
Abstract
Venous thromboembolism (VTE) is a common complication for critically ill patients. Intermittent pneumatic compression (IPC) is recommended for patients with high risk of bleeding. We aim to evaluate the effectiveness of IPC for thromboprophylaxis in critically ill patients. We searched PubMed, Embase, and ClinicalTrials for randomized controlled trials (RCTs) and observational studies that evaluated IPC in critically ill patients. RevMan 5.3 software was used for the meta-analysis. A total of 10 studies were included. The IPC group significantly reduced the VTE incidence compared with no thromboprophylaxis group (risk ratio [RR]: 0.35, confidence interval [CI]: 0.18-0.68, P = .002) and the IPC group also showed lower VTE incidence than the graduated compression stockings (GCS) group (RR: 0.47, CI: 0.24-0.91, P = .03). There were no significant differences between using IPC and low-molecular-weight heparin (LMWH) for VTE incidence (RR: 1.26, CI: 0.72-2.22, P = .41), but LMWH showed significantly more bleeding events. Intermittent pneumatic compression as an adjunctive treatment did not further reduce VTE incidence (RR: 0.55, CI: 0.24-1.27, P = .16). Intermittent pneumatic compression can reduce the incidence of VTE for critically ill patients, which is better than GCS and similar to LMWH, but it has no significant advantage as an adjunct therapy for thromboprophylaxis.
Introduction
Venous thromboembolism (VTE) includes deep vein thrombosis (DVT) and pulmonary embolism (PE). It is a common complication for hospitalized patients, which could prolong the length of hospital stay and even cause disability and death. For critically ill patients, the inability to free movement, infection, invasive operation, and other factors make them at extremely high risk of VTE. 1
Various preventive measures have been adopted to reduce the VTE incidence for patients who are at risk of VTE. There are generally 2 types of preventive measures for patients in the intensive care unit (ICU), one is drug therapies like low-molecular-weight heparin (LMWH), unfractionated heparin (UFH), or direct oral anticoagulants (DOACs), the other one is mechanical therapies like intermittent pneumatic compression (IPC) and graduated compression stockings (GCS). Although we have taken various measures to prevent thrombosis, VTE still occurs from time to time. 2,3 Autopsy of ICU patients who received prophylactic anticoagulation found that the incidence of PE was 14%. 4 Therefore, it is meaningful to choose the appropriate VTE precautions under this circumstance.
Mechanical prophylaxis alone is recommended for patients with high risk of bleeding or contraindications to anticoagulants. 5 And doctors sometimes also combine mechanical prevention with anticoagulants to achieve a lower VTE incidence. 6 Intermittent pneumatic compression is an intermittent inflating device that reduces the incidence of VTE by external pressure on the legs to increase local blood flow. Previous studies have confirmed the efficacy of IPC in stroke, trauma, and perioperative patients. 7 –9
In recent years, there have been many studies on the application of IPC in critically ill patients with inconsistent results. 10 –13 Whether IPC can reduce VTE incidence, or IPC is as effective as other therapies for thromboprophylaxis, or can adjunctive IPC further reduce VTE incidence among this population remain uncertain. Considering the lack of evidence, we think it is necessary to conduct this systematic review and meta-analysis to identify the effect of IPC on VTE prevention in critically ill patients.
Methods
We conducted this systematic review and meta-analysis in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis statement. 14 The protocol of this systematic review has been registered with the international Prospective Register of Systematic Reviews PROSPERO (registration number: CRD42019141124).
Search Strategy
We searched PubMed, Embase, and ClinicalTrials from inception to July 2019. Search strategies were adapted for each database, including medical subject headings and keywords for “intermittent pneumatic compression” and “critical illness” without limitations on publication type or language.
Inclusion and Exclusion Criteria
We identified eligible studies according to the following inclusion criteria: (1) original research studies for both randomized controlled trials (RCTs) and observational studies, (2) studies focusing on the efficacy of IPC for thromboprophylaxis in critically ill patients.
We excluded studies without a control group and studies that did not report our predetermined outcomes. Studies published as conference abstracts were also excluded in our meta-analysis.
Data Extraction and Quality Assessment
The quality of included studies was assessed by the Cochrane Risk of Bias Tool for RCTs 15 and Newcastle-Ottawa Scale for observational studies. 16 Two reviewers (Y.W-.W. and D-.H.) independently screened all the citations and selected studies that met the inclusion criteria. Disagreements between the 2 reviewers for study selection were discussed with Z.A-.L.
