
Abstract
Epilepsy is a disease arising from morphological and metabolic changes in the brain. Approximately 60% of patients with seizures can be controlled with 1 antiepileptic drug (AED), while in others, polytherapy is required. The AED treatment affects a number of biochemical processes in the body, including increasing the risk of cardiovascular diseases (CVDs). It is indicated that the duration of AED therapy with some AEDs significantly accelerates the process of atherosclerosis. Most of AEDs increase levels of homocysteine (HCys) as well as may affect concentrations of new, nonclassical risk factors for atherosclerosis, that is, asymmetric dimethylarginine (ADMA) and homoarginine (hArg). Because of the role of these parameters in the pathogenesis of CVD, knowledge of HCys, ADMA, and hArg concentrations in patients with epilepsia treated with AED, both pediatric and adult, appears to be of significant importance.
Introduction
According to the recommendations of the International League Against Epilepsy and the International Bureau for Epilepsy, epilepsy should be considered a disease. Epilepsy exists in a patient who has had a seizure and whose brain, for whatever reason, demonstrates a pathologic and enduring tendency to generate recurrent seizures. 1 Epilepsy is a relatively frequent medical condition, which affects all age groups, from neonates to elder people. It is estimated that over 60 million people worldwide suffer from epilepsy. 2
The problem of epileptic seizures and associated treatment affects the daily life of patients, their social functioning, and, in the case of children, also the course of education. In about 60% of patients, seizures can be controlled by administering 1 antiepileptic drug (AED), whereas in other patients, polytherapy is necessary. 1,3 Among AEDs, there are drugs inducing cytochrome P450 (CYP) isoenzymes, including carbamazepine (CBZ), phenytoin (PHT), phenobarbital (PB), or primidone, or inhibiting them—valproate (VPA), and drugs that have no effect on CYP, including gabapentin, vigabatrin (VGB), levetiracetam (LEV), or topiramate (TPM). Oxcarbazepine (OXC), being a new generation AED, belongs to weak inhibitors of P-450 (CYP2C19), and when used concomitantly with other AEDs, it may increase their plasma concentration, thereby increasing their activity or toxicity.
The following AEDs are recommended for the treatment of focal seizures in adults: CBZ, LEV, PHT, and zonisamide, while CBZ, lamotrigine (LTG), OXC, PB, PHT, TPM, and VPA for the treatment of generalized seizures. In contrast, for the treatment of focal seizures in children, OXC is the AED of first choice and for generalized seizures—CBZ, PB, PHT, TPM, and VPA. 4,5 One of the option in the therapy of epileptic seizures is also dietary treatment. The efficacy of ketogenic diet (KD), with high lipid and protein and low carbohydrate intake, is known both in children and adults with drug-resistant epilepsy. The number of seizures in 53% of adults with refractory epilepsy treated with KD was reduced to less than 50%. In 13% of the patients, the seizures were ceased, which means the potential possibility of withdrawal of some/all AEDs. 6
Taking AEDs affects a number of biochemical processes in the body, among others it can reduce cognitive and behavioral functions. It may also contribute to an increased risk of cardiovascular diseases (CVDs), although information concerning this issue is contradictory. On the one hand, it has been demonstrated that there is a relationship between the use of AEDs and the levels of biochemical parameters (including HCys, folic acid, or lipids), which may influence the development of atherosclerosis. 7 –9 On the other hand, there are data according to which this relationship does not exist. 10
Based on the comparative measurement of the intima–media thickness (IMT) in the common carotid artery in the group of epileptic adults, it has been demonstrated that the duration of AED therapy with some drugs significantly accelerates the process of atherosclerosis. 11,12 Most AEDs increase HCys concentration, recognized by many researchers as an independent risk factor for atherosclerosis. This is the result of reduced folic acid concentration. 2,13
The aim of the present literature review was to discuss the results of available up-to-date studies concerning a possible impact of AEDs on concentrations of some selected biomarkers of endothelial dysfunction, including HCys, and new nonclassical atherosclerosis risk factors, that is asymmetric dimethylarginine (ADMA) and homoarginine (hArg).
