
Abstract
Direct oral anticoagulants (DOACs) are more commonly prescribed since their introduction. Reports on inappropriate prescribing have been observed which may indicate poor awareness on these agents. In this study, we aim to evaluate the extent of the physicians’ knowledge on DOACs and its possible impact on physicians’ confidence to prescribe these medications. A prospective cross-sectional survey was developed based on the literature review. Eligible participants were physicians and surgeons currently practicing at Hamad General Hospital in Qatar. The survey included questions on demographic and professional characteristics. It also evaluated the awareness and attitudes regarding safety, efficacy, and prescribing of DOACs. Over 6-month period, 175 practitioners responded to the survey. Overall awareness score was moderate (61% ± 18%). These scores were in alignment with participants’ self-satisfaction with knowledge on DOACs (66% were not satisfied) and participants’ confidence toward prescribing DOACs (48% were not confident). Age, degree of education, and years of experience had significant positive influence on awareness score. This survey indicates that practitioners have moderate awareness on DOACs. Future work should focus on reassessing practitioners’ knowledge after providing well-designed education campaigns
Introduction
For almost 80 years, warfarin has been the mainstay anticoagulant used in both treatment and prevention of various thromboembolic disorders such as atrial Fibrillation (AF), prosthetic heart valve, and venous thromboembolism (VTE). 1 Being the only oral anticoagulant for such duration created an in-depth knowledge, experience, and understanding of its clinical applications, management, and associated risks. However, its narrow therapeutic index, inter, and intrapatient variability led sometime to treatment failure or life-threatening adverse reactions that remain unexplained. 2,3
Direct oral anticoagulants (DOACs) were introduced in 2010, with dabigatran—a direct thrombin inhibitor—followed by 4 factor Xa inhibitors (rivaroxaban, apixaban, edoxaban, and betrixaban). 1 Accumulated data from clinical trials and meta-analyses have shown that DOACs are noninferior to warfarin in stroke prevention for nonvalvular AF (NVAF), VTE, and recurrent VTE. 4 This has led to major changes in anticoagulation management. 5,6
DOACs have practical advantages over warfarin including administration in fixed dosing, lack of frequent monitoring requirement, fewer drug, and food interactions, reduced risk of intracranial hemorrhage, and major bleeding. 1,4 Despite the advantages of DOACs over warfarin, those agents are not favorable in all patients, since they can increase the risk of gastrointestinal bleeding (especially rivaroxaban and dabigatran) and lack antidote (except for dabigatran). 6 Additionally, DOACs are not recommended or even contraindicated in certain situations. For example, DOACs are contraindicated in pregnant, lactating females, patients on renal dialysis, and those with advanced renal impairment. Limited data also support their use in morbidly obese patients. 7,8 Finally, cost-effectiveness of DOACs compared to warfarin remains an issue and totally depends on the health-care system strategy for each country. 9 –11
DOACs were introduced in Qatar in 2011, and currently, dabigatran and rivaroxaban are the only available agents on formulary at Hamad Medical Corporation (HMC), which is the main medical institution in the country. Our group has previously reported that over the 5-year period from 2011 till 2015, there has been a significant increase in the trend of usage of DOACs that reached 23% of all oral anticoagulants in 2015. 6 However, in a further analysis of this data, we have shown that DOACs were not always appropriately prescribed. 1
To find out more about the reason for this inappropriate prescribing, we aim in this study to assess the knowledge and attitude of physicians from different specialties regarding DOACs and their reflection on their prescribing pattern.
Methods
Study Design and Population
A descriptive, cross-sectional survey using a self-administered questionnaire. The study took place over 6 months from December 2016 to June 2017. Eligible participants included all authorized physicians to prescribe anticoagulation at Hamad general hospital (HGH). Those who are not permitted to prescribe were excluded. The survey was hand-delivered by one of the investigators, and an introductory invitation cover page was attached explaining the purpose and objectives of the survey and assuring the anonymity of the participant’s identity. The participants were approached based on sample of convenience.
Study Settings and Ethics Approval
The study was done at HGH which is a 603-bed tertiary teaching hospital in Qatar. The hospital covers all specialties except hematology–oncology and obstetrics. The study was approved by Hamad Medical Corporation’s Institutional Review Board (HMC-IRB).
