
Abstract
There is limited data on the role of hyperhomocysteinemia as a risk factor for cerebral veno-sinus thrombosis (CVT) in Indians. We examined the association between plasma homocysteine (Hcy), methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism, and CVT in 185 patients with aseptic CVT (puerperal 80 and nonpuerperal 105) and 248 healthy controls (puerperal 67 and nonpuerperal 181). Fasting Hcy was higher in patients compared to controls (20.25 ± 5.97 vs 9.81 ± 5.19 μmol/L, P < .001) and associated with 4.54-fold (95% confidence interval [CI]: 2.74-7.53) increase in risk of CVT. Risk was higher in puerperal (odds ratio [OR]: 8.7, 95% CI: 2.73-26.91) compared to nonpuerperal CVT (OR: 3.82, 95% CI: 2.09-6.96). Plasma Hcy was higher in MTHFR 677TT compared to 677CT and 677CC genotypes (34.44 ± 32.8 vs 25.81 ± 33.3 vs 18.50 ± 23.7 μmol/L, respectively, P < .001), but the risk associated with MTHFR 677TT was insignificant (OR: 1.91, 95% CI: 0.53-7.06). We conclude that hyperhomocysteinemia is a risk marker for Indian patients with aseptic CVT. MTHFR 677TT genotype is not linked with CVT but is a determinant of plasma Hcy.
Introduction
Thrombosis of the cerebral veins and dural sinuses, generally considered an uncommon entity in the developed world, is not so rare in India. 1 The etiology of cerebral veno-sinus thrombosis (CVT) is multifactorial, involving acquired and genetic factors and diverse conditions have been recognized as risk factors for this condition. 2,3 Although local causes such as brain and sinus trauma, surgery, malignancy, and infection are well-described precipitating causes of CVT, these variables do not account for all cases. 4 In the recent past, hyperhomocysteinemia has been identified as an independent risk factor for venous thrombosis. 5 –7 Homocysteine (Hcy) is a thiol amino acid resulting from demethylation of methionine, an essential amino acid derived from dietary proteins. Hyperhomocysteinemia can result from genetic and/or nutrition-related disturbances in Hcy metabolism. Among genetic determinants, a homozygous substitution of cytosine by thymine at position 677 of the gene encoding methylenetetrahydrofolate reductase (MTHFR) results in decreased enzyme activity and may predispose to elevated plasma Hcy concentrations. 8 The few systematic studies that have evaluated the role of hyperhomocysteinemia in CVT show that elevated plasma Hcy increases the risk of CVT by 4- to 5-folds. 9,10 There is limited published data on the role of hyperhomocysteinemia as a risk factor for CVT in Indians. 11,12
Homozygosity for the C677T polymorphism in the MTHFR gene has been proposed as an independent risk factor for CVT in some studies, 9 whereas others have found no such association. 10 In a pilot study of 60 patients, we found that hyperhomocysteinemia was associated with increased risk of puerperal CVT. 11 We therefore attempted to determine the association of hyperhomocysteinemia and the MTHFR C677T polymorphism in patients with CVT, both puerperal and nonpuerperal, clarify the relationship between the MTHFR genotype and plasma Hcy, and evaluate their contribution to the risk for aseptic CVT occurring in the South Indian population.
Materials and Methods
The study was approved by the review board of the National Institute of Mental Health and Neuro Sciences (NIMHANS), Bangalore, India. Written informed consent was obtained from all participants/spouses for participation in this study. Patients diagnosed with aseptic CVT and treated in the Stroke Unit of NIMHANS were investigated. The diagnosis of CVT was confirmed by neuroimaging studies such as magnetic resonance imaging/computed tomography scanning, and magnetic resonance venography/digital subtraction angiography. The type of study depended on the judgment of the caring physician. Patients were excluded when (1) neuroimaging studies were inconclusive; (2) CVT was secondary to head trauma, invasive neurosurgical procedures, sepsis, neuroinfection, or malignancy; and (3) clinical and laboratory evidence of renal, hepatic or thyroid dysfunction, malignancy, or other major systemic diseases known to predispose to thrombosis was present. Patients on any medication known to affect Hcy levels, other than B vitamins, were also excluded.
Control participants were recruited during the same period from the same population group as the cases. All controls were clinically healthy. Previous thrombosis was excluded in them by clinical history. Since in 43.2% of our cases CVT occurred within 4 weeks after delivery, selection of controls was directed toward recruiting healthy women who had a recent childbirth and were in the same puerperal period.