Definitions
Critically ill patients are defined as patients with severe trauma, being life-threatening or staying in the ICU for various reasons. Bleeding events include various degrees of bleeding, such as hematuria, bleeding gums, subcutaneous hemorrhage or hematoma, gastrointestinal bleeding, intracranial hemorrhage, and so on. For articles reporting more than one type of bleeding event, we calculate the sum of all bleeding events. Mortality is defined as the death of patients due to various causes. We take the mortality during ICU and the mortality during hospitalization as all-cause mortality. Deep vein thrombosis is evaluated by Doppler (compression) ultrasonography or venography, and PE is evaluated by spiral computed tomography, ventilation/perfusion lung scan, or pulmonary angiography.
Outcomes
The aim of our study was to validate the efficacy of IPC to prevent VTE in critically ill patients. The primary outcome was VTE incidence. For studies that did not report the incidence of VTE, if both the incidence of DVT and PE were reported, we regarded VTE incidence as the sum of DVT and PE incidence. Otherwise, we use a separate incidence of DVT instead. The secondary outcomes include DVT incidence, PE incidence, bleeding events, and all-cause mortality.
Heterogeneity and Sensitivity Analysis
We tested the heterogeneity of included studies using the I 2 statistics, and an I 2 value of greater than 50% was considered significant heterogeneity. 17 We used the fixed-effects models for data with insignificant heterogeneity and the random-effects models for data with significant heterogeneity. The sensitivity analysis was conducted by excluding one study in each turn to test the influence of a single study on the overall pooled estimate.
Statistical Analysis
We undertook the meta-analysis in Review Manager 5.3 software (Cochrane Collaboration, Oxford, United Kingdom). The results were presented in terms of risk ratio (RR) and 95% confidence interval (CI). All statistical tests were 2-sided and we defined statistical significance as P <.05.
Results
Study Selection
We identified a total of 2123 records through database searching. We removed 301 duplicates and 1812 records by reading the titles of these studies. The 180 remaining records were identified as being potentially relevant and abstracts were assessed for eligibility. A total of 31 articles discussed IPC for thromboprophylaxis and full articles were carefully read. Finally, 10 studies met all the inclusion criteria and were included in the meta-analysis 10 –14,18 –24 (Supplementary Figure 1).
Study Characteristics
Ten studies involving a total of 4759 patients were pooled in the meta-analysis, including 6 RCTs and 4 observational studies. In order to better illustrate the effect of IPC under different conditions, we divided the patients in the study into 4 subgroups: IPC versus no prophylaxis, IPC versus GCS, IPC versus pharmacological thromboprophylaxis, and IPC as an adjunctive therapy in addition to anticoagulants or GCS. The characteristics of included studies were summarized in Supplementary Table 1.
Risk of Bias
The risk of bias for each study was evaluated. Overall, all of the included trials were considered of moderate to high quality and the details of the results were presented in Supplementary Table 2.
Venous Thromboembolism Incidence
All the studies enrolled reported VTE incidence. We used the random-effects model to analyze these data. Four studies compared IPC with no prophylaxis for VTE prevention and the result showed that IPC could significantly reduce VTE incidence (6.0% vs 16.3%, RR: 0.35, CI: 0.18-0.68, P = .002, I 2 = 51%). Three studies compared IPC with GCS, and a lower VTE incidence was found in IPC group (4.2% vs 9.1%, RR: 0.47, CI: 0.24-0.91, P = .03, I 2 = 0%). Three studies compared IPC with LMWH and no significant difference was found between groups (6.6% vs 6.0%, RR: 1.26, CI: 0.72-2.22, P = .41, I 2 = 6%). Four studies take IPC as an adjunctive treatment and no significant difference was observed between groups (8.8% vs 9.7%, RR: 0.55, CI: 0.24-1.27, P = .16, I 2 = 71%; Figure 1).

Venous thromboembolism incidence.
Deep Vein Thrombosis Incidence
Nine studies reported DVT incidence. We used the random-effects model for the high heterogeneity. Subgroup analysis showed that IPC group had lower DVT incidence compared with no prophylaxis (5.8% vs 19.1%, RR: 0.34, CI: 0.19-0.60, P = .0002, I 2 = 0%). No significant differences were found for IPC versus GCS (2.6% vs 6%, RR: 0.39, CI: 0.07-2.27, P = .29, I 2 = 0%), IPC versus LMWH (5.0% vs 4.5%, RR: 1.36, CI: 0.63-2.95, P = .43, I 2 = 16%), and IPC as an adjunctive treatment (8.2% vs 8.8%, RR: 0.58, CI: 0.25-1.32, P = .19, I 2 = 70%; Figure 2).
