
Abstract
Thromboprophylaxis following arthroscopic knee surgery (AKS) is not clear in the literature. The purpose of this study was to present the incidence of symptomatic deep vein thrombosis (DVT) following elective AKS over the age of 40. The secondary purpose was to investigate risk factors associated with venous thromboembolic events (VTEs). Surgical database and outpatient clinic follow-up charts of the patients who underwent AKS for any reason were included in the study. Odds for risk factors such as previous medical history of thrombosis, any family history for clotting disorders, diabetes mellitus (DM), oral contraceptive usage, body mass index, history of malignancy, and smoking were evaluated. The incidence of DVT following AKS significantly increased in the patients older than 40 years who had a previous medical history of VTE, DM, and smoking. A variety of guidelines exist for VTE prophylaxis; however, one should focus on risk factors related to the patient’s medical history and current medical conditions. In this study, smoking, DM, and previous history of DVT increased DVT risk significantly, and thromboprophylaxis should be kept in mind for these patients.
Introduction
Venous thromboembolism (VTE) is one of the most devastating complications in orthopedic surgery. Common consensus standards for VTE prophylaxis were set for certain orthopedic procedures such as joint replacement, vertebra, trauma, and tumor surgery. However, there are no standards for other orthopedic procedures, including upper extremity surgery and arthroscopic lower extremity procedures. Understanding the risk of VTE associated with these procedures is very important so that future guidelines may be developed based on these data. Arthroscopic lower extremity procedures are the most common orthopedic procedures in the world. 1 –3
Arthroscopic knee surgery (AKS) is associated with a low risk of deep vein thrombosis (DVT). 4 –7 Prospective studies suggest a rate of 1.2% to 17.9% DVT after AKS. 7 –13 The rate of symptomatic proximal thrombosis is reported much less (0.25%-0.67%). 1,3,10,14 However, VTE accounts for 7% to 30% of all complications following AKS. 15,16 Although some authors recommend routine prophylaxis after AKS, routine prophylaxis is not recommended in the guidelines. 1 –3,7,17 –19 All these studies were conducted on the entire population or adolescents. There is no clear data about DVT in the middle-aged or elderly population following AKS in the literature.
The purpose of this study was to present the incidence of symptomatic DVT following elective AKS that is performed without prophylaxis over the age of 40. The secondary purpose was to investigate risk factors associated with VTE events in the same population to consider the best VTE risk assessment model for use in the preoperative evaluation of patients undergoing AKS.
The present study hypothesized that the incidence of DVT would increase over the age of 40 following elective AKS without any prophylaxis.
Material and Methods
Surgical database and outpatient clinic follow-up charts of the patients who underwent AKS for any reason were queried. The patients who had less than 6 weeks of follow-up, had knee arthroscopy due to infection, fracture, or arthrofibrosis and had received preoperative or postoperative VTE prophylaxis were excluded from the study. The patients who were older than 40 years were evaluated for risk assessment.
Institutional Scientific Research Ethical Committee approval was obtained for this study. Preoperative VTE risk assessment was not calculated for the patients; however, past medical history of VTE, any family history for clotting disorders, any risk factors such as diabetes mellitus (DM), oral contraceptive (OCD) usage, increased body mass index (BMI), history of malignancy, and smoking were all queried. 2 The patients were divided into 3 groups for the evaluation of BMI. Body mass index was smaller than 25 in the healthy group, it was between 25 and 30 in the borderline group, and over 30 in the obese group. Arthroscopic procedures for all patients were also noted. Arthroscopic interventions were categorized as meniscus repair, cartilage repair, anterior cruciate ligament (ACL) reconstruction, and meniscectomy or joint debridement.
All operations were performed under tourniquet, and routine VTE prophylaxis was not applied to patients. A compressive bandage was used for all patients after the surgery for 12 hours. Any postoperative VTE or pulmonary embolism (PE), calf pain, and erythematous swelling were noted, and these patients were evaluated for risk factors. The diagnosis of DVT was confirmed with Doppler ultrasound in all cases.
Statistical analysis was performed by IBM SPSS Statistics for Windows (version 19.0; IBM Corp, Armonk, New York). A suitable χ2 test was used for qualitative data. After the risk factors for DVT were compared in pairs, the data that were P < .10 level were evaluated with a backward stepwise logistic regression method to demonstrate risk factors. After logistic regression analysis, the method differentiated 45.5% of the patients and 99.9% of healthy individuals. The logistic regression model assessed that there was harmony as a whole according to Hosmer and Lemeshow tests (P = 240). Nagelkerke R 2 is .487 and explains 48.7% of the variance in DVT formation. P < .05 was considered statistically significant.