The baseline demographic data, history of conventional vascular risk factors, and family history of vascular events were obtained for each participant. Alcohol intake and smoking were classified according to current habitual use or not. Women were considered to be on oral contraceptives if they had taken them until a week or less before the thrombotic event, or at the time of blood collection for controls. Details regarding diet were also recorded. Puerperal CVT was diagnosed when CVT occurred during the first 4 weeks after child birth.
Venous blood samples were collected into EDTA vacutainer tubes, after overnight fasting. Samples were immediately placed on ice and after transport to the laboratory, were centrifuged at 4000 rpm for 10 minutes. Plasma was separated and stored at −80°C until analysis. Total Hcy (tHcy) was estimated by reverse phase high-performance liquid chromatography and coulometric electrochemical detection in a Shimadzu HPLC system (LC-10ADVP) using the ESA Coulochem III detector. 13 The oxidized and protein-bound Hcy was released by addition of a reducing agent, sodium borohydride, and the tHcy was measured.
DNA was extracted from peripheral blood leucocytes according to a standard protocol. 14 The MTHFR genotypes were determined according to the method of Frosst and coworkers. 8 A 198-bp fragment encompassing the region around nucleotide 677 was amplified by polymerase chain reaction (PCR), with forward primer 5′-TGAAGGAGAAGGTGTCTGCGGGA-3′ and reverse primer 5′-AGGACGGTGCGGTGAGAGTG-3′. The amplified fragment was subjected to restriction cleavage by HinfI enzyme. The C to T substitution creates a HinfI recognition sequence, and digestion of the mutant product results in 175- and 23-bp fragments. The fragment size was determined by 12% polyacrylamide gel electrophoresis. Genotyping results were confirmed by direct sequencing of the PCR products with a DNA sequencer (ABI prism 377, Applied Biosystems, USA), with a concordance rate of 100%
Statistical analysis of data was performed using the SPSS (Version 11.0) for Windows. Data of patients with CVT and controls were compared using Student t test for continuous variables, and χ 2 test or Fisher exact test for categorical variables. Hyperhomocysteinemia was defined as the levels of plasma tHcy above the 90th percentile of the tHcy value distribution in healthy controls. Estimated risk for CVT associated with hyperhomocysteinemia was expressed as odds ratio (OR) and its 95% confidence interval (95% CI). Crude OR was calculated by simple cross tabulation. Adjusted OR were obtained to determine the influence of other independent variables through multiple logistic regression analysis. The MTHFR genotype frequencies and allelic frequencies were calculated by Hardy-Weinberg formula. One-way analysis of variance (ANOVA) was employed to assess the associations between the genotype distributions and plasma tHcy concentration. Significance levels were established at a value of P < .05.
Results
All study participants were from the southern states of India and belonged to the same socioeconomic group. The baseline characteristics of cases and controls are summarized in Table 1. There was no significant difference in age or gender ratios. The mean age was 28.9 years in cases and 27.5 years in controls. The usual preponderance of CVT in young women was observed, with the percentage of female patients being 67.6%. In the patient group, 80 (43.2%) had developed CVT in the puerperal period. Among the control participants, 67 (27.0%) were in the same postpartum period. A majority of patients (79%) had headache as the first symptom. The other clinical features were seizures in 88 (47.6%), focal deficits in 87 (47%), altered sensorium in 84 (45.4%), visual deficits in 33 (17.8%), and speech disturbances in 15 (8.1%). Superior sagittal sinus was most frequently involved (75.7%), followed by lateral sinus (41.6%), cortical cerebral veins (23.8%), and deep venous system (17.8). In 45.9% of cases, 2 sinuses or more were involved. Neuroimaging studies showed a high frequency of parenchymal lesions (56.8%).
Characteristics of Patients With CVT and Healthy Controls.