Sample Size Calculation
The sample size was calculated using Raosoft online calculator (www.roasoft.com)Given that the population size of medical practitioners in Qatar is 900, and to achieve a power of 80% with a margin of error of 5% and considering a 50% response distribution, a sample size of 140 participants was found to be adequate. Considering a 30% nonresponse rate, we aimed to recruit 175 participants.
Validation and Piloting
Structure and content of the survey were checked for validity (to ensure it produces true results) by 2 senior faculty members (one with expertise in surveys and pharmacy practice research and the other with clinical knowledge and teaching experience in clinical pharmacy), one clinical pharmacy specialist (with cardiovascular expertise), and internal medicine senior consultant. Modifications were made based on feedback provided. A pilot version was tested on randomly selected 10 participants with different specialties and years of experience. Respondents found the questionnaire clear and concise.
Survey Development
The survey was designed based on literature review on the effect of physician knowledge and attitude regarding DOACs and its impact on their prescribing pattern. The survey was composed of 4 domains (1) demographic and professional characteristics of the participants; (2) evaluating awareness regarding DOACs safety profile; (3) evaluating awareness regarding DOACs efficacy profile; and (4) evaluating the prescribing pattern of DOACs. Under the safety domain, 6 questions were designed to assess the general awareness on the safety of DOACs in comparison to warfarin. Under the efficacy domain, the attitude of participants regarding the efficacy of DOACs was assessed using 7 questions. The last domain had 7 questions to measure the physicians’ prescribing pattern of DOACs and 1 question regarding the percentage of DOACs prescribed by participating physicians among patients requiring anticoagulation (Table 1).