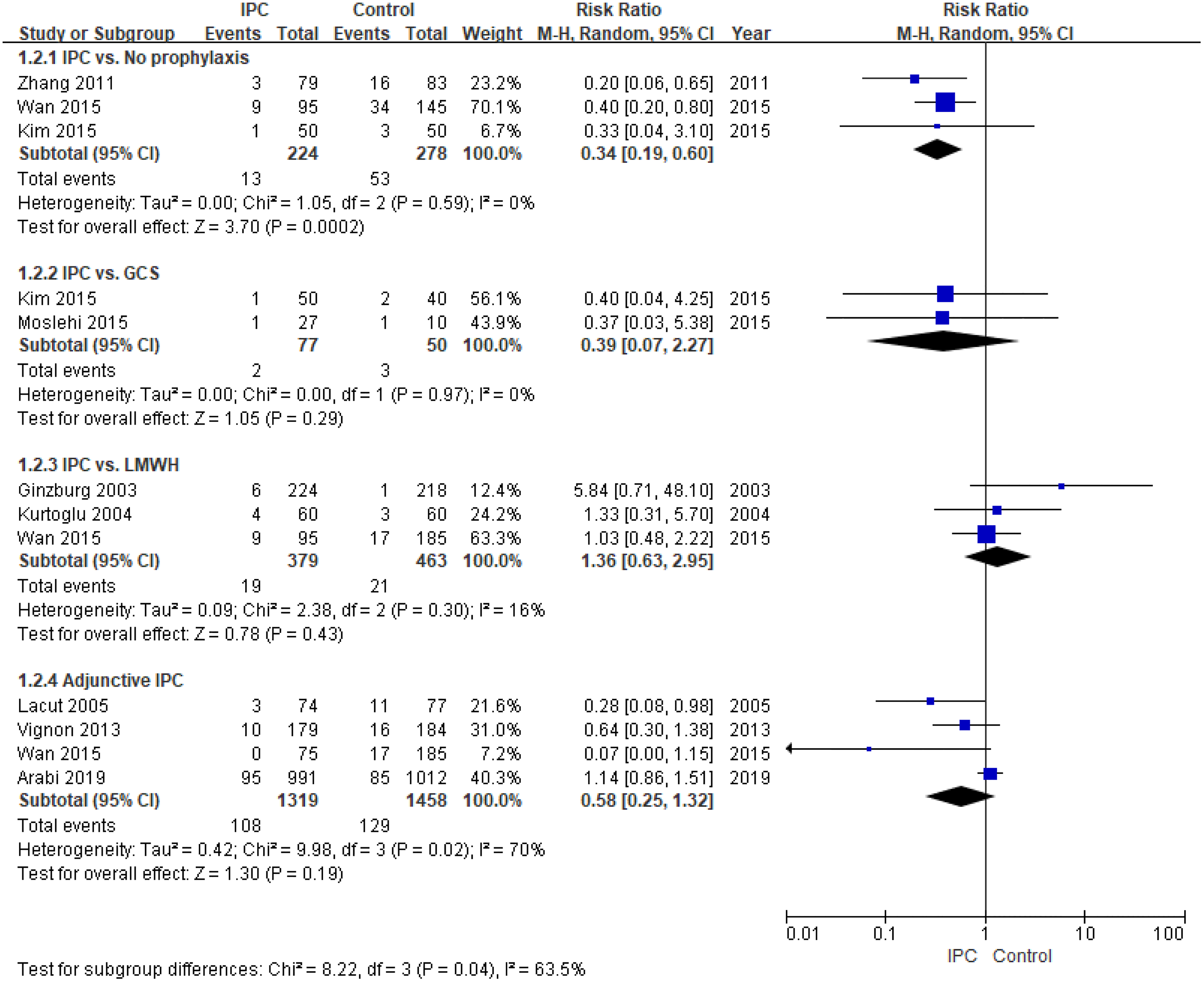
Deep vein thrombosis incidence.
Pulmonary Embolism Incidence
Six studies reported PE incidence. In addition to the small sample size of the IPC versus GCS group, we performed subgroup analysis in the remaining 3 subgroups using the fixed-model effects. Intermittent pneumatic compression showed significant lower PE incidence compared with no prophylaxis (1.7% vs 12.3%, RR: 0.17, CI: 0.06-0.50, P = .001, I 2 = 0%). Similar PE incidence were found in IPC versus LMWH (1.6% vs 1.5%, RR: 1.09, CI: 0.39-3.04, P = .87, I 2 = 2%) and adjunctive IPC group (0.6% vs 0.9%, RR: 0.72, CI: 0.31-1.69, P = .45, I 2 = 0%; Figure 3).

