
Abstract
In this randomized trial, we compared the hemodynamic effects of 2 different methods of bilateral sequential pneumatic compression (Simultaneous compression with Fixed cycling rate [SF] vs Alternate compression with Adjusted cycling rate [AA]) and investigated whether venous flow augmentation influenced deep vein thrombosis (DVT) development in patients undergoing total knee arthroplasty. Pneumatic compression was started on the operation day and applied to discharge. A total of 108 limbs was evaluated by computed tomographic angiography and duplex ultrasound. Augmented peak volume flow (P = .008), expelled total volume (P < .001), and expelled peak volume (P < .001) were significantly larger in group SF. The DVT developed in 35 (32.4%) limbs, and they were neither symptomatic nor ileofemoral in location. The enhanced hemodynamic parameters did not influence the DVT development. In conclusion, group SF showed superior hemodynamic efficacy, but this superiority may not be a surrogate for better thromboprophylaxis.
Introduction
In patients undergoing total knee arthroplasty (TKA) without thromboprophylaxis, deep vein thrombosis (DVT) incidence has been as high as 46% to 84%. 1 –3 For these patients, intermittent pneumatic compression (IPC) has been widely used and was still recommended as one of the grade 1 modalities for the prevention of thrombosis in the new guidelines of American College of Chest Physicians published in February 2012. 4 From the results of 3 randomized controlled trials to date that included 503 patients with TKA, IPC achieved 62.5%, 88.8%, and 100% reduction in DVT incidence, respectively, compared to the control group. 5 –7 However, we cannot help hesitating before selection of 1 IPC device over another because of insufficient studies that link different methods of IPC with the respective physiological and clinical effects. 8
Sequential compression, compared to uniform compression, was reported to provide more efficient venous emptying 9 and to increase the peak flow velocity more efficiently by over 200% within the lumen. 10 We have 2 different sequential compression devices that were claimed to have major market share. While the DVT-2600 (DS MAREF, Gunpo, Korea) offers a simultaneous compression, the SCD Express (Tyco Healthcare/Kendall, Massachusetts) offers an alternate compression. There is the theoretical presumption that simultaneous bilateral compression might be superior to alternate bilateral compression in augmentation of venous return and volume flow, which seems to be in accordance with the results of our preliminary study of 4 volunteers. All of them showed even more increase in peak velocity (PV), total volume flow (TVF), and peak volume flow (PVF) after simultaneous compression. The SCD Express showed a promising venous hemodynamic performance by offering customized compression that was readjusted every 30 minutes to individual refill time of both legs. 11 However, it should be asked whether or not this refill time-adjusted compression device works optimally throughout the duration of IPC, considering that venous hemodynamics can change at irregular intervals and vary depending on position, postoperative day, and the activity of patients. 12
It is true that venous hemodynamics indicated mainly by peak venous velocity or venous volume flow is commonly accepted as a surrogate measure of clinical efficacy of IPC, 11,13,14 but the relationship between them has not yet been determined. In an effectiveness study comparing 5 pneumatic compression devices that were used in 1350 patients, the highest DVT incidence was observed not in the device group showing the least increase in PV but in that showing the greatest increase. 15
The aims of this study were to compare the hemodynamic effects of 2 different methods of bilateral sequential compression (Simultaneous compression with Fixed cycling rate [group SF] vs Alternate compression with Adjusted cycling rate [group AA]) and to investigate whether venous flow augmentation influences DVT development in patients undergoing TKA.
Patients and Methods
This study was performed at the Seoul Metropolitan Government-Seoul National University Boramae Medical Center in Seoul (Korea). The protocol was approved by the local institutional review board (IRB approval number: 20111102/08-2011-6/113). All patients signed an informed consent before their participation in the study. The protocol was registered at ClinicalTrials.gov (ID: NCT01779648).
Study Design and Interventions
This study was a single-center, single-blind (patient), and randomized trial that compared the hemodynamic performance of the 2 parallel interventional arms. One was assigned for bilateral simultaneous sequential compression with an optimally fixed cycling rate using DVT-2600 (group SF) and the other for bilateral alternate sequential compression with an adjusted cycling rate using SCD Express (group AA). All operations were performed by a single orthopedic surgeon, and the same operative technique was used in all patients. Pneumatic compression was started on the day of the operation. Because all patients had continuous passive movements and an identical regime of physiotherapy every day, it would have been quite difficult to maintain the continuous application of IPC and good compliance if the IPC duration had been too long. Therefore, we determined to strictly apply continuous IPC for 2 hours 2 times a day to discharge without concern of poor compliance based on the reports indicating that 4- and 18-hour IPC were similarly effective in terms of
Study Patients and Eligibility
Adult patients aged more than 18 years who were not under anticoagulation therapy and had been admitted for TKA were recruited for enrollment in the study. Preoperatively, the recruited patients were thoroughly interviewed, clinically examined, and tested by ultrasonography. Patients were excluded if they had chronic superficial or deep venous insufficiency, DVT, venous anomalies like a duplication of the superficial femoral vein, history of venous thromboembolism, severe arteriosclerosis obliterans without a palpable dorsalis pedis pulse, or inappropriate conditions for compression like open fracture, hemorrhagic condition, or extensive dermatitis of the lower branches, and congestive heart failure. Additional exclusion criteria included a documented malignant tumor because pharmacological prophylaxis with anticoagulants would be a more reasonable treatment in such patients.