Results
Surgical database and outpatient clinic follow-up charts of 1466 patients who underwent AKS for any reason and who had at least 6 weeks of follow-up were queried. Eighty-one patients who had knee arthroscopy due to infection, fracture, or arthrofibrosis and had received preoperative or postoperative VTE prophylaxis were removed from the study. A total of 1385 patients were included in the study. The patients older than 40 years (n = 610) were evaluated for risk assessment. Fifty-three percent of the patients older than 40 years (324) were male, and 47% (286) were female. Eleven patients had thromboembolic events in total with an incidence of 0.79%.
Nine patients who were older than 40 years had either DVT or PE; on the other hand, only 2 cases were observed in the younger group. The incidence was 1.47% in the patients older than 40 years, and it was 0.25% in the younger group. When these 2 groups were compared, the difference was statistically significant (P = .014).
Six of the patients who had DVT were female; however, female sex was not significantly associated with increased risk of DVT after the age of 40 (odds ratio [OR]: 0.44, 95% confidence interval [CI], 0.11-1.76, P = .24).
History of malignancy was also investigated as a risk factor. Only 2 patients had a history of previous malignancy, and one of them had DVT. Therefore, the history of malignancy was found to be a significant risk factor after the age of 40 (OR: 75, 95% CI, 4.30-1307.37, P = .0031).
The previous history of DVT was positive in 11 patients. Five of these patients had DVT or PE. The previous history of DVT increased the risk of DVT significantly (OR: 12.95, 95% CI, 26.54-578.93, P < .0001).
Diabetes mellitus was seen in 14.59% (89) of the patients. Six patients with DM had DVT or PE. Diabetes mellitus was also significantly associated with an increased risk of DVT (OR: 12.49, 95% CI, 3.06-50.88, P = .0004).
A family history of any coagulation disorders was also investigated in this study. Four patients had a positive family history of coagulation disorder, and only 1 of them had DVT. A positive family history of coagulation disorder was also significantly associated with an increased risk of DVT (OR: 24.91, 95% CI, 2.33-266.08, P = .0078).
One hundred and forty-four (23.6%) patients were smokers in this group, and 6 of them had DVT or PE. The risk of postoperative DVT increased up to 6.7-fold for smokers when compared to nonsmokers (OR: 6.71, 95% CI, 1.66-27.18, P = .0076).
Oral contraceptive usage among women was also investigated. One hundred and twenty-two (42.6%) women prescribed OCD, and 2 of them developed DVT after the operation. Oral contraceptive usage did not increase the risk of postoperative DVT significantly among women (OR: 5, 95% CI, 0.90-27.84, P = .066).
The BMI of the patients was summarized in Table 1. The BMI was not associated with postoperative DVT in this study (P > .05). Arthroscopic interventions were summarized in Table 2. The association between the arthroscopic interventions and postoperative DVT was insignificant in this study (P > .05).
BMI of the Patients.
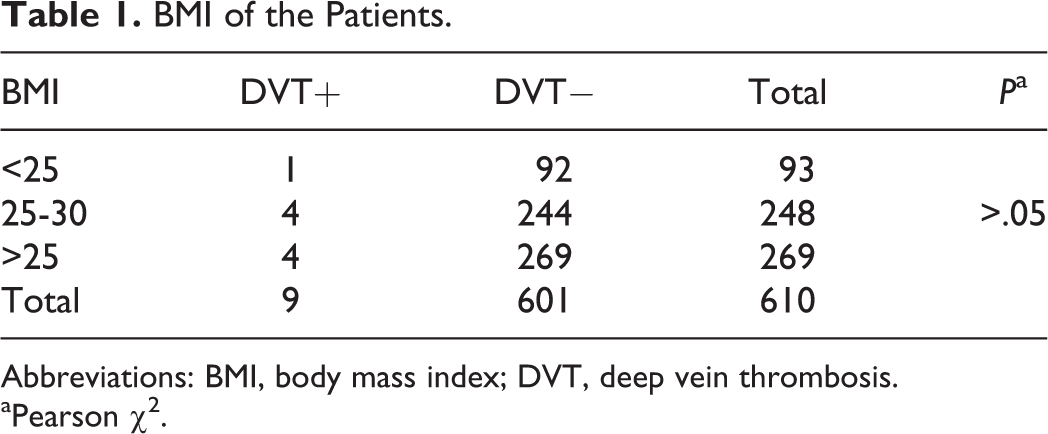
Abbreviations: BMI, body mass index; DVT, deep vein thrombosis.
aPearson χ2.
Arthroscopic Interventions

Abbreviations: ACL, anterior cruciate ligament reconstruction; cartilage, cartilage repair intervention; DVT, deep vein thrombosis; Men. & Deb., meniscectomy and debridement; Men. Rep., meniscus repair.
aPearson χ2.