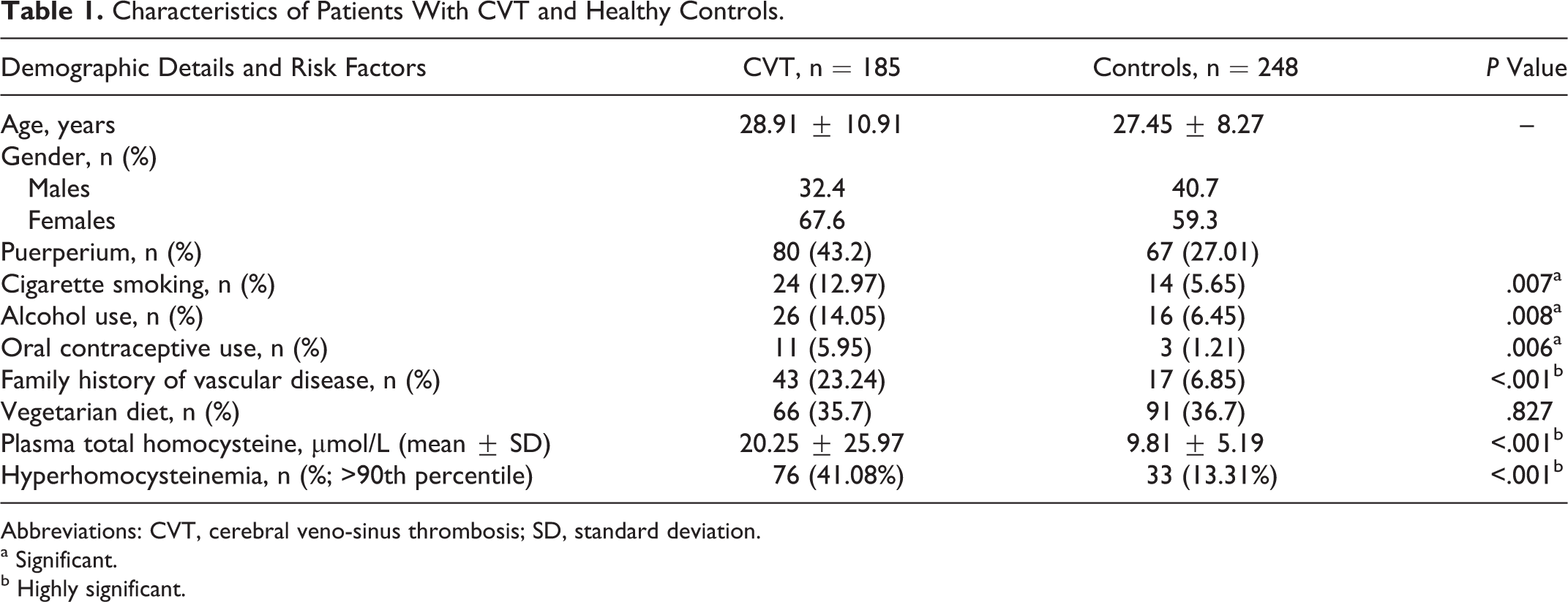
Abbreviations: CVT, cerebral veno-sinus thrombosis; SD, standard deviation.
a Significant.
b Highly significant.
The conventional risk factors for venous thrombosis such as cigarette smoking, alcohol intake, oral contraceptive use, and family history of vascular disease were significantly more prevalent in cases compared to controls (Table 1). There was no significant difference in the dietary habits of cases and controls (P = .827). Anemia was present in 65% of cases. Serum VDRL and vasculitis workup were negative in all patients. Seven (3.78%) patients died during hospital stay and the remaining patients were discharged after recovery. All participants in the control group were clinically normal and symptom free. In all, 8 (10%) patients with puerperal CVT and 62 (92.5%) control participants were on folate supplementation (P < .001). None of the participants in the nonpuerperal group were on B6, B12, or folate supplementation.
Fasting plasma tHcy was significantly higher in cases than in controls (median 12.90 μmol/L, mean 20.25 μmol/L, 95% CI 16.48-24.05 vs median 9.4 μmol/L, mean 9.81 μmol/L, 95% CI 7.11-13.77, respectively). Higher mean tHcy was observed in male than in female control participants (12.1 ± 4.82 vs 8.0 ± 4.84 µmol/L, P < .001) and in male patients than in female patients (29.8.9 ± 39.42 vs 15.7 ± 13.9 µmol/L, P < .001). When plasma tHcy >15.4 μmol/L (90th percentile) was used as the cutoff to define hyperhomocysteinemia, it was observed that it was more prevalent in patients with CVT compared with control participants (41.1% vs 13.31%; P < .001; Table 1). Hyperhomocysteinemia was associated with a crude OR of 4.54 (95%CI: 2.77-7.47) for overall CVT. After adjustment, the association was not attenuated (OR: 4.538; 95% CI: 2.74-7.53).