Description of IPC Devices
The SCD Express provides bilateral alternate and graded sequential compression with an adjusted cycling rate, which is changeable in accordance with an individual’s separate venous refill time of lower limbs. The DVT-2600 provides bilateral simultaneous and graded sequential compression with a fixed cycling rate. A cycle time was determined by adding up cuff inflation and deflation times. The DVT-2600 was designed to offer 12 seconds of inflation and several options of fixed deflation times. In order to select the optimal cuff deflation time, we performed a preliminary study in which postcompression venous refill times of 61 volunteers (age 39.2 ± 9.9 [21-60] years; 32 men), enrolled with the same exclusion criteria, were investigated using duplex ultrasound (DU). The median value was 28 seconds, and the cuff deflation time was determined to be fixed at 28 seconds. Thereby, the DVT-2600 used in group SF produced SF of 90 cycles/h. In contrast, the SCD Express provided 11 seconds of inflation and measured the postcompression time of the 2 legs separately and then used the longest refill time of both legs to adjust the compression. 11 Thereby, the SCD Express used in group AA produced AAs. Both devices were the latest in their respective series and had been designed to improve overall compliance of both the patients and the medical team, and thus, optimize thromboprophylaxis. Both manufacturers reduced the size and weight of the devices (<2 kg) to improve portability and handling. The SCD Express has the optional battery power, which supports full functioning for 6 to 8 hours, and the same for the DVT-2600, which is supported for 8 to 10 hours. Noises were reduced to 60 dB in the DVT-2600 and 80 dB in the SCD Express. With regard to sleeves, both devices not only have similar cuff volume and tube thickness but also have same chambers. Nevertheless, we used only the sleeves of the DVT-2600 in order to exclude the sleeves-related bias. The sleeves had 3 circumferential air chambers running the distance from the ankle to the lower thigh. For equivalence of cuff pressure generation, a specially modulated tube adaptor formulated by a medical engineering team after tests was connected to the SCD Express, so that both devices could produce similar cuff pressures with a maximum lower calf pressure of 40 to 45 mmHg.
Detection of DVT and Measurements of Venous Hemodynamics
The CTA and DU scan were performed to detect DVT and to measure venous hemodynamic parameters, respectively. When the CTA was not reliable for the evaluation of popliteal vein because of the artificial knee material, DU using a 12.5-MHz linear-array transducer (iU22; Philips Ultrasound, Bothell, Washington) was used instead. The criteria for a positive finding included lack of vein compressibility and visualization of thrombus. Additional computed tomography with a special protocol for detecting acute pulmonary embolism was planned in case it was symptomatic or proximal DVT. In order to attain flow and velocity measurements, we followed the detailed methodology described in the literature published by Kakkos et al. 18 Briefly, longitudinal scans of bilateral superficial femoral veins, just distal to the confluence of the profunda femoral veins, were performed. Baseline velocity, flow pattern, and augmented flow produced by a cuff inflation were recorded. Under a fixed state of other ultrasound scan parameters, PV was measured by determination of the maximum point of the augmented waveform. The TVF was automatically calculated by the software. The PVF was also calculated with 1-second interval around the PV. Expelled volume was a theoretically calculated value in order to figure out how much blood was squeezed by the compression for an hour; expelled total volume (ETV) = single cycle augmented TVF × cycling rate (cycles/h) and expelled peak volume (EPV) = single cycle augmented PVF × cycling rate (cycles/h). All the measurements were performed in the supine position.
Sample Size
In order to determine the appropriate sample size, the mean and standard deviation of EPV (mL/h) measured in a similar randomized study of 34 participants were used. The previous study, the data of which are not yet published, was designed to compare simultaneous compression with alternate pneumatic compression and was approved by the IRB of Dongguk University Ilsan Medical Center (Goyang, Korea; IRB approval number: 2009-1-54). In the previous study, the EPV was the only parameter that showed statistical significance (P = .045) between the 2 methods of compression. The pooled standard deviation and mean difference were 274.6 and 225.2 mL/h, respectively. Using a 2-side test with α = .05 and 1-β = .85, the minimum sample size was 27 for each arm, thereby 54 patients was enrolled in this study.