Pulmonary embolism incidence.
Bleeding Events
Three studies reported bleeding events comparing IPC with LMWH. Intermittent pneumatic compression showed significantly lower rate of bleeding events compared with LMWH group (3.4% vs 6.9%, RR: 0.46, CI: 0.24-0.88, P = .02, I 2 = 0%; Figure 4).

Bleeding events.
All-Cause Mortality
We analyzed the relationship between the use of IPC and mortality during hospitalization. A total of 4 studies reported thromboprophylaxis therapies using or not using IPC for all-cause mortality and no significant differences were found between the 2 groups (23.7% vs 25.0%, RR: 0.95, CI: 0.82-1.09, P = .46, I 2 = 0%; Figure 5).

All-cause mortality.
Funnel Plots for Publication Bias
We analyzed the publication bias by a visual inspection of the funnel plots. No obvious publication bias was observed in our meta-analysis (Supplementary Figure 2).
Discussion
Our systematic review and meta-analysis suggested that IPC significantly reduced the incidence of VTE, DVT, and PE in critically ill patients compared to those who did not receive any thromboprophylaxis. Lower VTE incidence was observed compared with GCS, but no significant differences were found for DVT incidence. There was no significant difference between IPC and LMWH for the incidence of VTE, DVT, and PE, but higher bleeding events were observed in the LMWH group. Intermittent pneumatic compression did not show significant advantage as an adjunct therapy in addition to GCS or anticoagulants for thromboprophylaxis. Using IPC to prevent VTE did not improve all-cause mortality for critically ill patients.
According to the Virchow’s triad, stasis, hypercoagulability, and vessel wall injury are 3 factors predispose patients to thrombosis. 24 Intermittent pneumatic compression is a mechanical measure to prevent VTE by pressurizing and deflating the calf from the distal end to the proximal end of lower limbs. Such compression increases the velocity of venous blood flow, thus reducing blood stasis of critically ill patients. 25 Besides, studies also showed that IPC could suppress procoagulant activation and increase fibrinolytic activity. 26,27 Our findings were consistent with the previous meta-analysis that IPC could reduce VTE incidence compared with placebo for both surgical and nonsurgical patients. 28
Graduated compression stockings could improve blood flow velocity by reducing the cross-sectional area of veins and is widely used in VTE prevention. 12,29 Limited number of studies reported the efficacy of GCS for VTE prophylaxis in critically ill patients. The Clots in Legs or Stockings after Stroke (CLOTS) 1 trial with more than 2500 hospitalized stroke patients showed that GCS did not reduce the incidence of VTE and could increase skin breaks. 30 The CLOTS 3 trial later showed that IPC significantly reduced the risk of proximal DVTs compared with the standard care group. 8 We speculate that the poor GCS effect may be related to the underlying disease of patients. From a pathophysiological point of view, critically ill patients and stroke patients lack active muscle contractions of the lower limbs that GCS might not improve blood flow velocity to a certain degree to achieve the preventive effect. The dynamic compression produced by IPC may be more efficient than the static compression produced by GCS. In our meta-analysis, we observed lower VTE incidence comparing IPC with GCS, but no significant difference was found for DVT incidence. It was generally because only 2 studies with 127 patients were included. Although the reported DVT incidence was 2.6% in the IPC group and 6.0% in the GCS group, the sample size was too small to prove a positive result. More studies are needed to further confirm this result.
The 9th American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis Guidelines suggest the use of mechanical thromboprophylaxis with GCS or IPC for patients at increased risk of thrombosis who are bleeding or at high risk for bleeding. 31 The 2018 American Society of Hematology (ASH) Guideline on VTE prophylaxis suggests using pharmacological VTE prophylaxis over mechanical VTE prophylaxis for acute or critically ill medical patients with very low certainty in the evidence of effects. 32 In our meta-analysis, IPC is not inferior to LMWH for reducing the incidence of VTE, DVT, and PE. These results were consistent with the previous network meta-analysis for critically ill patients that LMWH and UFH showed lower risks of DVT than IPC without statistically significant differences. 33 In addition, we observed more bleeding events in LMWH group compared with patients receiving IPC. For critically ill patients, trauma, major surgery, and various invasive procedures put them at higher risk of bleeding. Intermittent pneumatic compression may be safer from the perspective of reducing bleeding events and may also be a good option for VTE prevention for critical illness. However, we also need to point out that only 2 RCTs and one observational study were enrolled to compare the efficacy of IPC with LMWH. More high-quality studies are needed to further verify our results.