As shown in Figure 1, in the control participants the mean plasma tHcy was significantly lower in those in the puerperal period compared to those in the nonpuerperal group (5.69 vs 11.39 μmol/L; P < .001). Plasma tHcy was significantly elevated in puerperal CVT cases compared to puerperal controls (15.84 vs 5.69 μmol/L P < .001) and in nonpuerperal CVT cases compared to nonpuerperal controls (23.62 vs 11.39 μmol/L P < .001). In the puerperal group, 40% of CVT cases and 5.97% of healthy controls had hyperhomocysteinemia (OR: 10.5, 95% CI: 3.48-31.71, P < .001). In the nonpuerperal group, hyperhomocysteinemia was present in 41.9% of cases and 16.02% of controls (OR: 3.49, 95% CI: 2.02-6.03, P < .001). The adjusted ORs were 8.57 (95% CI: 2.73-26.91) for puerperal CVT and 3.82 (95% CI: 2.09-6.97) for nonpuerperal CVT (Table 2).
Odds Ratio for CVT With Elevated Homocysteine.
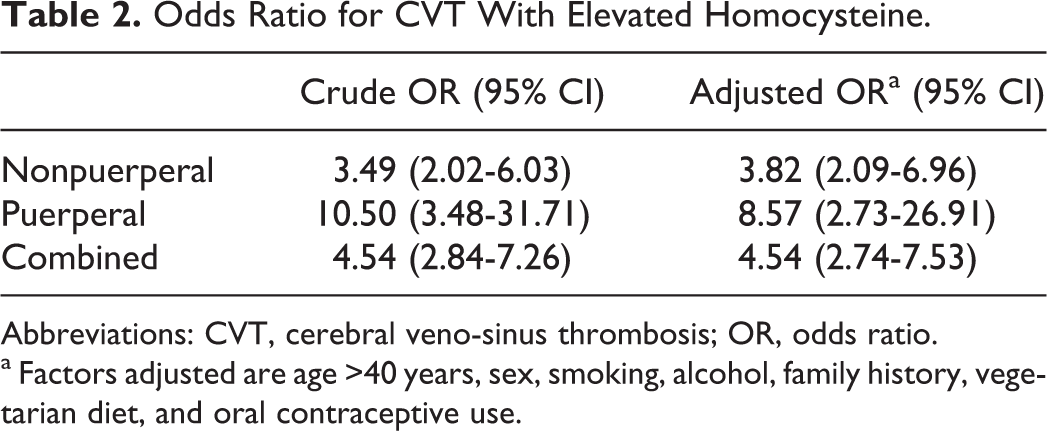
Abbreviations: CVT, cerebral veno-sinus thrombosis; OR, odds ratio.
a Factors adjusted are age >40 years, sex, smoking, alcohol, family history, vegetarian diet, and oral contraceptive use.
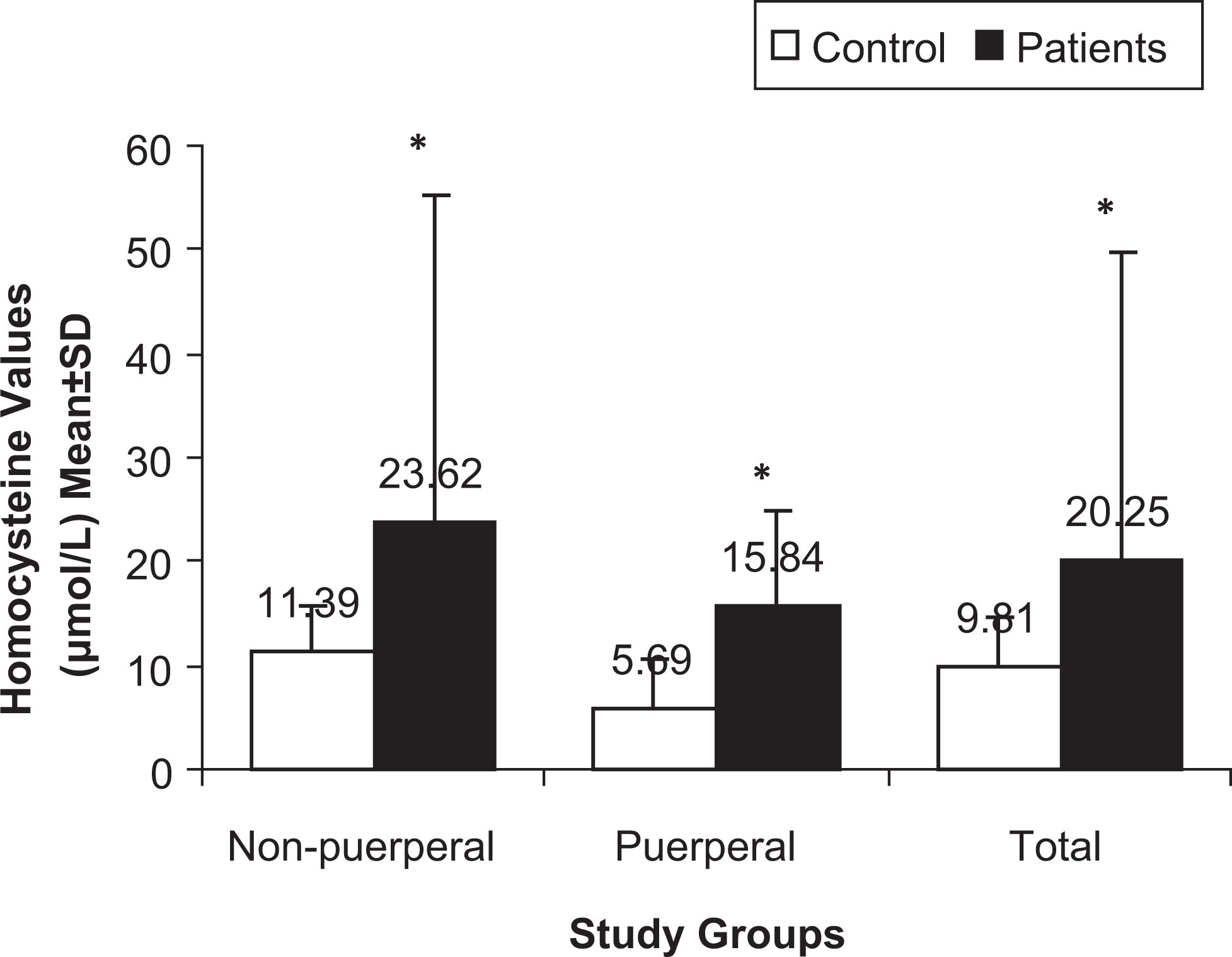
Pasma total homocysteine (mean ± standard deviation [SD]) in nonpuerperal, puerperal, and total study groups. *Highly significant P < .001.
Multivariate logistic regression analysis for determinants of plasma tHcy levels adjusted for confounding factors showed that age, smoking, alcohol consumption, oral contraceptive use, vegetarian diet, and family history had no effect on plasma tHcy. Male gender showed a trend toward significance (P = .075). When plasma tHcy was divided into tertiles with cutoffs of 7.32 μmol/L for the lowest tertile and 11.5 μmol/L for the middle tertile, significantly