Randomization and Blinding
The patients who signed the informed consent were numbered in recruiting order for the screening test including a DU. Once the inclusion criteria were met, the patients were enrolled and randomly allocated to either group. The random allocation sequence was simply generated by a computer program without any restrictions and managed by a researcher who was otherwise unrelated to the study. The random allocation code was delivered in a sequentially numbered, opaque-sealed envelope on the day of the operation. The patients were blinded to group assignment, and the success of blinding was checked by confirmation of the patients’ lack of awareness of the IPC type at discharge.
Statistical Analysis
The continuous data of the 2 groups were expressed as mean ± standard deviation and analyzed using a 2-tailed, unpaired t test or Mann-Whitney U test if the normality was not satisfied after using the Kolmogorov-Smirnov test. Categorical variables were compared with the chi-square test. Hemodynamic parameters were compared using a linear mixed-effects model where age, sex, body mass index, and baseline values were controlled as fixed-effects parameters. In the risk factor analysis for the development of DVT, statistical significance was obtained using the multivariable logistic regression model or the generalized linear model with generalized estimating equation if within-subject correlation had to be considered. P values of .05 or less were considered statistically significant. The SPSS version 20.0 (SPSS Inc, Chicago, Illinois) was used for the analysis.
Results
Between March 2012 and January 2013, a total of 57 patients were recruited. Two of them were excluded prior to group assignment because of the detection of a lung cancer and a DVT, respectively. During the study, an additional patient who was initially allocated to group SF was dropped out of the study due to protocol violation involving inadequately longer compression time. Hence, the study was completed in 54 patients, and the analysis was performed on their results. Baseline characteristics and perioperative data are shown in Table 1. Female predominance was noted in both groups. Mean age was higher in the group AA (72.3 vs 68.0 years). Serial perioperative change in
Baseline Characteristics and Perioperative Data.
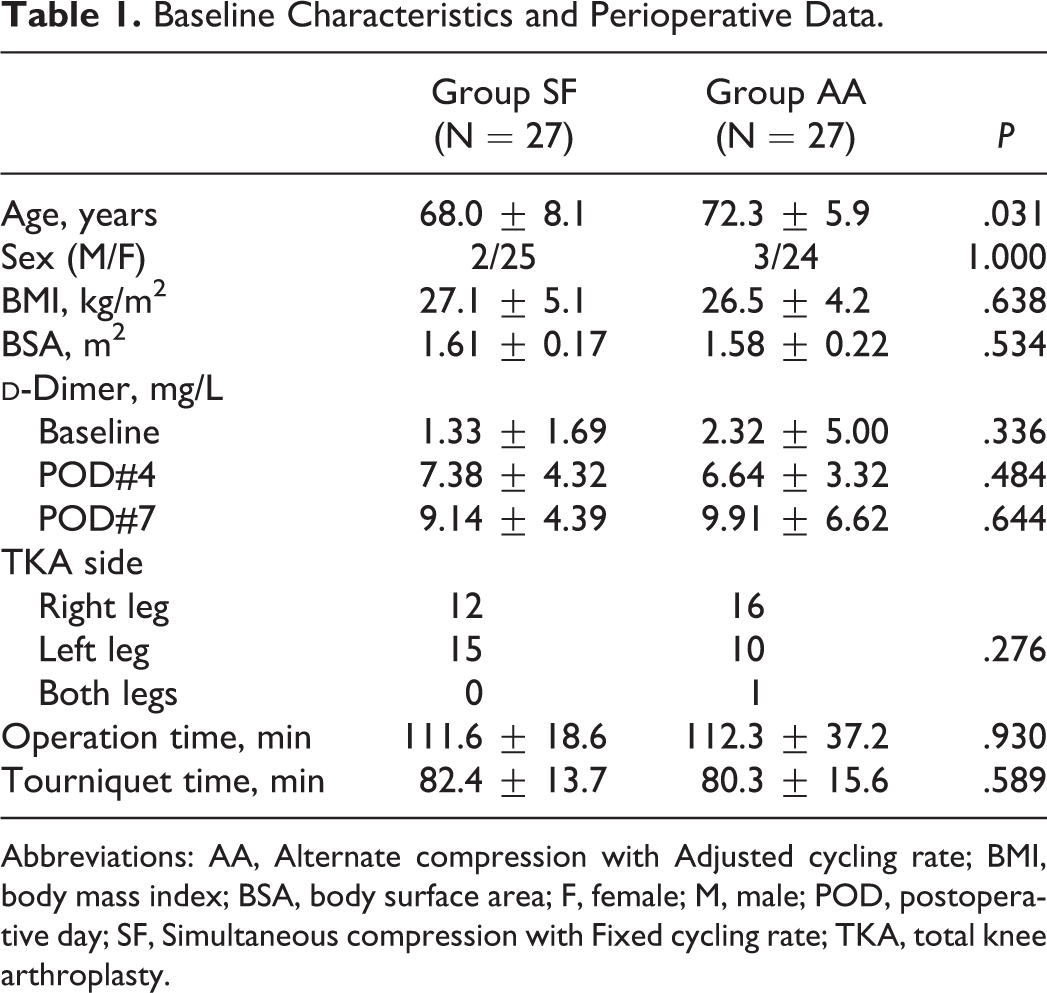
Abbreviations: AA, Alternate compression with Adjusted cycling rate; BMI, body mass index; BSA, body surface area; F, female; M, male; POD, postoperative day; SF, Simultaneous compression with Fixed cycling rate; TKA, total knee arthroplasty.