Survey Awareness Domains, Questions, and Responses.
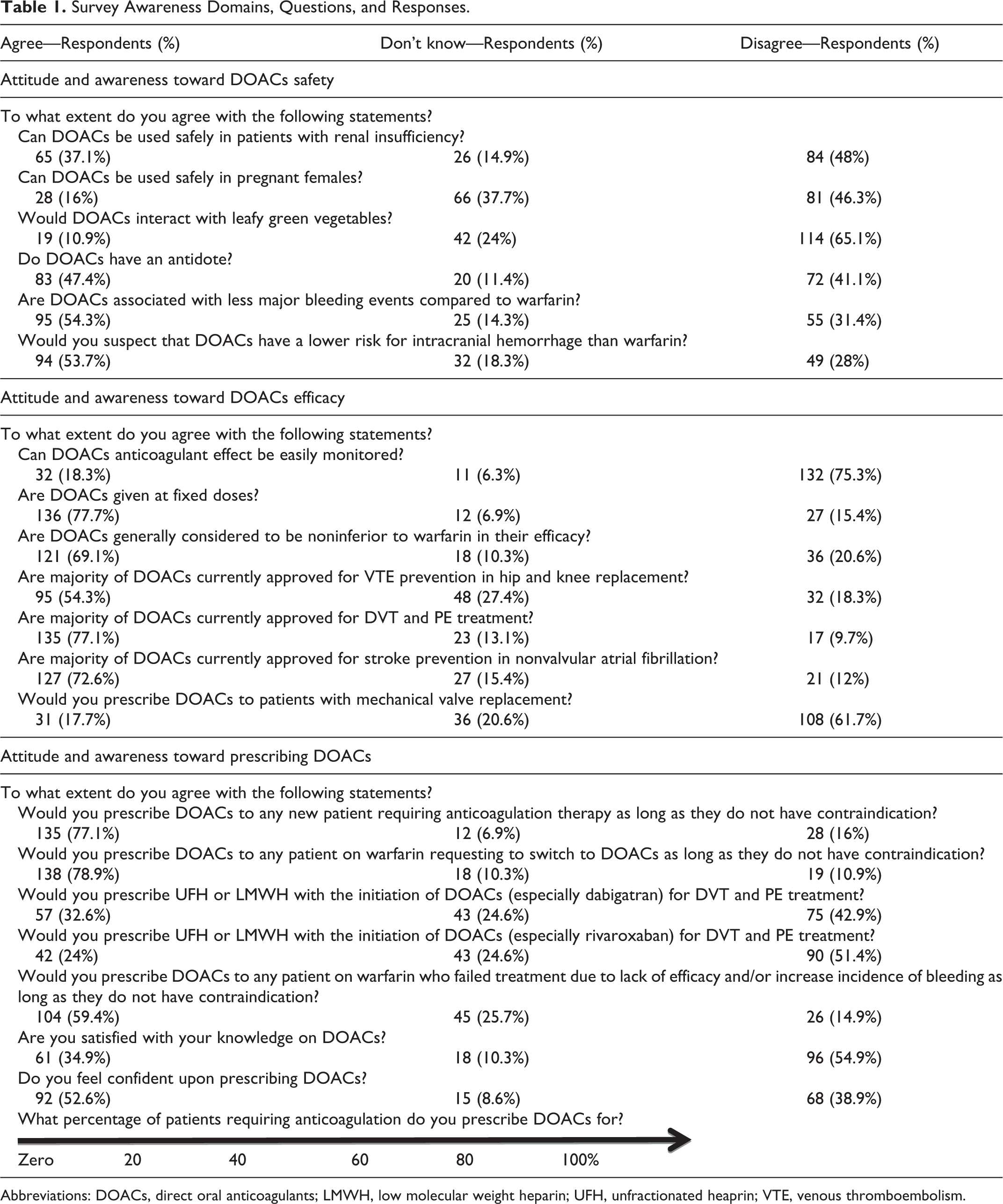
Abbreviations: DOACs, direct oral anticoagulants; LMWH, low molecular weight heparin; UFH, unfractionated heaprin; VTE, venous thromboembolism.
Responses were on a 3-point Likert-type scale (disagree, don’t know, and agree). The last question, however, was score ranging from (0% to 100%) with 20% intervals to rate the percentage of patients prescribed DOACs by the physicians.
Measured Outcome and Statistical Analysis
Descriptive and inferential statistical analyses were applied to the collected data using IBM Statistical Package for Social Sciences (IBM SPSS 24 software; IBM, New York). All variables were categorical including participants’ demographics, professional information as well as their responses to questions assessing their knowledge and attitude toward the DOACs and were expressed as frequencies and percentages. Awareness score of 1 point was provided if the respondent agreed for true statements or disagreed for false statements and a score of zero point otherwise. This was done for all questions in the 3 domains except for the last question which was a score rating the percentage of patients prescribed DOACs by each participant. The percentage awareness score (PAS) was calculated by dividing the participant score in each domain by the number of questions in that perspective domain (the maximum possible score) and multiplying the result by 100. Percentage awareness score was expressed as mean ( standard deviation). Overall PAS was the sum of PAS in each domain. The t test was used to test the effect of the profession as well as other demographic and professional parameters on the PAS. Analysis of variance test was used to test the effect of age on the PAS. A level of significance was set a priori at P ≤ .05.