higher number of patients were in the highest tertile compared to the lowest tertile (55.7% vs 17.8%, P < .001). Furthermore, there were more cases than controls in the highest tertile (55.7% vs 33.5%, P < .001). As shown in Figure 2, the crude OR (95% CI) for CVT in participants in the highest tertile was 2.49 (1.68-3.95). When adjusted for gender, age, and the other vascular risk factors the OR remained significant at 3.13 (2.02-4.84), P < .001.
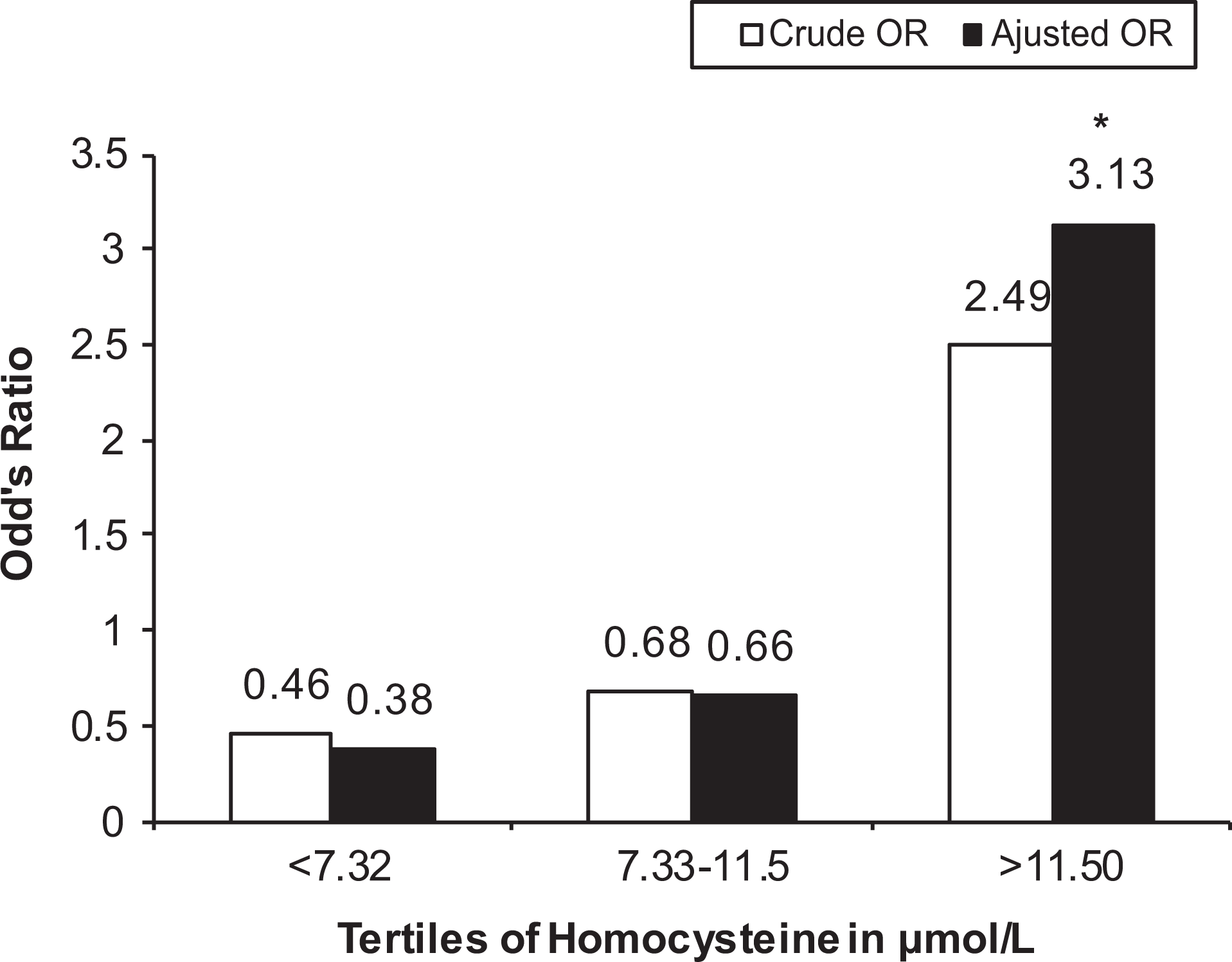
Association between tertiles of plasma homocysteine and risk of cerebral veno-sinus thrombosis (CVT). *Highly significant P < .001.
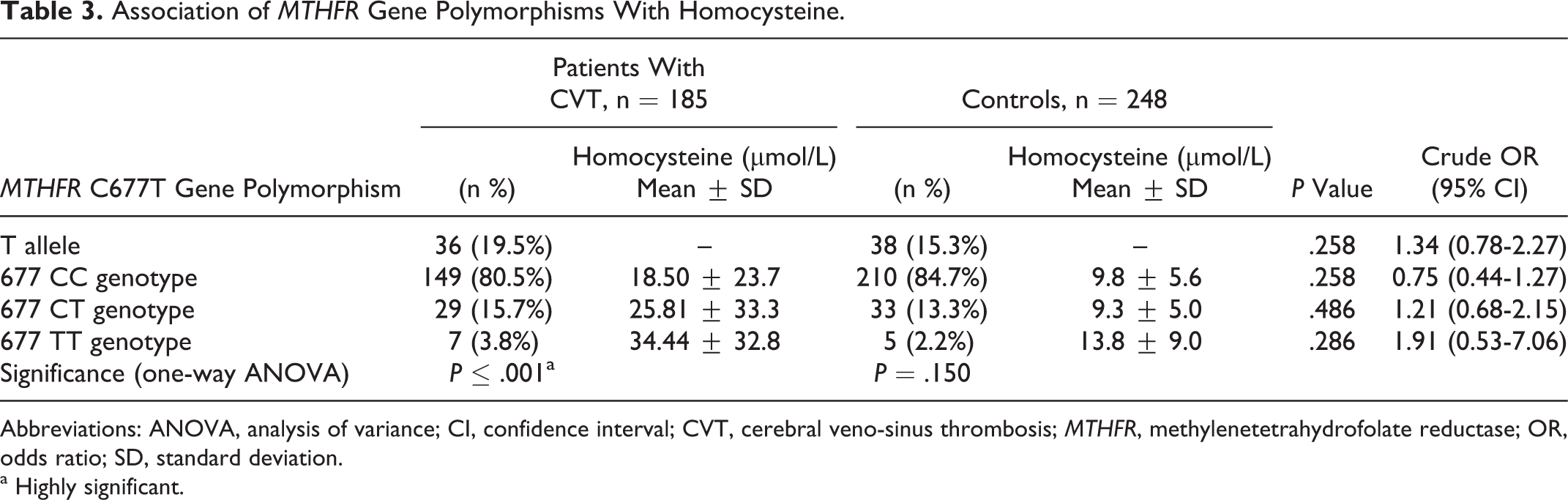
The frequency of the MTHFR 677T allele was 19.5% in cases and 15.3% in controls with no significance (P = .258, OR: 1.34, 95% CI: 0.78-2.27). There were 149 (80.5%) cases versus 210 (84.7%) controls with MTHFR 677CC genotype, 29 (15.7%) cases versus 33 (13.3%) controls with MTHFR 677CT genotype, and 7 (3.8%) cases versus 5 (2.2%) controls with MTHFR 677TT genotype. There was no significance of all genotypes in cases compared with controls (P = .258, .486,.286, OR, 0.75, 1.21, and 1.91, respectively, Table 3). Comparison of participants carrying the 677TT genotype with those with either CT or CC genotype revealed a trend of an association of the TT genotype with CVT, but it was not statistically significant, P = .286; OR:1.91 (95% CI: 0.53-7.06). One-way ANOVA test showed that MTHFR genotype was a significant determinant of plasma tHcy concentration in cases (P < .001). Mean plasma tHcy concentrations in cases were significantly higher in 677TT homozygotes than in 677CT heterozygotes and 677CC homozygotes (34.44 ± 32.8 vs 25.81 ± 33.3 vs 18.50 ± 23.7 μmol/L, respectively, P < .001; Table 3).