Methodology
We searched PubMed using combinations of the following keywords: “epilepsy,” “antiepileptic drugs,” “AED,” “children,” “adults,” “homocysteine,” “ADMA,” “homoarginine,” “endothelial dysfunction,” and “atherosclerosis” (last search October 2018). We planned to focus our attention on the articles published within the last 10 years, but eventually we decided to include several important results published before 2009 to the present review. Thus, our discussion is limited to those data, which we believed are the most interesting as well as the most relevant ones. The searches were conducted by 3 authors (B.S.-H., I.K., and I.S.-B.).
Homocysteine
Homocysteine is a nonprotein sulfuric amino acid created during the transformation of methionine and cysteine as a by-product of methylation. In the human body, HCys mainly participates in oxidation–reduction reactions and thiol–disulfide exchange. Homocysteine is produced in all types of cells in the human body. However, its detoxification occurs mainly in the liver and kidneys, through remethylation or transsulfurylation. In the cells of blood vessels and skin, due to the lack of expression of enzymes in the transsulfurylation pathway, HCys is only converted by remethylation. The key role in the transformation of HCys is played by folic acid, necessary for the synthesis of tetrahydrofolate, which is a substrate of 5,10-methylenetetrahydrofolate reductase (MTHFR). The availability of folates is a condition for removing HCys. Other cofactors important for HCys metabolism are vitamins B12 (methionine synthase cofactor) and B6 (cystathionine-beta-synthase [CBS] cofactor).
Homocysteine has cytotoxic properties toward endothelial cells, causes strong oxidative stress, which stimulates the production of pro-inflammatory cytokines, and can also cause chronic inflammation. 14 Homocysteine contains a highly reactive thiol group and can modify the activity of proteins by forming disulfide bonds by reaction with cysteine side chain residues (S-homocysteinylation) or by reaction with amino groups (N-homocysteinylation). 14 N-homocysteinylation occurs at high concentrations of HCys, which then forms homocysteine thiolactone. In this way, various proteins in the blood may be modified, including albumin, fibrinogen, or hemoglobin as well as endothelial cell proteins, which then become vulnerable to free oxygen radical activity. N-homocysteinylation of the apoB-100 protein, which is a component of low-density lipoproteins (LDLs), results in the aggregation of LDL molecules, which increases their toxicity toward endothelial cells and thus accelerates the atherosclerotic process. 15 In the presence of adenosine, an increased amount of HCys leads to the formation of S-adenosyl homocysteine (SAH), which reduces the number of endothelial cell divisions. The protection against the migration of phagocytes and platelets is then impaired, as well as the production of nitric oxide (NO), which relaxes blood vessels. These are the endothelial functions that protect the vessels against the development of atherosclerosis. Nitric oxide under physiological conditions neutralizes HCys by converting it into S-nitrohomocysteine, which does not have oxidizing properties, acts as an antiaggregating agent, and widens the vessels. 14 Homocysteine induces the expression of lectin-like oxidized low-density lipoprotein receptor 1, which plays an important role in the regulation of the progression of atherosclerotic lesions and causes endothelial apoptosis and inflammation. 16
Factors Affecting HCys Levels
The normal range of plasma HCys concentration should be between 5 and 15 μmol/L, although levels of 10 to 13 μmol/L may be toxic to vascular endothelium. Data are available according to which HCys concentrations higher than 10.4 μmol/L are considered to be elevated.