Results
Participants’ Characteristics
Over 6-month period, 300 participants were approached among which 175 participated in the survey (response rate = 58.3%). Participants answered all survey questions. Majority (83.4%) of the participants were male, and about half (57.7%) of them were middle age (35 years of age or younger). One hundred fourteen (65%) physicians were internal medicine with the remaining from other specialties. Almost half of the respondents were residents (45.7%) while the remaining were consultants and fellows (31.4% and 22.9%, respectively). Almost half of the participants were board certified (45.7%; Table 2)
Participants Baseline and Professional Characteristics.a
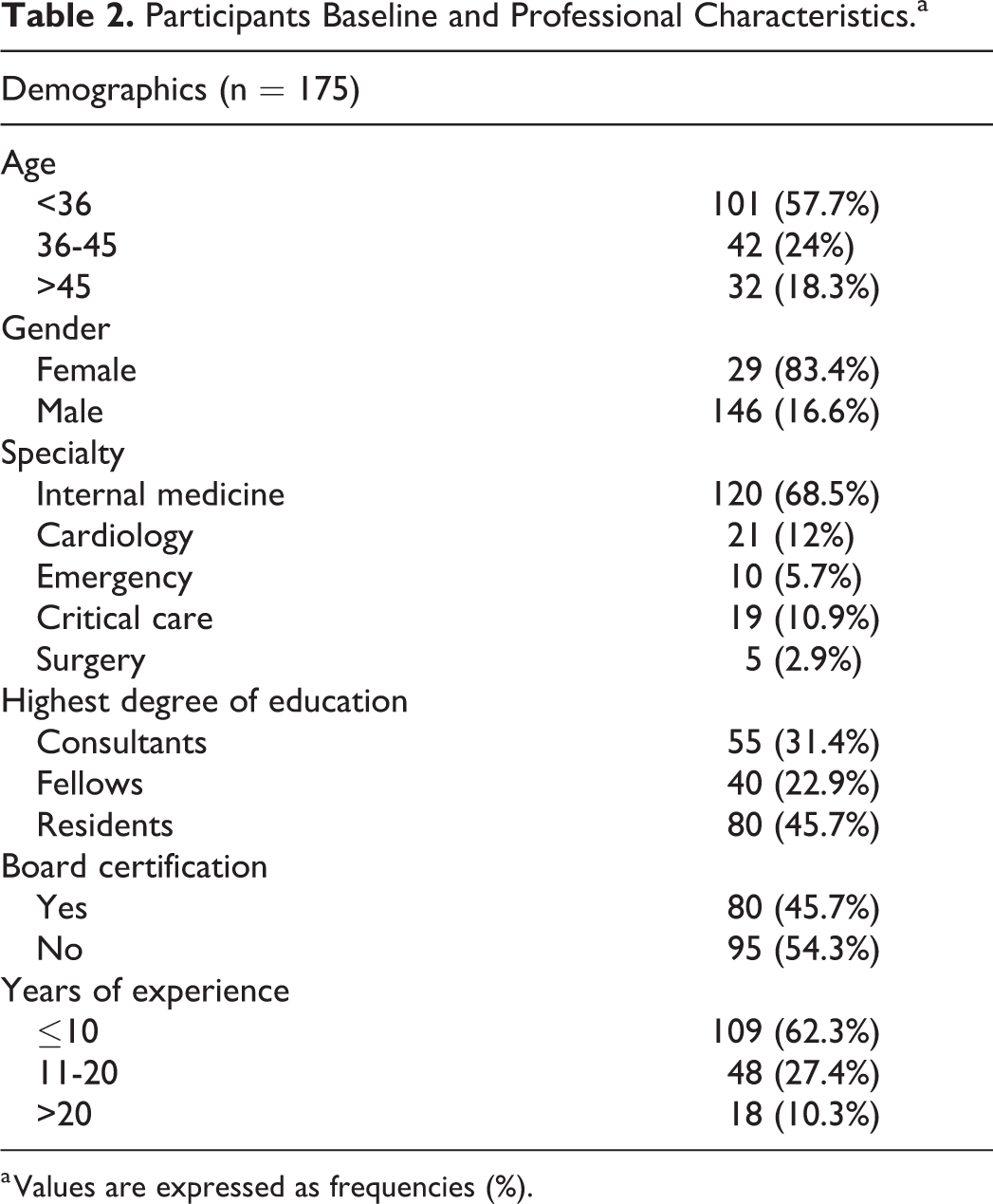
a Values are expressed as frequencies (%).
Evaluating Awareness Regarding DOACs
Awareness of physicians toward DOACs was assessed from different domains perspective (safety, efficacy, and prescribing). Participants’ responses are reported in Table 1. Overall PAS was moderate (61% ± 18) and was lowest (52% ± 25) for awareness on safety and highest for awareness on prescribing (71% ± 24; Table 3). Interestingly, these scores were in alignment with participants’ self-satisfaction with knowledge on DOACs (66% were not satisfied; Figure 1) and participants’ confidence toward prescribing DOACs (48% were not confident; Figure 2). As expected, age, degree of education, and years of experience had significant positive influence on PAS (Table 4). About two-third (59.3%) of the physicians were found to prescribe DOACs for 20% or less of their patients who require anticoagulation (Figure 3). When comparing the prescribing PAS score of the low DOAC prescribing physicians (20% or less) to the high DOAC prescribing physicians (40% or more), we did not find any significant difference (61.7 ± 22.5 vs 57.9 ± 21.9; P = .29).