Association of MTHFR Gene Polymorphisms With Homocysteine.
Abbreviations: ANOVA, analysis of variance; CI, confidence interval; CVT, cerebral veno-sinus thrombosis; MTHFR, methylenetetrahydrofolate reductase; OR, odds ratio; SD, standard deviation.
a Highly significant.
Discussion
The principal findings of this study were that (i) elevated plasma tHcy was associated with CVT and contributed to increased risk for both puerperal and nonpuerperal aseptic CVT, the risk being higher in puerperal compared to nonpuerperal CVT; (ii) the MTHFR C677T polymorphism, though not associated with a risk of CVT, contributed to significantly higher plasma tHcy in CVT cases in the Indian population.
In an early study on CVT, Martinelli and coworkers 9 have reported that in patients with hyperhomocysteinemia, the risk of CVT is increased 4-fold (OR: 4.2, 95% CI: 2.3-7.6). Similarly, a meta-analysis of 4 case–control studies 15 showed that the pooled OR for CVT in patients with hyperhomocysteinemia was 4.07 (95% CI: 2.54-6.52; P < .001). Results of our study are consistent with these studies showing an OR of 4.538 (95% CI: 2.74-7.53) for CVT in our participants with hyperhomocysteinemia. We also found that there were significantly more patients in the top tertile of plasma tHcy compared to lower tertiles. A recent Indian study has found hyperhomocysteinemia in 18.2% of patients with CVT. 12 In our study, although controls were chosen from the same population group as cases, the baseline population could have included groups with different risks of developing CVT and any disparity within the sample has the potential to affect the OR. Since the postpartum state is an important risk factor for CVT, we