are not without limitations. They have a short half-life (not the best option for patients with poor adherence), may increase gastrointestinal bleeds (especially dabigatran and rivaroxaban), need dose adjustments in renal impairment and elderly patients, and are contraindicated in pregnant and breastfeeding women. 1,7 Last but not least, their use is contraindicated in mechanical heart valve. 8
Similar to the role of pharmacists in warfarin management, pharmacist-led AMS are thought to play a significant role in DOACs patient’s education, monitoring, and adherence. A large multisite study involving 67 Veterans Health Administration sites found that pharmacist-led dabigatran monitoring had the tendency to improve patient adherence. 9 More recently, a retrospective analysis of all DOACs prescription within the University of Michigan Health System found that pharmacist-led DOACs service increased appropriate dosing, follow-up, and patient adherence to DOACs. 7
Since the introduction of DOACs to the market, anticoagulation management has encountered significant changes. Current practice guidelines such as CHEST guidelines suggest DOACs over warfarin in both non-valvular atrial fibrillation and non-cancer venous thromboembolism patients. 2,10 Similarly, the American College of Cardiology, American Heart Association, and Heart Rhythm Society (AHA/ACC/RHS) suggest DOACs over warfarin in patients who are eligible to DOACs and unable to maintain therapeutic international normalized ratio. 11
Direct oral anticoagulants were introduced in Qatar in 2011, and currently, dabigatran, rivaroxaban, and apixaban (added in June 2019) are all available on the formulary. Our group has shown that there has been a significant increase in the DOACs use reaching 23% of all OACs in 2015. 12 However, further data analysis showed that DOACs were not always appropriately prescribed. 6 To understand this better, we administered a survey to 175 physicians in Qatar and it showed that they have moderate awareness on DOACs. 1 With the important role of the pharmacist in DOACs prescribing, monitoring, and counseling, we sought to conduct an additional survey to assess the knowledge and attitude of pharmacists regarding DOACs to identify any potential gaps.
Methods
Study Design and Population
This is a descriptive, cross-sectional survey study performed through the administration of a Survey Monkey online questionnaire (www.surveymonkey.com). The study took place over 3 months from January 2018 to March 2018. Eligible participants included all pharmacists currently practicing at Hamad Medical Corporation (HMC) or the community pharmacies in Qatar. Subjects from all facilities were approached with repeated reminders. A sample of convenience was collected.
Study Settings and Ethics Approval
The study was conducted in 5 hospitals of HMC in Qatar, which includes Hamad General Hospital, Al-Wakra General Hospital, Heart Hospital, Al-Rumailah Psychiatry Hospital, and Al-Amal Oncology Hospital in addition to a chain of community pharmacies. The study was approved by Hamad Medical Corporation’s institutional review board.
Sample Size Calculation
The sample size was calculated using Raosoft online calculator (https://www.roasoft.com). Given that the Pharmacist population size at HMC and the community pharmacy chain is about 450 to 500 and to achieve a confidence (power) level of 90%, with a margin error of 5% and considering a 50% response distribution, a sample size of 170 participants was found to be adequate. Considering 25% nonresponse rate, we aimed to recruit 190 participants.
Validation and Piloting
Structure and content of the survey were checked for validity (to ensure it produces true results) by 3 senior pharmacists (one of them is a community pharmacy expert and the others are hospital pharmacist supervisors), 3 clinical pharmacy specialist (2 of them with cardiovascular disease expertise), and internal medicine senior consultant. Modifications were made based on feedback provided. A pilot version was tested on randomly selected 10 subjects with different working areas and years of experience. Respondents found the questionnaire clear and concise.
Survey Development
The survey was designed based on the literature review of the effect of pharmacist knowledge and attitude regarding DOACs and its impact on their dispensing and patient education pattern. The survey was composed of 4 domains: (a) demographic and professional characteristics of the participants; (b) evaluating awareness regarding DOACs safety profile; (c) evaluating awareness regarding DOACs efficacy profile; and (d) evaluating the counselling (dispensing) pattern of DOACs. Under the safety domain, 10 questions were designed to assess the general awareness on the safety of DOACs in comparison with warfarin. Under the efficacy domain, the awareness of participants regarding the efficacy of DOACs was assessed using 11 questions. The last domain had 5 questions to assess the pharmacist awareness on DOACs counselling and dispensing of DOACs, and 1 question regarding the percentage of DOACs dispensed by participating pharmacists among patients requiring anticoagulation (Table 1). Responses were on a 3-point Likert scale ranging among (Disagree, Don’t know, and Agree). The last question, however, was a score ranging from 0% to 100%.