17
The factors affecting HCys levels include age, sex, smoking, physiological conditions (pregnancy), chronic diseases, low physical activity, and drugs used, such as antituberculosis drugs, sulfonamides, oral contraceptives,
Hyperhomocysteinemia is a confirmed risk factor for vascular diseases both in children and adults. 13,25,26 Moderate hyperhomocysteinemia is associated with a 4-fold increase in the risk of ischemic stroke in children. 27 Disturbed HCys metabolism increases the level of soluble form of the amyloid precursor protein in the cerebrospinal fluid and may contribute to amyloidogenesis. 28 In addition, elevated HCys levels may also correlate with neural tube defects—in women with pregnancies affected by such defects, elevated plasma HCys levels indicate disruption of folate metabolism. However, in studies on mouse embryos, exposure to homocysteine thiolactone in doses of 0.5 mM or more delayed the growth and abnormalities of somatic development, but it did not increase the incidence of neural tube defects. 29
Asymmetric Dimethylarginine
Asymmetric dimethylarginine is an nitric oxide synthase (NOS) inhibitor and can compete with

Scheme of connection between homocysteine metabolism and ADMA metabolism. ADMA indicates asymmetric dimethylarginine; ATP, adenosine-5’-triphosphate; DDAH, dimethylarginine dimethylaminohydrolase; MTHFR, methylenetetrahydrofolate reductase; NADPH, reduced nicotinamide adenine dinucleotide phosphate; NOS, synthase of nitric oxide; PRMT, N-methyltransferases; ROS, reactive oxygen species; SAH-S, adenosyl homocysteine; SAMS, adenosylmethionine; SDMA, symmetrical dimethylarginine.
The bioavailability of NO decreases with increasing ADMA concentration. Nitric oxide deficiency affects a number of processes in the body, that is increases the synthesis of MCP-1 protein and promotes aggregation and proliferation of thrombocytes and inhibition of apoptosis of myocytes. Low NO levels can also inhibit angiogenesis. 30 Nitric oxide is involved in synaptic transmission in the central and peripheral nervous system.
Asymmetric dimethylarginine concentration is influenced by a number of factors, both endo- and exogenous. The most important exogenous factors include diet, age, drugs used, inter alia, in the course of diabetes or neuroleptics. One of the endogenous factors that affect ADMA metabolism is HCys. It induces oxidative stress by increasing the production of reactive oxygen species. This is due to the increased oxidase activity of reduced nicotinamide adenine dinucleotide phosphate with simultaneous reduction in the concentration of thioredoxin, which protects proteins from oxidative stress by reducing disulfide bridges. 31 Experimental data indicate that HCys inhibits the activity of the enzyme catalyzing the decomposition of ADMA—dimethyl arginine dimethyl amino hydrolase, which consequently causes the accumulation of ADMA and subsequently reduces the synthesis of NO by endothelial cells 32 (Figure. 1).
It is suggested that increased ADMA concentrations influence the progression of the atherosclerotic process. Asymmetric dimethyl arginine also exacerbates oxidative stress and monocyte adhesion. Studies conducted on a large group of children indicate that ADMA levels correlate with the thickness of the carotid IMT complex.
33
Elevated plasma ADMA levels in atherosclerotic patients are related to the degree of vascular endothelial dysfunction and disease progression.
34,35
A study by Lu et al
36
has shown that ADMA levels and the
The data concerning the correction of ADMA concentration are not as numerous as in the case of HCys. However, the results of studies by Sydow et al
40
indicate that B vitamins do not lower the level of ADMA in contrast to HCys.