recruited healthy women who were in the same postpartum period as the women with puerperal CVT as controls. However, we have not tested for genetic thrombophilic risk factors, such as protein C, protein S, and antithrombin, which is a potential limitation of our study.
Higher mean plasma tHcy has been previously reported from India and other developing countries. 16,17 In this study, the mean plasma tHcy in our healthy nonpuerperal controls was higher than that in Japanese, 17 Europeans, 18 and Americans 19 but similar to previous reports in Indians. 20 Several reasons have been suggested for the higher tHcy in developing countries like India, including the high prevalence of undernutrition resulting from lower economic status and religious and social customs observed in various regions of India.
Previous studies have indicated that gender and age are major determinants of plasma tHcy levels. We also demonstrated a trend toward significance for male gender. Other conventional risk factors such as cigarette smoking, alcohol intake, oral contraceptive use, and family history of vascular disease, did not show significant association with hyperhomocysteinemia in our study though it has been reported in other studies. 21,22 Exclusion of animal products in vegetarian diets has been suggested to cause vitamin B deficiencies and elevation in plasma tHcy concentration. Vegetarianism is practiced by a considerable number of people in India. However, no such association between vegetarian diet and plasma tHcy was observed in this study. The lack of difference could be attributed to the very small portions of meat consumed by a majority of Indians who take a mixed diet, compared to an average adult in the developed countries.