Tested Domains and Scores.a
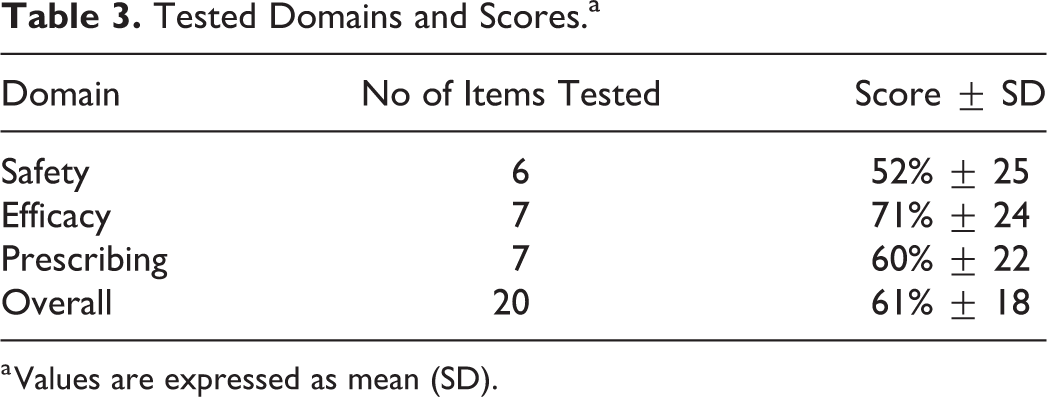
a Values are expressed as mean (SD).
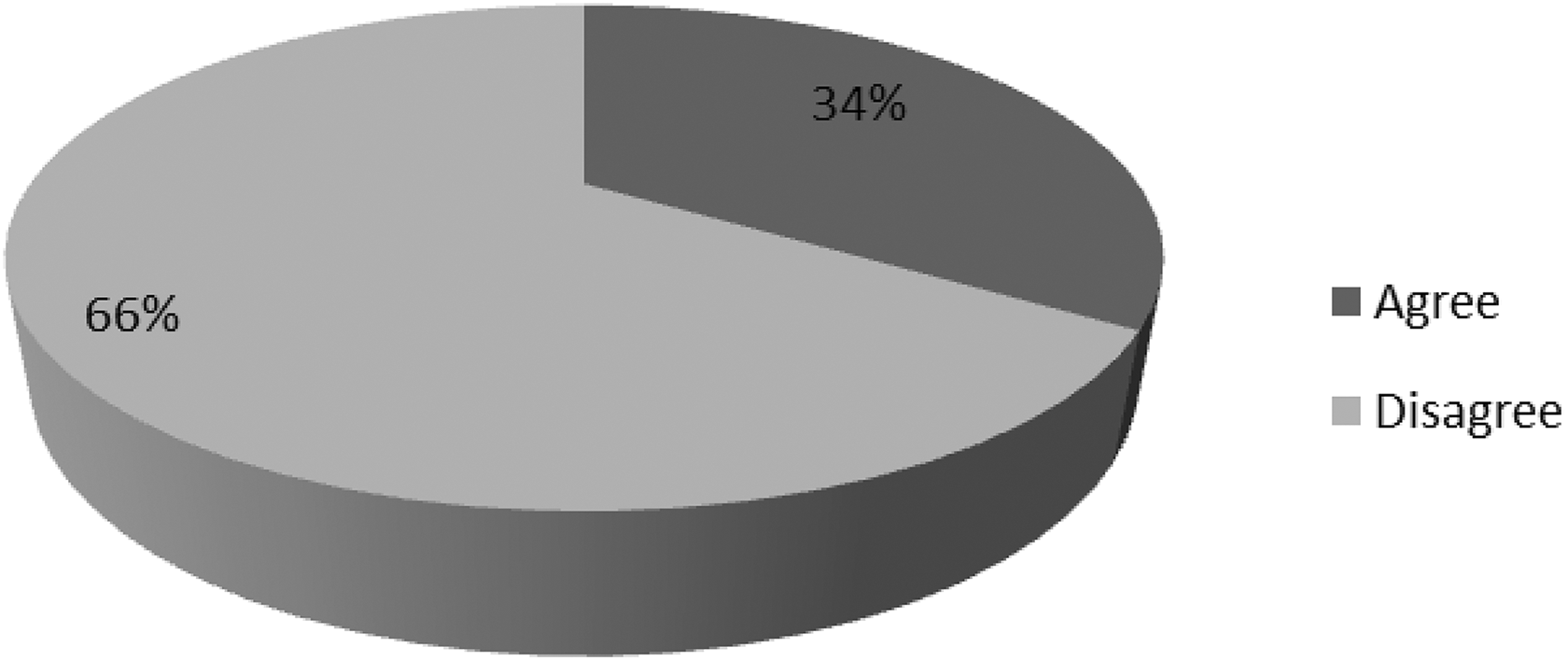
Participants satisfaction with their knowledge regarding direct oral anticoagulants.