Homoarginine
Homoarginine is a naturally occurring amino acid derived from lysine. It is mainly produced in the kidneys, and in most body fluids, it occurs in low concentrations. An additional methyl group makes it different from
Biomarkers of Endothelial Dysfunction in the Course of Epilepsy
Homocysteine
It is suggested that HCys together with its metabolite, which is homocysteine acid formed in the oxidation process, can antagonistically affect the receptor for N-methyl-
Literature data indicate that pharmacotherapy with AEDs affects HCys concentration, both in adult and pediatric patients. 7,8 Hyperhomocysteinemia is observed in more than 15% of children treated with AEDs, and its risk may increase during polytherapy (combination of 2 AEDs such as CBZ, VPA, PHT, VGB, OXC, TPM, LTG, and clobazam). 17 In the group of 78 epileptic children from the south of Italy (45% treated with monotherapy), the mean HCys value in patients was significantly higher than the mean in the control group (12.11 vs 7.4 μmol/L) and the decreased folate concentration was significantly correlated with increased HCys levels. 49 The results of study by Sener et al 50 confirm the effect of AEDs on plasma HCys concentration. Patients with newly diagnosed epilepsy were characterized by significantly lower HCys levels compared to 3 groups of patients treated with CBZ, PHT, and VPA monotherapy, respectively (the mean duration of AED treatment was 6.5 ± 6.2 years), as well as in relation to healthy volunteers. 50
Antiepileptic drugs may result in increased HCys concentration, inter alia, by affecting the absorption of cofactors necessary for its remethylation as well as inducing hepatic enzymes, which determine the level of folates. In addition, the metabolism of AEDs, and in particular their hydroxylation, increases the consumption of folates, thus lowering their level in plasma, which in turn is associated with hyperhomocysteinemia. In 2 groups of epileptic children treated with VPA and CBZ, both in monotherapy, the early effect of AED treatment on HCys metabolism was observed. Its concentration significantly increased in both groups after 20 weeks of therapy. 7 However, the authors observed that the level of folates and vitamin B12 increased significantly in the VPA group, whereas it significantly decreased in the CBZ group. Similar conclusions have been drawn by Gorjipour et al 9 based on a meta-analysis of 10 papers showing that CBZ and sodium VPA increase the level of HCys, with CBZ also lowering the level of folates. However, there is no relationship between taking VPA and reduced folic acid concentration. Another meta-analysis has also confirmed a significant effect of VPA on HCys concentration, but it has been shown that this compound does not correlate with age and ethnicity. 51 In contrast, the study of Kumar et al, 52 conducted in the group of epileptic children, has not demonstrated a relationship between CBZ therapy and the levels of HCys and folates, whose concentrations did not increase significantly after a 6-month treatment with a dose of 10 to 20 mg CBZ/kg/day. In turn, the meta-analysis of Rezaei et al 10 has not confirmed the effect of OXC monotherapy on HCys, vitamin B12, and folate concentrations, compared to the control group. However, this observation may be due to the fact that OXC belongs to new AEDs that do not show an effect on CYP or the effect is relatively weak.
The relationship between using new AEDs and HCys concentration was also studied in Korean patients with newly diagnosed epilepsy treated with LEV, OXC, or TPM monotherapy. 53 A statistically significant increase in HCys concentration has been observed during the therapy with each drug, but these changes were in the range of physiological concentrations. Similar correlations have been demonstrated in the case of LDL cholesterol and apolipoprotein B. The authors have observed a reduced folate level in patients taking OXC, whereas the level of folates has not changed significantly in those treated with LEV and TPM. 53 On the other hand, normal serum HCys levels have been observed in the groups of patients with epilepsia treated with LTG and LEV. 54 Similar results have been obtained in the study of Ni et al, 22 in which no relationship has been found between LTG monotherapy and HCys levels.
Because epilepsy occurs in 20% to 50% of patients with brain atrophy, the role of hyperhomocysteinemia in this phenomenon is also observed. In the study by Gorgone et al, 55 brain atrophy has been found in 30% of patients and was associated with both increased HCys levels and the use of a combination of several AEDs. Therefore, it seems that there is a correlation between neuronal damage by HCys and oxidative stress and excitotoxicity. The influence of AED therapy and HCys concentration on the level of intelligence in pediatric patients with epilepsy is also interesting. It has been shown that children treated with AED polytherapy had significantly lower intelligence quality (IQ) values compared to those treated with 1 AED, whereas plasma HCys concentrations were not significantly related to IQ scores. 56 Previously, patients with epilepsia with long-term antiepileptic treatment were found at 3-fold higher risk of ischemic stroke than control group. 57 It may be related to the influence of AEDs on the levels of lipids or other atherosclerotic biomarkers. Especially high risk of stroke was demonstrated in patients receiving PHT compared to those treated with CBZ. 58
Homocysteine concentration can be easily corrected by supplementation with group B vitamins or vitamin B-rich diet. Using folic acid, it is possible to get a 25% to 30% reduction of HCys levels and an additional 7% reduction is provided by B12 supplementation. 59 In patients with peripheral arterial occlusive diseases after 8-week supplementation with B vitamins, HCys concentration decreased from the initial level of 15 to 8.7 μmol/L. 40 Folic acid supplementation significantly lowers HCys levels also in patients with epilepsia. 17,60 The use of folic acid before and during pregnancy can also reduce the risk of fetal brain damage caused by ischemic stroke. 61
Asymmetric Dimethylarginine
Asymmetric dimethylarginine can affect the proper level of neuronal excitability because it induces changes in the metabolism of arginine, which is a precursor of excitatory and inhibitory neurotransmitters (glutamate and γ-aminobutyric acid, respectively), and in this way may promote the occurrence of epileptic seizures.