Incidence, Distribution, and Follow-Up of DVT
The DVT developed in 29 (53.7%) patients. Of them, 15 (55.6%) were from group AA and the other 14 (51.9%) were from group SF. Except for 1 popliteal vein involvement in each group, the detected thrombus were all isolated calf DVT without symptoms. Pulmonary CTA was performed in 2 patients with popliteal vein thrombosis, and it demonstrated no pulmonary embolism. Most of the calf DVTs involved multiple sites including axial veins (6 in group AA vs 8 in group SF). With regard to the other calf DVTs involving single lesion, anterior tibial, posterior tibial, peroneal, tibioperoneal, and calf muscle branch vein were involved in 1, 1, 3, 1, and 2 patients in group AA and in 0, 0, 2, 1, and 2 patients in group SF, respectively. The majority (72.4%) of the DVTs developed on the ipsilateral side of the operation (12 patients in group AA and 9 patients in group SF). The patients with DVT began to receive chemical antithrombotic therapy according to the protocol. The patients without DVT continued to receive IPC until they were discharged (duration of IPC: 16.4 ± 5.4 days). Eventually, all the patients discharged themselves without symptoms of venous thromboembolism. Three-month follow-up CTA was performed in 62% (18 of 29) of the patients with DVT. As for the 2 patients with popliteal DVT, a compression ultrasound was added to the investigation. As a result, 3 (16.6%) patients still showed thromboses, all of which were reduced in extent and remained only in calf muscle branch vein.
Comparison of Venous Hemodynamic Parameters
A total of 108 limbs was analyzed to compare the venous hemodynamics between the 2 groups. The limbs of the 2 groups were well balanced with respect to baseline venous hemodynamic profiles including mean velocity (MV), PV, PVF, and TVF. These venous velocities and volume flows were enhanced 2 times or more after IPC in both the 2 groups (Figure 1). These significant enhancements were observed both in the operated and in the nonoperated legs. The enhancement degrees of several parameters including augmented PVF, ETV, and EPV were significantly larger in group SF than in group AA. When the accumulated volume flows as indicated by ETV and EPV were corrected by body surface area (BSA), the significant differences between the groups were preserved. The mean value of the ETV index (ETV/BSA) of group SF was 1.7 times higher than that of group AA (4151.8 ± 2280.7 vs 2448.3 ± 1212.4 mL/h; P < .001), and the EPV index (EPV/BSA) was 1.6 times higher in group SF (593.9 ± 247.0 vs 371.5 ± 171.9 mL/h; P < .001; Table 2).