Participants confidence upon prescribing direct oral anticoagulants.
Effect of Baseline and Professional Characteristics on Percentage Awareness Scores.a
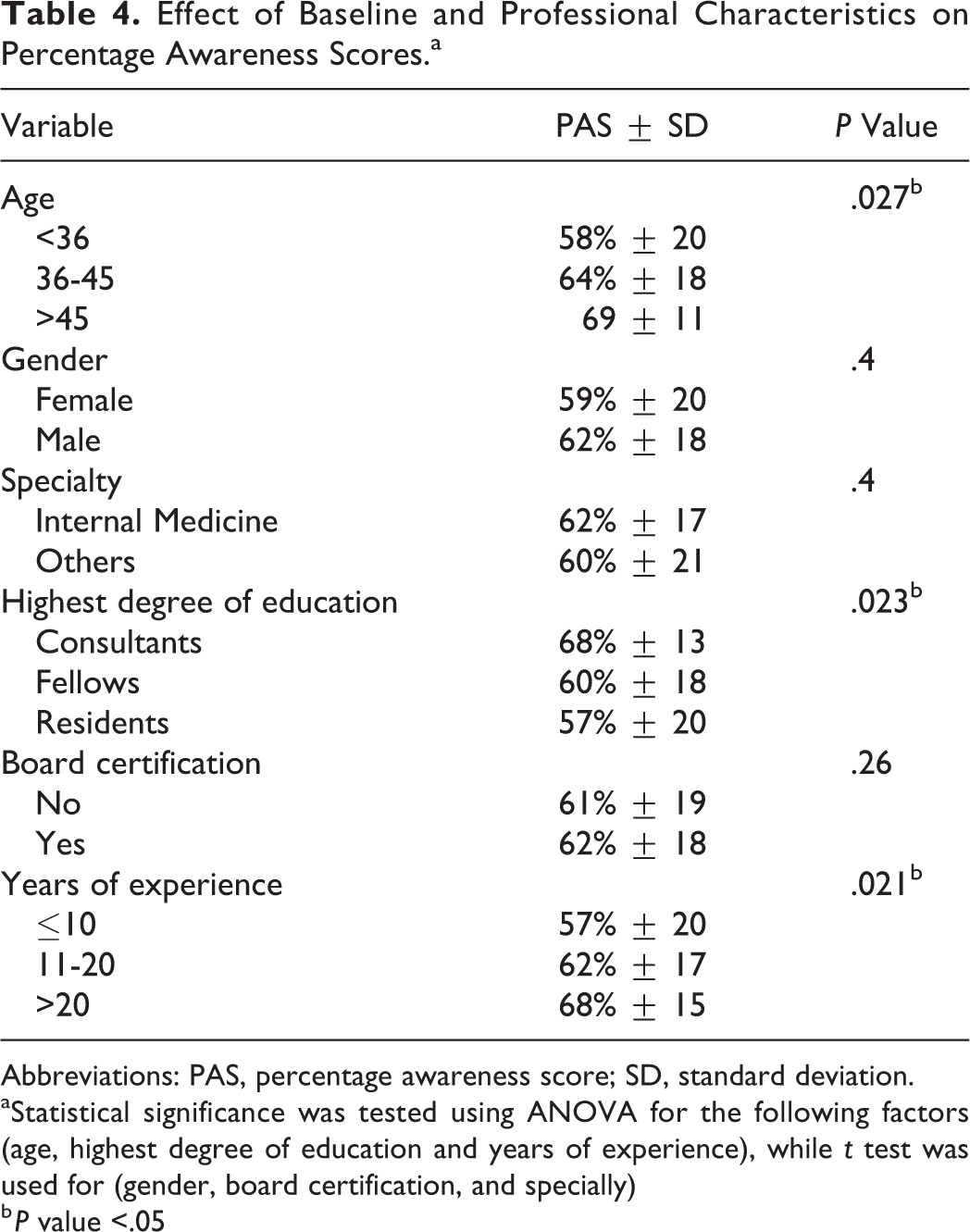
Abbreviations: PAS, percentage awareness score; SD, standard deviation.