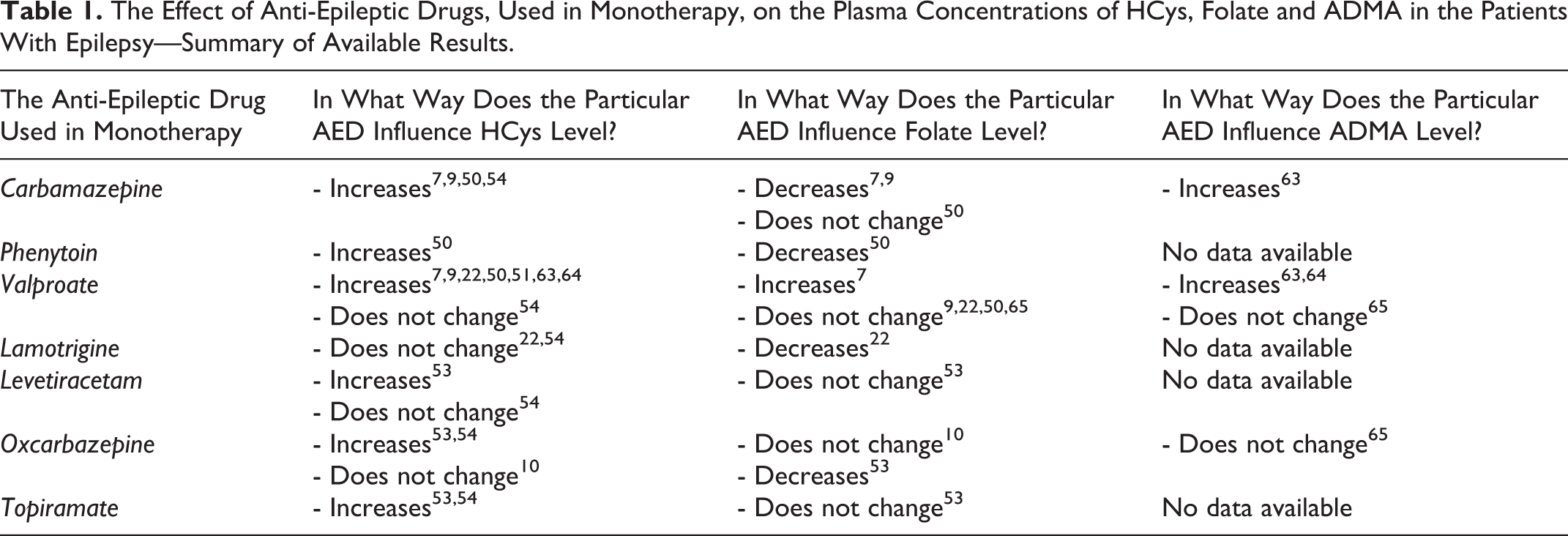
A study of Śnieżawska et al 62 has shown that AED pharmacotherapy in adult patients (68% patients treated with monotherapy and 32% patients treated with polytherapy) leads to elevated levels of both ADMA and HCys. Similarly, in 2 groups of patients with epilepsia from Turkey treated with VPA and CBZ, respectively, ADMA levels significantly increased after the therapy. 63 In contrast, HCys levels after AED treatment were higher in both groups, but only significantly in the VPA group. 63 Similar results were obtained in groups of pediatric patients with epilepsy. Children treated with VPA monotherapy were characterized by higher serum ADMA and HCys levels compared to healthy children. 64 Significantly higher concentrations of ADMA, HCys, and triglycerides were observed in patients who had received VPA therapy for more than 2 years versus patients treated below 2 years as well as in those who received VPA at a dose of 25 to 30 versus 20 mg/kg/d. 64 Other studies of Turkish children with epilepsy have shown that the use of OXC may cause the risk of hyperhomocysteinemia. However, no statistical differences have been found in ADMA, NO, vitamin B12, and folate levels between groups of children treated with VPA, children treated with OXC, and healthy children. 65 On the other hand, a study by Tatarewicz et al 66 has shown a significant reduction in the arginine/ADMA ratio in adult patients with epilepsy treated with VPA compared to those treated with CBZ. Table 1 presents a summary of the discussed results of studies conducted in adult and pediatric patients with epilepsia relating to the effect of AED monotherapy on HCys, folate, and ADMA levels.
The Effect of Anti-Epileptic Drugs, Used in Monotherapy, on the Plasma Concentrations of HCys, Folate and ADMA in the Patients With Epilepsy—Summary of Available Results.
Homoarginine
There are very few studies on the relationship between hArg levels and epilepsy. One of the first studies, conducted by Shiraga et al 67 on a group of adult patients, showed that both the level of arginine in epileptic men and hArg levels in epileptic men and women treated with VPA were significantly lower than in those who were not treated with VPA. The published literature data show that low hArg concentrations may be related to CVDs and may increase the mortality of patients resulting from CVDs. 68,69 Patients subjected to angiography also showed differences in plasma hArg concentrations between the sexes, that is the mean level of hArg was significantly higher in men than in women and was 2.7 and 2.3 μmol/L, respectively. 68