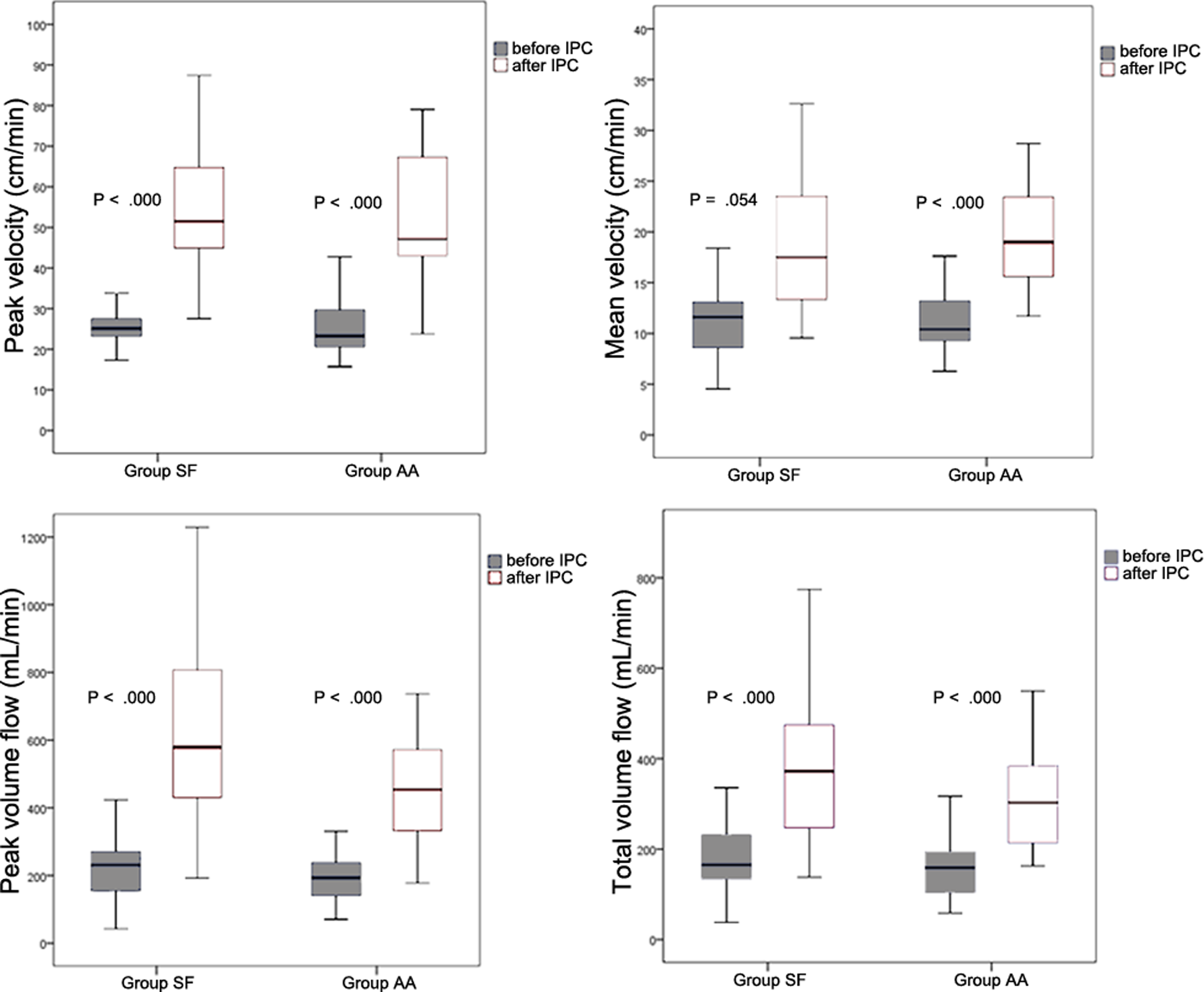
Flow velocity and volume flow enhancement after pneumatic compression in operated limbs.
Comparison of Venous Hemodynamic Parameters After Pneumatic Compression.
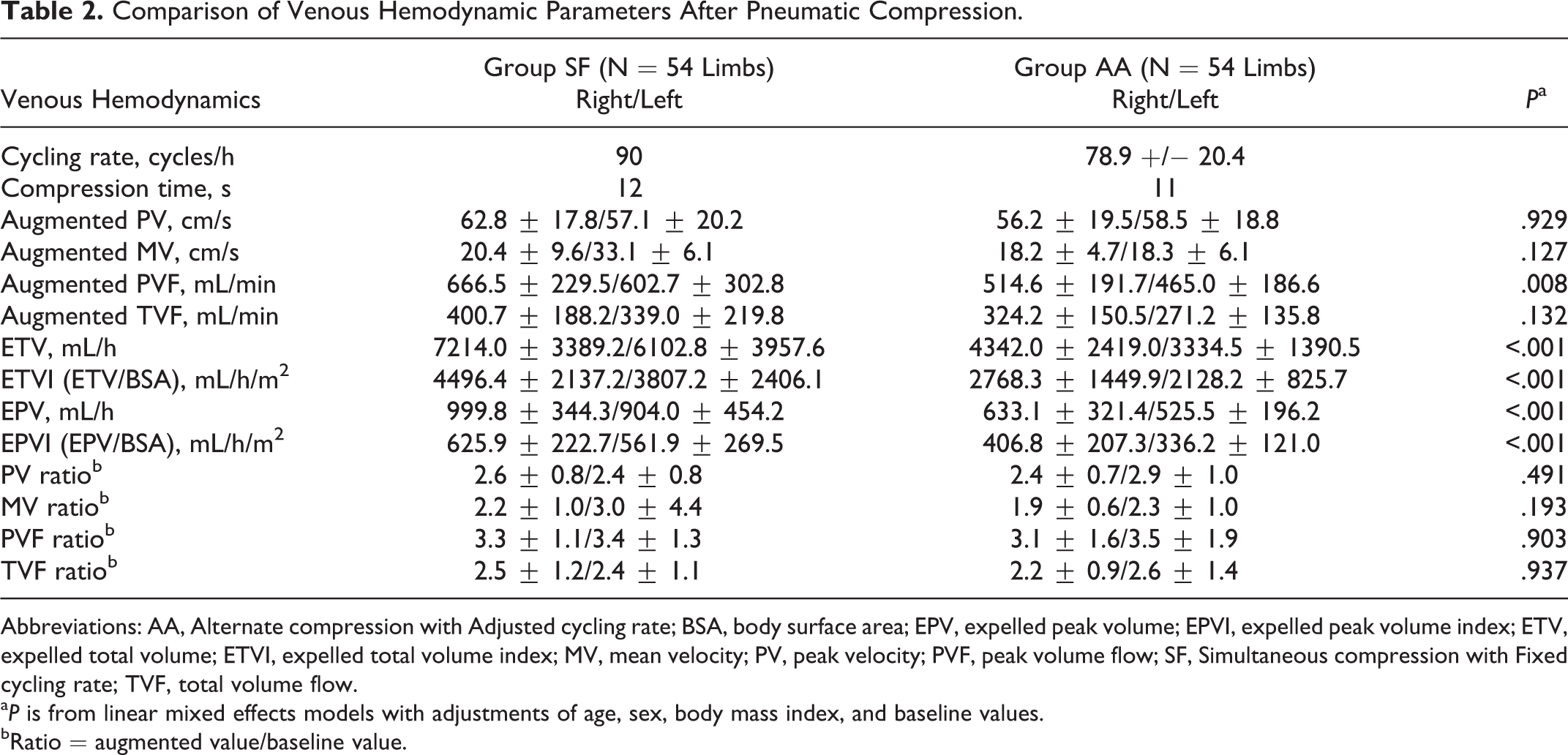
Abbreviations: AA, Alternate compression with Adjusted cycling rate; BSA, body surface area; EPV, expelled peak volume; EPVI, expelled peak volume index; ETV, expelled total volume; ETVI, expelled total volume index; MV, mean velocity; PV, peak velocity; PVF, peak volume flow; SF, Simultaneous compression with Fixed cycling rate; TVF, total volume flow.
a P is from linear mixed effects models with adjustments of age, sex, body mass index, and baseline values.
bRatio = augmented value/baseline value.
Risk Factor Analysis for DVT Development
From the risk factor analysis in 54 patients, age, BMI, type of IPC device, operation time, and tourniquet time did not influence the development of DVT. Left-sided TKA was a significant risk factor (odds ratio = 3.977, P = .046). The DVT incidence was 65.3% (17 of 26) in left-sided TKAs and 41.4% (12 of 29) in right-sided TKA. The
Generalized Linear Model for the Development of Deep Vein Thrombosis in 108 Limbs.