Intermittent pneumatic compression as an adjunctive therapy for thromboprophylaxis did not further reduce the incidence of VTE, DVT, and PE in our study. For the 4 articles included, 2 studies with large sample size both showed neutral results. The PREVENT trial was a multicenter RCT and various IPC devices were used in different hospitals. According to some studies, the incidence of VTE between different IPC devices may vary greatly, and different types of heparins may also influence the VTE incidence for various underlying diseases. 34 –37 The CIREA1 trial found a trend for additional IPC to reduce VTE incidence, but no significant differences were found between groups. The 2018 ASH guideline suggested using pharmacological or mechanical method for VTE prophylaxis alone rather than combining pharmacological method with mechanical method for VTE prophylaxis. 32 In our study, no statistically significance was found in the adjunctive IPC group. Considering the lower incidence of VTE and the insufficient sample size, more high-quality studies are needed to further validate the effect of IPC as an additional treatment.
In recent years, the application of IPC for thromboprophylaxis in critically ill patients has attracted much attention. However, studies included the comparison of IPC with GCS, anticoagulant, and other preventive measures with inconstant results. Limited studies summarized the efficacy of IPC compared with other preventive measures. A meta-analysis about mechanical thromboprophylaxis in critically ill patients published in 2006 showed that the use of compressive and pneumatic devices did not reduce VTE incidence compared with no treatment or the use of LMWH. A network meta-analysis published in 2016 suggested that IPC only showed a trend for lower DVT incidence compared with the control group, but the effect was not statistically significant. 33 Our meta-analysis compared the thromboprophylaxis effects of IPC with other preventive measures. The results showed that IPC could reduce the risk of VTE without increasing bleeding events and all-cause mortality. We hope that this meta-analysis could provide the latest evidence for the use of IPC to prevent VTE in critically ill patients.
Limitation
Our meta-analysis has some limitations. Firstly, clinical heterogeneity is inevitable. The duration of IPC use varies in the included studies, and the disease and coagulation status of patients may affect the incidence of VTE. Secondly, some studies only screened patients with suspected PE, so the incidence of PE may be biased, thus affecting the effectiveness of IPC assessment. Thirdly, in order to better illustrate the effectiveness of IPC in different situations, we did subgroup analysis. Although the heterogeneity was reduced, it led to a relatively small number of studies for each group. In addition, our meta-analysis included both RCTs and observational studies. The observational studies are very prone to bias, which may affect the results of our study. More high-quality RCTs are needed to further confirm our results.
Conclusion
Intermittent pneumatic compression can reduce the incidence of VTE in critically ill patients, and its effect is better than GCS and is not inferior to LMWH. The use of IPC as an adjunctive treatment does not further reduce the incidence of VTE. More high-quality RCTs are needed to confirm the results of this study.
Supplemental Material
Supplemental Material, sup_Fig._1_flow - Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental Material, sup_Fig._1_flow for Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis by Yiwei Wang, Dong Huang, Maoyun Wang and Zongan Liang in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplemental Material, sup_Fig._2_Funnel_plots_for_publication_bias - Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental Material, sup_Fig._2_Funnel_plots_for_publication_bias for Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis by Yiwei Wang, Dong Huang, Maoyun Wang and Zongan Liang in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplemental Material, sup_table_1_characteristics - Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental Material, sup_table_1_characteristics for Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis by Yiwei Wang, Dong Huang, Maoyun Wang and Zongan Liang in Clinical and Applied Thrombosis/Hemostasis
Supplemental Material
Supplemental Material, sup_table_2_quality - Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental Material, sup_table_2_quality for Can Intermittent Pneumatic Compression Reduce the Incidence of Venous Thrombosis in Critically Ill Patients: A Systematic Review and Meta-Analysis by Yiwei Wang, Dong Huang, Maoyun Wang and Zongan Liang in Clinical and Applied Thrombosis/Hemostasis
Footnotes
Authors’ Note
Yiwei Wang and Dong Huang are co-authors. Y.W-.W. designed the study, conducted the literature search, performed data analysis, and drafted the manuscript. D-.H. helped in the design of the study, conducted the literature search and drafted the manuscript. M.Y-.W. helped in data analysis and revised the manuscript. Z.A-.L. revised the manuscript critically for important intellectual content and provided the final version for publication. All authors read and approved the final manuscript. Each enrolled trial was approved by the corresponding institutional Ethical Committee, and all participants provided written informed consent. Neither the entire paper nor any part of the manuscript is published or under consideration of publication in any other journal or conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Key Research and Development Program of China (2016YFC1304303). Sichuan Science and Technology Agency Grant (2015JY0176).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.