aStatistical significance was tested using ANOVA for the following factors (age, highest degree of education and years of experience), while t test was used for (gender, board certification, and specially)
b P value <.05
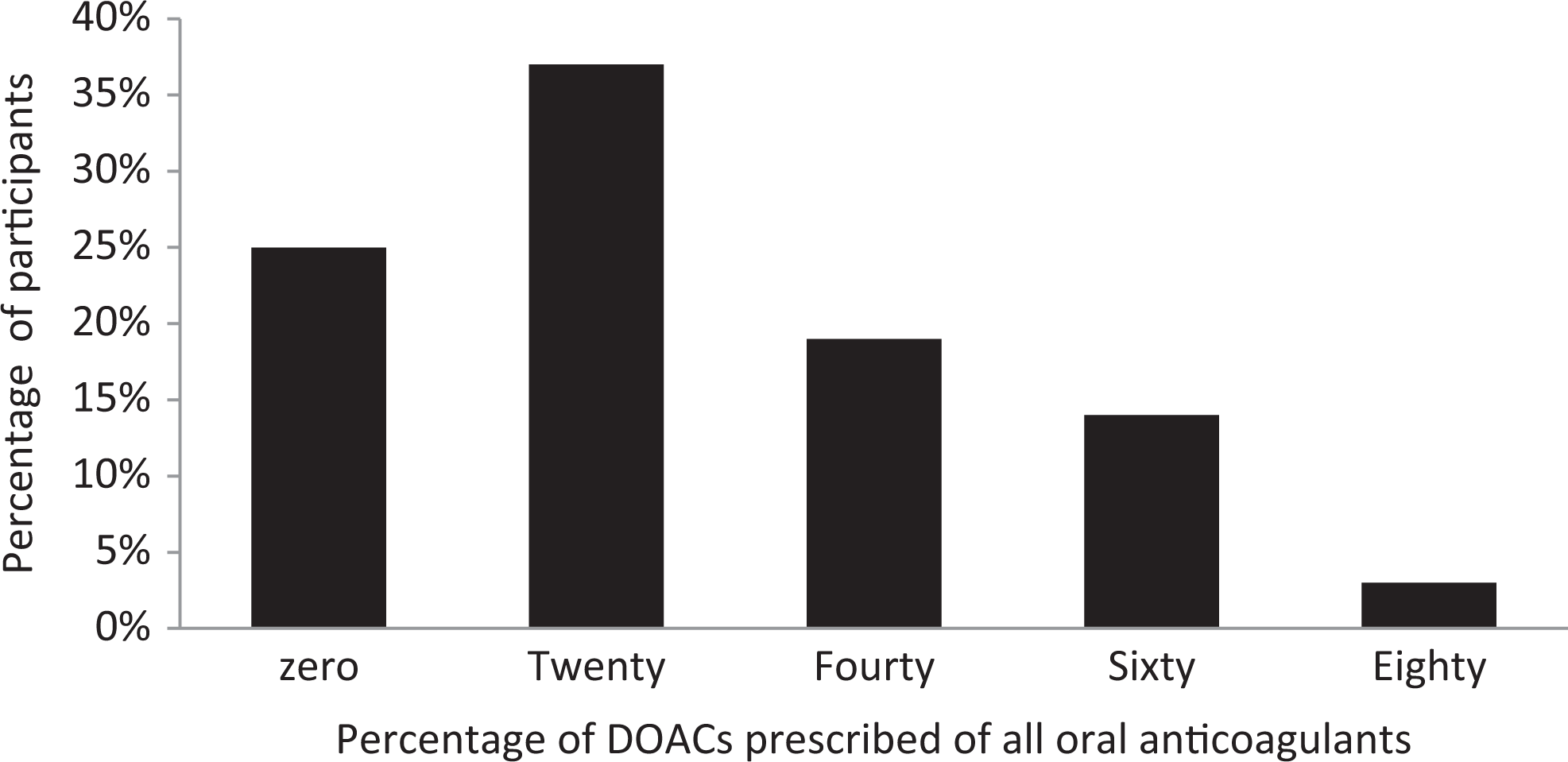
Extent of DOACs prescribed by participants for patients requiring oral anticoagulants. DOACs indicate direct oral anticoagulants.