Discussion
The incidence of DVT after major orthopedic surgery is relatively high; therefore, some form of thromboprophylaxis is provided for these patients. 1 –3,7,20,21 However, the risk is not clear after AKS. 1,2,7,17 Since VTE is relatively low after AKS, routine thromboprophylaxis is not recommended after these operations. 1,2,7,17 –19,22,23 There are many studies to clarify this subject in the literature; however, none of them are about the older population in which the risk is even higher for thromboembolic events. 1 –3,7,18 –24 Arthroscopic knee surgery is the most common orthopedic operation throughout the world; therefore, understanding the risk is very important to develop guidelines and possible patterns for surgeons. 7,17 –19,22,23
The total incidence of DVT in following AKS was relatively low (0.79%) in this study, and it was comparable with the literature. 1,2,19,21 –23 However, when the incidence of the patients older than 40 years was compared with the incidence of the younger patients, an approximately 6-fold increase that was statistically significant (P = .014) was observed. Maletis et al also observed the incidence of DVT higher in the patients older than 50 years in their 20 770 patients cohort similar to this study; however, they did not assess risk factors for this age-group. 1 However, Delis et al 8 did not find any difference between young and old age-groups for the development of DVT after AKS. On the other hand, there is a case report of a 17-year-old lady who died of a PE after ACL reconstruction in the literature. 25 She had risk factors such as a family history of a thromboembolic disorder and OCD usage. Case reports of fatal VTE events highlight the need for risk assessment and the need for thromboprophylaxis in high-risk patients. The risk was much higher for the patients older than 40 years in this study; therefore, risk assessment was required for this age-group. Our hypothesis was thus confirmed with these findings.
The known risk factors for DVT following AKS are female sex, OCD usage, previous history of malignancy and DVT, family history of thromboembolic disorders, smoking, BMI, and type of arthroscopic intervention. 1,2,7,17,24,26 All these risk factors were evaluated for patients older than 40 years in this study. Many articles are evaluating the risk factors of DVT after elective AKS; however, these studies include the whole population or adolescents. Demers et al 9 investigated risk factors such as age, sex, previous history of DVT, family history of VTE events, history of medication, anesthesia, tourniquet time, and duration of immobilization. Only tourniquet time longer than 60 minutes was found to be a statistically significant risk factor. Delis et al 8 also investigated risk factors for DVT such as age, smoking, BMI, venous insufficiency, previous DVT, and OSC usage. A positive history of DVT was found to be the only significant risk factor. History of malignancy, previous history of DVT, DM, family history of any coagulation disorder, and smoking were associated with an increased risk of DVT or PE over the age of 40 in this study.
Female (>40 years of age) sex itself was not associated with increased risk of DVT similar to the literature in this study (P = .024). 1,2 There are many studies about the increased risk with OCD usage in current literature; however, the population included all females in these studies. 1,2,27 Maletis et al 1 remarked that female patients who had been prescribed OCD had a higher incidence of DVT compared to the ones who had not received such a prescription. Oral contraceptive usage among females older than 40 years also increased the risk in this study (OR: 5); however, this increase was statistically insignificant in contrast to the literature (P = .066). 8 There is a case report of a 17-year-old female soccer player who died of PE after ACL reconstruction in the literature. 25 Therefore, further investigations are needed to clarify the risk of OCD after AKS.
History of malignancy is one of the known risk factors for VTE; however, there are no data about the risk of DVT after AKS in the literature. Only 2 patients had a history of malignancy in this study, and 1 of them developed DVT. History of malignancy was found to be a significant risk factor for the development of DVT after AKS over the age of 40 in this study (OR: 75, P = .0031). However, the sample size for this risk factor is small; the result might be misleading. Further investigation is also needed for this subject.
In patients with first spontaneous DVT, the annual likelihood of recurrence is 5% to 15%, with a cumulative recurrence rate of 25% after 4 years. 26 However, the risk is lower in patients with postoperative DVT. 26 The previous history of DVT was a significant risk factor over the age of 40 (OR: 12.95, P < .0001) in this study. Delis et al 8 also found the risk significant for the previous history of DVT. We recommend thromboprophylaxis if the patient had a positive DVT history following AKS.
Diabetes mellitus is a well-known disease with many microvascular complications. The risk of DVT was significantly increased for the patients who had DM over the age of 40 in this study (OR: 12.49, P = .0004). However, no data were found about this risk factor after AKS in the literature. Since the relationship is strong, we also recommend thromboprophylaxis if the patient had known DM after AKS over the age of 40.
The risk of positive family history for any coagulation disorder was also investigated in this study, and the risk increased with positive family history (OR: 24.91, P = .0078). Demers et al 9 found that positive family history for VTE events did not increase the risk of postoperative DVT after AKS. There is not much data about this subject in the literature. The results of this study suggested an increased risk; however, the sample size for this risk was very small. Only 1 of 4 patients had postoperative DVT. Larger series are needed to confirm this result.