The C677T polymorphism in the MTHFR gene has been suggested as a candidate risk factor for vascular disease, although results are controversial. 8,23 The MTHFR C677T polymorphism was not associated with overall CVT in this study. This is consistent with the previous studies conducted in Italians 24 and Mexicans. 10 A crucial point to note is that the prevalence of the TT genotype in healthy participants in our study is lower than that reported in Europeans and Mexicans (11.1%) but similar to that reported in previous studies in Indians. 12,20
On assessment of the contribution of the MTHFR C677T genotype to circulating Hcy levels, we found that plasma tHcy was significantly higher in patients with CVT with the thermolabile MTHFR 677TT genotype as expected but the increase was not significant in healthy controls with this genotype. It has been suggested that the influence of this polymorphism on plasma tHcy is more apparent in participants with lower folate levels. 10,25 It is therefore likely that patients with CVT had lower folate than healthy controls.
Puerperal CVT is reported very frequently from the Indian subcontinent, with an incidence of 5 per 1000 deliveries in south India. It is 10 to 12 times commoner in India compared to the west. 26 CVT associated with pregnancy/puerperium is also common in Mexico, where it forms 60% of cases. 27 In the present study, 43.2% of CVT cases were associated with puerperium, and hyperhomocysteinemia increases the risk of puerperal CVT by 8.57-fold. A hypercoagulable state and stasis of intracranial blood flow with coexistent dehydration, infection, and vessel wall injury occurring during the postpartum period have been considered as important factors for the high prevalence of CVT during this period. 28 It is therefore possible that preexisting prothrombotic conditions like hyperhomocysteinemia may accelerate thrombosis and increase the risk of CVT and account for its high prevalence in India.
Deficiency of the B vitamins, folate, B12, and B6, are the nutritional causes of hyperhomocysteinemia. Of these, folate has been implicated as the most important determinant of plasma tHcy levels. 29 During pregnancy, there is a considerable increase in vitamin requirements and unsupplemented pregnancies are at risk of folate deficiency. In our study, inadequate folate supplementation reported by a significant number of the patients with puerperal CVT could have contributed to a deficiency in folate. Unfortunately, plasma vitamin B6, B12, and folate levels were not determined in all participants, which might be an important limitation of this study.
Several studies have reported that plasma tHcy is lower in normal human pregnancy than in the nonpregnant state. 30,31 This was observed in our women also, the puerperal group having significantly lower tHcy compared to nonpuerperal group. The reduction in tHcy is likely to be a physiological effect of pregnancy, with several factors contributing. 32 It is possible that the changes in blood volume and hormone concentrations in pregnancy combined with the vitamin supplementation during pregnancy may play a substantial role in lowering plasma tHcy.
Various experimental data suggest that Hcy can promote thrombosis by various effects including increased expression of adhesion molecules, blood coagulation factor V, tissue factor and cytokines, increased platelet reactivity, inhibition of fibrinolysis, and disturbance of nitric oxide metabolism. 33,34 However, Hcy-lowering therapies have not been effective in decreasing the incidence of secondary vascular events challenging the concept of a causal relationship between Hcy and thrombosis. It is therefore unclear whether it is Hcy itself that leads to thrombosis or whether the elevation in Hcy is a result of the vascular damage. It is possible that Hcy may be a marker rather than being causally related to arterial or venous thrombosis. Other factors associated with abnormal Hcy metabolism, which may be responsible for the tendency to thrombosis observed in persons with hyperhomocysteinemia need to be investigated. 35
In conclusion, our data suggest that hyperhomocysteinemia is associated with an increased risk of aseptic CVT and could possibly contribute to the relatively high frequency of CVT, especially puerperal CVT, in India, compared to developed countries. CVT is not linked with the MTHFR polymorphism, despite an association between MTHFR and tHcy concentrations. The high prevalence of hyperhomocysteinemia could be explained by low vitamin B status in our population, which needs to be evaluated in order to determine the appropriate therapeutic approach.
Footnotes
Acknowledgment
The authors gratefully acknowledge the help in statistical analysis provided by Dr K. P. Suresh.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Indian Council for Medical Research (ICMR), New Delhi, India.