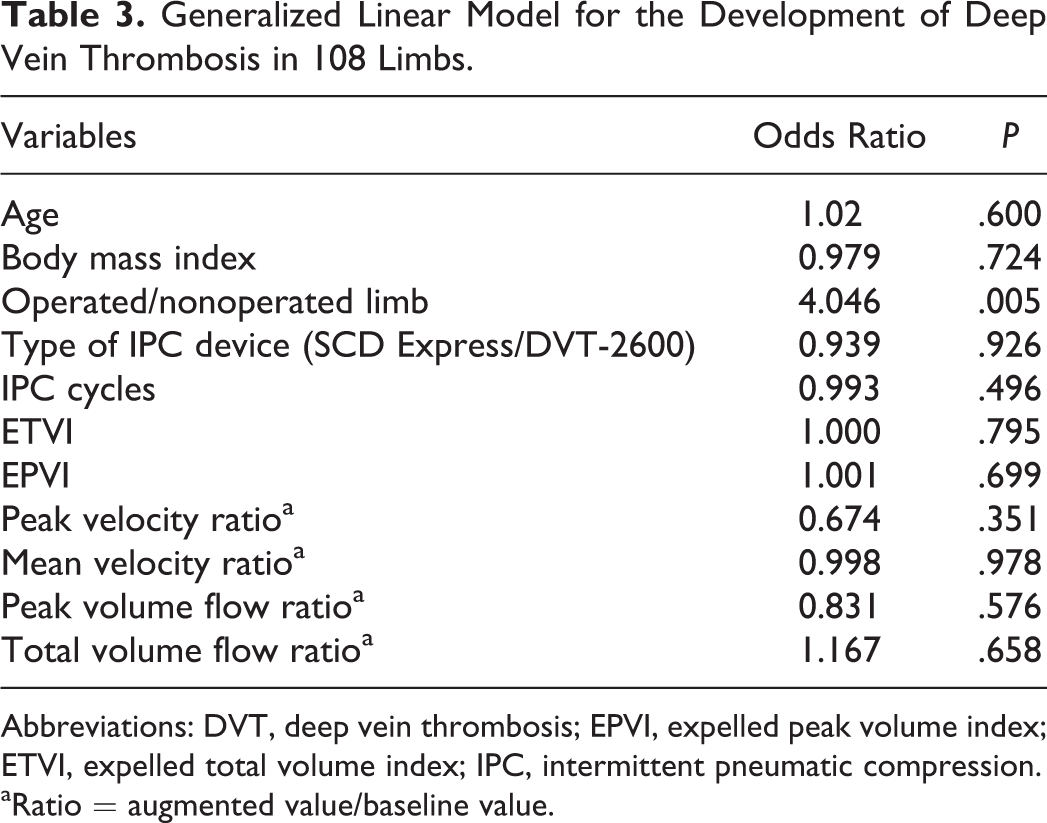
Abbreviations: DVT, deep vein thrombosis; EPVI, expelled peak volume index; ETVI, expelled total volume index; IPC, intermittent pneumatic compression.
aRatio = augmented value/baseline value.
Compliance and Complaints
All of the patients completed full-time pneumatic compression as scheduled. However, there were some complaints associated with the application of IPC. Both devices showed similar results in a survey of convenience and minor complications. Nine patients complained of increasing but well-tolerated wound pain. Five of them were from group SF and 4 from group AA. Oozing from the drain-tube removal site was reported in a patient in each group. One patient in group SF complained of nausea on the first day of pneumatic compression but it was well controlled with medication.
Discussion
In this randomized clinical trial, the simultaneous fixed cycling rate compression (group SF) provided more excellent profiles of venous hemodynamics than the alternate adjusted cycling rate compression (group AA) did in patients with TKA. However, the hemodynamic parameters were not found to be determinant factors for the development of DVT.
Simultaneous and alternate bilateral sequential compression have never been compared by other researchers, although the 2 types of compression are widely used in the IPC device market. In the literature, SCD Express showed good performance in expelling venous blood volumes for an hour. 11 However, in this study, the expelled peak and total volumes for an hour were in favor of DVT-2600 rather than SCD Express. Especially for TVF, single-cycle augmented TVF was not different between the 2 groups but the TVF accumulated for an hour and the ETV was higher in group SF mainly due to more frequent cycling rates. This implies that it may not be the refill-time adjustment but the cycling rate that plays a key role in enhancing the venous hemodynamic effects of IPC.
This study made an attempt to ascertain whether venous hemodynamic parameters were directly related with the development of DVT after TKA. Because the number of patients was not enough to compare the DVT incidence between the 2 groups, we performed overall analysis rather than intergroup comparison to investigate whether the hemodynamic parameters were determinant factors for DVT occurrence. The venous hemodynamic parameters as well as types of IPC devices were not significant factors that influenced the development of DVT. This result challenges the belief that the hemodynamic effects of IPC, such as reduced venous stasis and increased volume flow in deep veins, result in the clinical benefit of reduced DVT. Analyzing a large number of patients in a valuable comparative study, the authors could not show any difference in DVT incidence based on the method of compression, 15 which is congruous to our study. To the best of our knowledge, there has been no study to verify the direct link or detailed mechanism between hemodynamic parameters and DVT incidence in spite of the abundance of studies dealing with the hemodynamic effects of IPC and their potential direct and indirect benefits. 11,18
In both groups, postoperative thrombi were detected in more than half of the patients. However, neither iliofemoral DVT including pulmonary embolism nor symptomatic DVT was observed. The detected thrombi including the 2 popliteal thrombi finally disappeared at 3-month follow-up CTA in 87% of the patients with DVT. It is almost certain from the literature that isolated calf DVT has little clinical importance in many respects: rare clinical complication and sequela, a low recurrence rate, and a short duration of anticoagulation for treatment. 19 Considering that the frequency of proximal DVT observed in TKA varies from 4.4% to 20% in other literature, 1,20 –22 both the IPC devices were thought to play some role in the prevention of clinically significant DVT. On the other hands, the still high incidence of isolated calf DVT implies that the present IPC methods combined with graduated compression stockings may not be enough for optimal thromboprophylaxis in patients undergoing TKA.