Smoking is a predisposing factor for DVT, and 23.6% of the patients were smokers in this study. 26 Smoking did not increase the risk for DVT after AKS due to some articles in the literature 8 ; however, the risk increased significantly in this study for smokers older than 40 years compared to nonsmokers (OR: 6.71, P = .076). Thromboprophylaxis should be kept in mind following AKS for heavy smokers.
Obesity is one of the risk factors for postoperative DVT 26 ; however, the risk did not increase significantly in this study. There is no consensus about the relationship between obesity and DVT following AKS in the literature. Although some authors found an increased risk in the pediatric population up to 6.1-fold, 28 some authors 25 did not found any significant difference between obese and nonobese patients. It was thought that more evidence is needed to reach an agreement about this subject.
Some complex arthroscopic interventions such as ACL reconstruction tend to have increased risk for DVT, since complex operations increase the tourniquet time and therefore increase the duration of stasis that leads to increased risk. 29 Increased tourniquet time may be associated with increased postoperative DVT risk following AKS. 9,29 The evidence is not clear about this subject in the literature. Some studies have not reported any statistically significant relationship between the type of procedure and postoperative risk of DVT. 1,30 However, other larger series suggested tourniquet time more than 60 minutes as a risk factor. 9,20,31 The association between arthroscopic procedure complexity and risk of postoperative DVT over the age of 40 was insignificant in this study. This situation may be related to a decreased need for complex arthroscopic operations such as ligament reconstruction over the age of 40. However, tourniquet time is important for the development of DVT after orthopedic surgery, 26,29 and it was not investigated in this study due to insufficient data, which was one of the limitations of this study.
The major limitation of this study was its retrospective nature. The risk factors were evaluated according to previous patient database knowledge and follow-up charts. Another limitation was the investigation of OCD usage for female patients. Oral contraceptive usage was investigated as a risk factor; however, we could not be sure that they took the medication routinely or not, due to the retrospective nature of the study.
Although many risk factors such as age, DM, previous history of DVT, smoking, and family history for thromboembolic disorders increased the risk of DVT significantly following AKS over the age of 40, this may be clinically unimportant due to still very low incidences. Lack of investigation of anesthesia type that may influence DVT risk was also a limitation for this study.
Another limitation was a very small sample size for some risk factors such as previous malignancy or DVT and positive family history for any coagulation disorders. These risk factors increased the risk significantly in this study; however, the interpretation of these data is limited since calculated risks based on a low number of cases.
There are some studies in the literature about the efficiency of DVT prophylaxis following AKS, and most of them used ultrasonography measurements for follow-up. They suggested chemical prophylaxis, but most of the DVT cases that they found were in calf veins (distal DVT) that were clinically not important. 32 –34 Clinically relevant bleeding was higher in the chemoprophylaxis group. 4 These studies suggest that DVT incidence was decreased with thromboprophylaxis; however, many of them were subclinical, which may not require treatment with the potential risk of bleeding. 17 –19,22,23
Recent meta-analyses about the effect of anticoagulants on VTE prevention suggest that anticoagulation therapy following AKS is ineffective, and they do not recommend routine prophylaxis because 7,17 –19,22,23 the incidence is still very low, and many DVTs are clinically unimportant. However, in the relatively older age group, some well-known risk factors were discussed in this article. The odds of thromboembolic events increased with age, smoking, DM, and previous history of DVT in this study. Therefore, individual risk model assessment should be developed for patients undergoing AKS. It should be remembered that risk is even higher in elderly patients. Group model DVT chemoprophylaxis that is applied to hip and knee arthroplasty patients would not be valid for AKS patients who require an individual model of prophylaxis.
Today guidelines about prophylaxis following AKS vary, and consensus has not been reached. 35 Current recommendations in the American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (ninth edition) suggest thromboprophylaxis only for patients with a history of prior VTE following AKS. 36 However, the National Institute for Health and Clinical Excellence guidelines suggest low-molecular-weight heparin for 14 days if total anesthesia time is over 90 minutes or the VTE risk of the patient outweighs the risk of bleeding. 37 These universal guides do not describe risk factors for DVT for the elderly population. How other risk factors that are affected by age are unknown.
As a conclusion, the incidence of DVT following AKS is very low. Whether the rate of DVT following AKS is 0.1% or 10%, millions of AKSs are performed each year, and this generates thousands of people with VTE complications. Venous thromboembolism risk assessment should be a routine part of preoperative evaluation before AKS, especially in high-risk patients older than 40 years. A VTE risk scoring system is needed for the appropriate use of chemoprophylaxis following AKS. A variety of guidelines exist for VTE prophylaxis; however, one should focus on risk factors, especially in the elderly related to patient’s medical history and current medical conditions. In this study, smoking, DM, and previous history of DVT increased DVT risk significantly following AKS, and thromboprophylaxis should be kept in mind for these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.