Discussion
In this study, we attempted to assess the knowledge and attitude of physicians on DOACs, as well as their perceived satisfaction with self-knowledge and extent of DOACs they prescribe to patients in need for oral anticoagulation. The main finding of the study was that participants’ DOACs awareness is moderate and matched their self-reported knowledge and confidence when prescribing DOACs. Although previous studies assessed physicians’ attitude toward DOACs, 12 –15 only few studies have tested the prescribers’ knowledge and awareness. In 2016, Olaiya et al aimed to establish physicians’ level of awareness of the different DOACs and to assess whether prescribers can recognize the level of anticoagulation in a hypothetical scenario. 16 Awareness on DOACs ranged from 50%to 88%. Additionally, recognizing the harm that could occur from performing an invasive procedure in a hypothetical clinical scenario was recognized by only 55% to 58%. These results seem to be in alignment with the current survey and yield the same conclusion. The declined level of awareness noted in this study also strongly explains our group’s recent findings on the increased rate of inappropriate prescribing of DOACs in the same study setting. 17 However, physicians are not expected to know all information on a drug in an individual therapeutic class; the situation is a bit different when it comes to a high alert medication class such as oral anticoagulants. Furthermore, inappropriate prescribing of DOACs (either through use of a wrong dose or for the wrong indication) can yield to major adverse events such as stroke, thrombosis, or bleeding. One thing to remember about DOACs compared to other anticoagulants is that they lack simple practical surrogate marker to use as a predictor for adverse reactions. Given the increasing number of patients using DOACs in clinical practice, prescribers’ awareness is a very important aspect to ensure patient safety. Even if an individual clinician is unable to have perfect awareness on all agents in a certain class of medications, she or he should focus at least on the agents under formulary and those that are widely used at the institution.
In addition to our main finding above, we also observed that age, years of experience, and degree of education positively correlate with awareness on DOACs. Although one would think that recent graduates may have better awareness on these recently approved medications (DOACs), it seems that practical training and higher education degree was a more important factor in determining awareness of DOACs in our setting. Unexpectedly, we also found that the awareness of the frequent DOACs prescribers was not different compared to the unusual DOACs prescribers
Last but not least, our results have shown that for majority of the respondents, DOACs are not the first choice when prescribing oral anticoagulants. This finding is confirmed by our recent research work that explored the trend of use of oral anticoagulants in Qatar and found that in 2015, warfarin (77%) was still the main oral anticoagulant prescribed compared to DOACs (23%). 6 Similarly, a survey by Connell et al has found warfarin to be the most common choice of initial treatment of both deep venous thrombosis (DVT) (85.6%) and pulmonary embolism (PE) (89%) among attending physicians in the state of Rhode Island. 12
A major limitation that we faced in this study is that our sample is not fully representative of all health-care providers in Qatar which limits its external validity. Survey fatigue and lack of time required to fill the survey is another challenge that could have affected our response quality. We attempted to resolve this issue by validating our survey instrument to ensure that it is not time-consuming yet clear, comprehensive, and easy to understand. Finally, survey instruments that use Likert scale are prone to central tendency bias (choosing “neutral/ don’t know” answers). 18 However, majority of our questions had low percentage of these type of answers which likely reduce the impact of this type of bias.
Despite the established advantage of DOACs over warfarin, their prescribing still requires good knowledge to make appropriate evidence-based recommendation. In conclusion, this survey indicates that practitioners have moderate awareness on DOACs. Age, years of experience, and level of education are factors associated with enhanced DOACs’ awareness. Most practitioners don’t widely prescribe DOACs for their patients who require oral anticoagulation. Future work should focus on reassessing practitioners’ knowledge after providing well-designed education campaigns. Education courses should be tailored more toward agents present on the formulary.
Footnotes
Authors’ Note
Ahmed El-Bardissy and Hazem Elewa have contributed equally to the paper. This work has been presented at AC Forum meeting in 2017: Elewa H, El-Bardissy A, Mohammed S, Shible A, Imanullah R, Mohammed A. Assessing Physicians Knowledge and Attitude towards the Direct Oral Anticoagulants in Qatar. AC forum conference, April 20-22, 2017, Los Angles, California, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Qatar University student internal grant# QUST-2-CPH-2018-7.