Survey Awareness Domains, Questions, and Responses.a
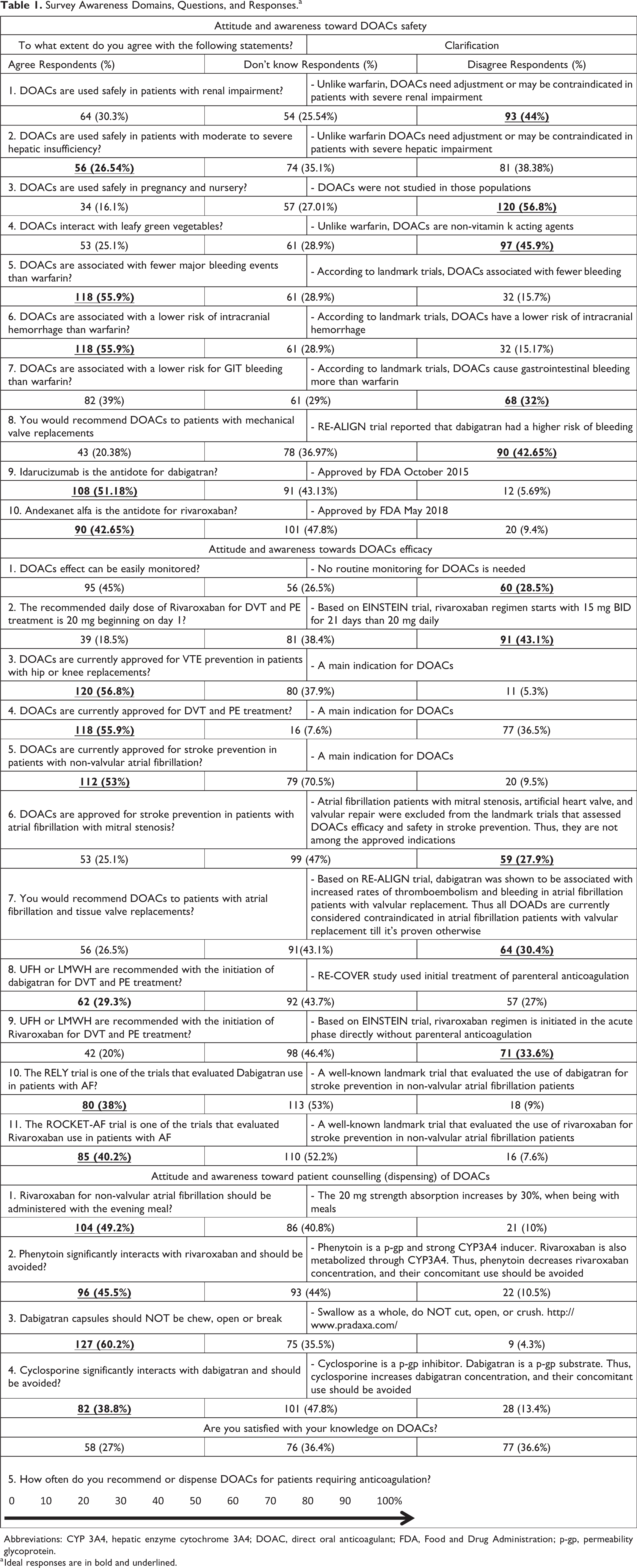
Abbreviations: CYP 3A4, hepatic enzyme cytochrome 3A4; DOAC, direct oral anticoagulant; FDA, Food and Drug Administration; p-gp, permeability glycoprotein.
a Ideal responses are in bold and underlined.
Measured outcome and statistical analysis
Descriptive and inferential statistical analyses were applied to the collected data using IBM Statistical Package for Social Sciences (IBM SPSS 25 software; IBM). All variables were categorical including participants’ demographics, professional information, as well as their responses to questions assessing their knowledge and attitude toward the DOACs and were expressed as frequencies and percentages. Awareness score of 1 point was provided if the respondent agreed on true statements or disagreed on false statements and a score of 0 point, otherwise. This was done for all questions in the 3 domains except for the last question, which was a score rating the percentage of patients dispensed DOACs by each participant per week from the total weekly prescriptions of OAC. The percentage awareness score (PAS) was calculated by dividing the participant score in each domain by the number of questions in that perspective domain (the maximum possible score) and multiplying the result by 100. PAS was expressed as mean (± SD). Overall PAS was the sum of PAS in each domain. T test was used to test the effect of the profession as well as other demographic and professional parameters on the PAS. Analysis of variance test was used to test the effect of age categories on the PAS. A level of significance was set a priori at P ≤ .05.