Sobczak et al
70
observed low serum levels of hArg and high serum levels of ADMA in smoking men compared to nonsmokers. This may suggest the antagonistic effect of hArg and ADMA in the cardiovascular system.
71
In older patients, the concentrations of
Summary
Knowledge of HCys, ADMA, and hArg levels in patients with epilepsia, both children and adults, seems to be of great importance since the usage of AEDs may affect their concentrations. The above parameters play a role in the endothelium dysfunction, which is a crucial event in the pathogenesis of CVDs. Over half of the patients affected by epilepsy are treated with a combination of several AEDs, thus awareness on this subject may be helpful in the prevention of CVD. Routine monitoring of serum ADMA and HCys levels may be particularly beneficial for patients receiving long-term therapy, especially in children with concomitant risk factors for CVDs. Usage of AEDs together with other risk factors for vascular disorders, occurring during the life of children with epilepsia, may predispose the patients to development of early vascular problems. Treatment with B vitamins, mainly folic acid, would be a safe and cheap way to decrease the elevated level of HCys in patients with epilepsia taking AEDs and in turn primary prophylaxis of vascular disorders.
From the clinical and practical point of view, future studies should be focused not only on assessing which of the biomarkers of endothelial dysfunction appear during treatment with any AED, but whether such an appearance is related to the dose of the drug or the duration of the therapy. It would be also interesting to observe whether the elevated levels of the discussed biomarkers increase the risk of cardiovascular events in patients taking AED compared to people who have not been treated with AEDs at an adequate age of their lives. This, however, would involve long-term follow-up studies.
Footnotes
Authors’ Note
B.S.-H., I.S.-B,. and I.K. were involved in the literature search. A.S. and B.D. provided advice on all aspects of the study. All authors were involved in the manuscript preparation with a significant participation of B.S.-H., I.S.-B,. and I.K. All authors edited and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.