This study evaluated bilateral limbs and revealed that nonoperated legs were also at risk of DVT development. Of the 29 patients with DVT, 8 showed contralateral involvement of nonoperated limbs. Therefore, contralateral limbs were also included in the venous hemodynamic analysis. There are not a few studies where ipsilateral contrast venography is chosen as an investigation tool. This has raised concerns that the investigators have taken no account of the potential risk of undetected DVT in the contralateral limb. A systemic review emphasized that bilateral venography evaluation should be done for the same reason, insisting that evaluation by only ipsilateral venography would require an increased sample size. 23
Multivariable logistic regression analysis showed that left-sided TKA was an independent risk factor for DVT development. This finding seems to be related to the previous observations of left-leg predominance of DVT. 24,25 The only plausible explanation for it until now has been the compression of the left common iliac vein by the right common iliac artery. Even a large-sized study that enrolled 2863 patients with isolated leg DVT and analyzed 2576 patients in the end failed to find a modulating factor for the left-sided predominance among the factors examined including obesity, age, sex, history of injury and surgery, and oral contraceptive use. 26 A close investigation into the anatomical distribution of distal DVT showed that involvement of multiple below-knee veins including muscular branches was more frequent than involvement of single axial vein like the tibioperoneal trunk. This nonaxial predominance might be one of the explanations for the rarity of clinical symptoms and the low diagnostic sensitivity of DU in isolated distal DVT.
In order to maximize diagnostic sensitivity and specificity, we performed a combined evaluation using CTA and DU. This fact must have contributed to the high DVT incidence in this study in spite of the mechanical thromboprophylaxis that was applied, compared with other data based on DU only. The DU is noninvasive, readily available, relatively low cost, and quite accurate in the detection of clots in the iliofemoral and/or popliteal vein. However, for the detection of calf thrombi after TKA, duplex is not as accurate and reliable. 27 In contrast, it is well known that contrast CTA has about 97% sensitivity and 100% accuracy. 28 An additional advantage of CTA is that when pulmonary embolism is suspected, a combined pulmonary arteriography can be obtained at the same time. On the other hand, a serious disadvantage is that streak artifacts caused by metal implants of the knee degrade the image quality and make popliteal vein evaluation difficult. Thus, DU is an optimal tool for popliteal vein evaluation after TKA.
Although several factors associated with the TKA procedure such as anesthesia type, bone manipulation, and reaming of the medullary canal have been mentioned as relevant risk factors for DVT, 29,30 they have received little attention. Some researchers have suggested tourniquet and total operation time during TKA as potential risk factors for DVT. 22,29 A tourniquet can cause retention of blood flow, endothelial dysfunction, and enhanced coagulation activity contributing to DVT. A total operation time of >120 minutes was reported to increase the risk of proximal DVT in a recent study. 22 On the other hand, both these factors did not play any role in the development of DVT in this study.
Our study has some limitations. First, the sample size was small for a statistical comparison of clinical efficacy, and it was not performed. Because the purpose of this study was not to compare the DVT incidence or clinical efficacy between the 2 IPC device groups but to know whether or not hemodynamic parameters could significantly influence the development of DVT after TKA, the sample size was initially determined by the previous hemodynamic data not by DVT incidence data. In fact, to our knowledge, there has been no such clinical data comparing these 2 methods of compression. Second, although the basis of the short duration of IPC was already described, it might have contributed to the high incidence of DVT and to the masking of the true intergroup difference. Third, this study did not investigate the late development of DVT in patients without DVT, and thus it could be claimed that the real prevalence was higher. However, sequentially repeated screening with CTA in all patients is quite limited in practice. At least the patients with DVT did not showed aggravated or newly appeared DVT at the follow-up CTA.
In conclusion, simultaneous bilateral compression with a fixed cycling rate showed the superior venous hemodynamic effects. However, there was no hemodynamic parameter that influenced the development of DVT, which was inconsistent with commonly held beliefs. Accordingly, hemodynamic superiority may not be a surrogate for better thromboprophylaxis and IPC device alone may not be so effective for the prevention of DVT. Further randomized clinical studies with large volume are required in order to confirm our findings and details of mechanism that connect physiological effects of IPC to DVT reduction should be further studied.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by a research grant from Small and Medium Business Administration of Korea and the DVT-2600 devices were supplied by DS MAREF Co., Ltd.