Results
Participants’ Characteristics
Over 3 months period, 400 participants were approached among which 211 participated in the survey (response rate = 52.7%). Participants answered all survey questions (Table 1). More than half of the participants (54%) were male, and about half of them (53.6%) were middle age (35 years of age or younger). Forty-seven pharmacists were clinical pharmacists (22.4%) with the remaining hospital pharmacist (54%) and (23.6%) community pharmacists. Fifty-five percent (55%) of the respondents were in practice for more than 10 years. Thirteen percent of the participants were board-certified (Table 2).
Participants Baseline and Professional Characteristics.

Evaluating Awareness Regarding DOACs
Awareness of pharmacist toward DOACs was assessed from different domains perspective (safety, efficacy, patient counselling, and dispensing). Participants’ responses are reported in Table 1. Overall PAS was moderate (41.6% ± 26%), lowest (39.6% ± 29%) for awareness on efficacy, and highest (44.4% ± 36%) for awareness on counselling (Table 3). Interestingly, these scores were in alignment with participants’ self-satisfaction with knowledge on DOACs (72% of participants were not satisfied). Being a clinical pharmacist, male and board-certified were factors significantly associated with higher PAS (Table 4). Age and years of experience did not show any significant effect on overall awareness. Additionally, pharmacists dispensing less than 50 DOACs prescription per week had significantly lower PAS score in the dispensing domain compared to the high DOAC dispensing pharmacists (50 prescriptions or more; 39.1 ± 27 vs 49.9 ± 21, P = .006).
Tested Domains and Scores.

Abbreviation: PAS, percentage awareness scores.
Effect of Baseline and Professional Characteristics on AS.a
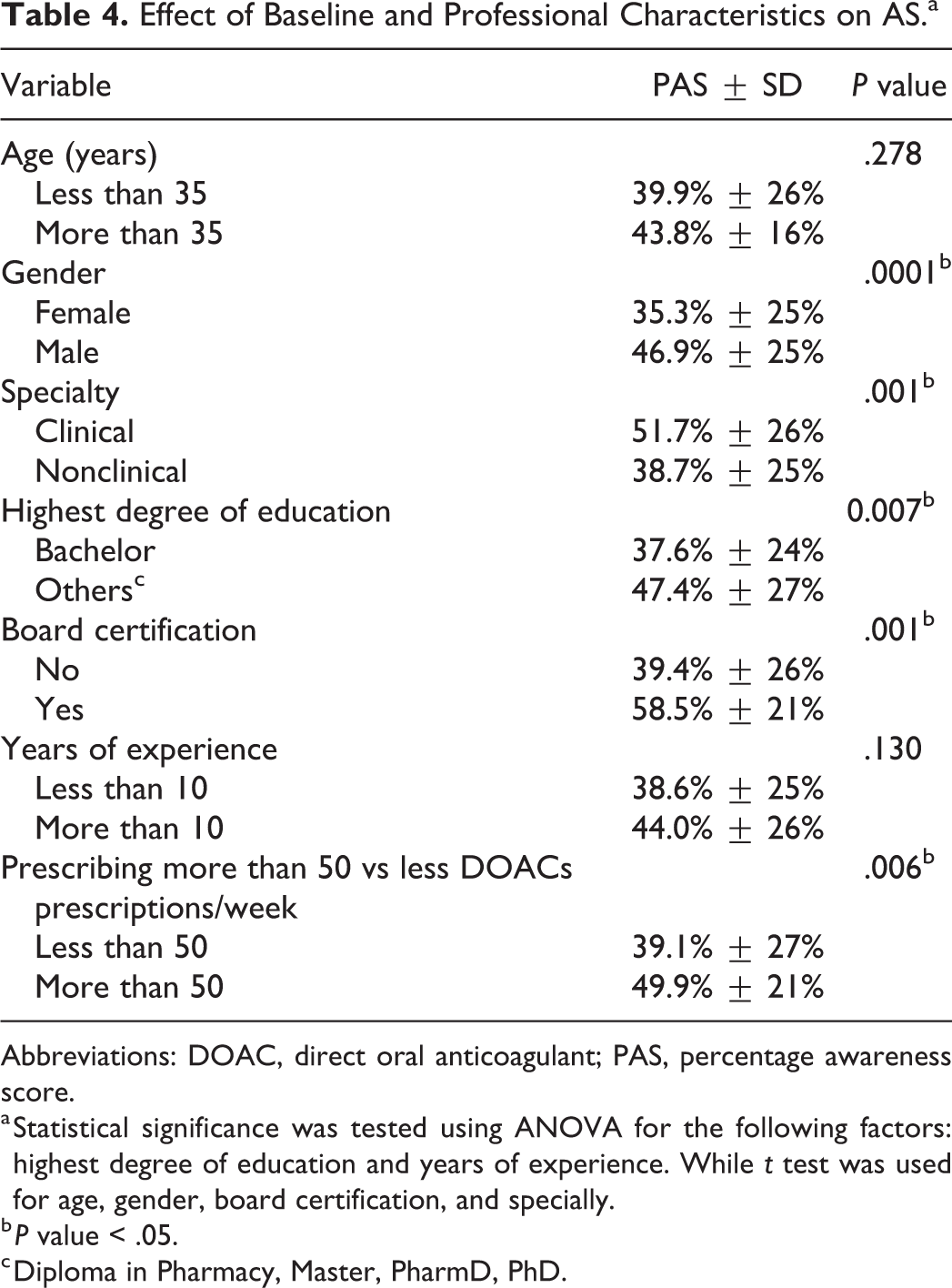
Abbreviations: DOAC, direct oral anticoagulant; PAS, percentage awareness score.
a Statistical significance was tested using ANOVA for the following factors: highest degree of education and years of experience. While t test was used for age, gender, board certification, and specially.
b P value < .05.
c Diploma in Pharmacy, Master, PharmD, PhD.
Discussion
Pharmacists play an integral role in the counseling, dispensing, and monitoring of drug’s efficacy and safety. 13 Additionally, they are considered the last line of defense against potential medication errors in the outpatient setting. In this study, we attempted to assess the knowledge and attitude of pharmacists on DOACs in Qatar and their self-satisfaction with current knowledge through a cross-sectional survey. The survey revealed that pharmacists have moderate awareness of DOACs with the majority not being satisfied with their current knowledge.
Although previous studies assessed pharmacist confidence toward OAC, only a few studies evaluated pharmacist knowledge and awareness. Sandhu et al aimed to assess the appropriateness and barriers to prescribing OAC by pharmacists for AF using hypothetical scenarios. 3 Lacking knowledge on DOACs among participants reached 35%. Additionally, 25% of the participants were not confident in prescribing DOACs. 3 Similarly, Papastergiou and his colleagues reported in an international pharmacist survey in 2017 a significant difference in confidence upon dispensing warfarin versus DOACs. 4 As expected, the study also revealed that pharmacists with clinical experience (carrying a board certification, being involved in more DOACs prescribing or dispensing) had better awareness. In the same line, Ashjian et al evaluated the impact of a pharmacist-led AMS and found that clinical pharmacist played a vital role in selecting, optimizing, and educating patients on DOACs. 7
One may argue that pharmacists are not expected to know all pieces of information on drugs in an individual therapeutic class. However, OACs are high-alert medications and should be managed with more caution and awareness. Direct oral anticoagulant agents have also increased through a short period of time starting with a sole agent in 2010 growing up to 5 agents at the time being. Additionally, having different dosing regimens in certain populations and lacking head-to-head trials to discriminate DOACs from each other warrant in-depth knowledge about this therapeutic class. 14 One of the limitations that were faced in this study is that our surveyed sample did not adequately represent all pharmacists in Qatar. Majority of the participants were hospital pharmacists which limit its external validity. Lastly, survey instruments that use Likert-scale are prone to central tendency bias (choosing “neutral/ don’t know” answers). 15 However, majority of our questions had a low percentage of these types of answers which likely reduce the impact of this type of bias.
Conclusion
In conclusion, this survey indicates that pharmacists have moderate awareness on DOACs. Clinical and practical experiences were the most important factors associated with enhanced DOACs’ awareness. Future work should focus on reassessing pharmacists’ knowledge after providing well-designed educational campaigns.
Footnotes
Authors’ Note
Ahmed El-Bardissy and Hazem Elewa have contributed equally to the paper. This work has been presented at AC Forum meeting in 2019: Assessing pharmacists’ knowledge and attitude toward the direct oral anticoagulants in Qatar. AC forum conference, April 11-13, 2019, Fort Lauderdale, FL, USA
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication of this article was funded by the Qatar National Library.