
Abstract
Pulmonary embolism (PE) is a fatal disease that arises from genetic and environmental factors. There is little evidence for low high-density lipoprotein cholesterol (HDL-C) with hyperhomocysteinemia to lead to PE. Therefore, we evaluated homocysteine levels and lipid profile in PE patients and to display risk for PE. Forty six patients with proven PE and 46 healthy controls were included in the study. Homocysteine and serum lipid levels were calculated and compared in both groups. There were no significant differences between two groups in terms of total cholesterol, triglyceride, and low-density lipoprotein cholesterol. In PE group, HDL-C levels were found significantly lower in comparison to the control group (P = .004). Mean homocysteine levels were significantly higher in PE group than in the control group (P = .001). High-density lipoprotein cholesterol levels were significantly low in which homocysteine levels were high in the PE group. We thought that low HDL-C level with hyperhomocysteinemia is susceptible to PE.
Introduction
Venous thromboembolism (VTE) is a serious and potentially fatal disease which has an incidence of 1 to 3 per 1000.1–5 Its reasons are multifactorial and risk factors may be genetic or acquired.6–8 Main acquired risk factors are immobilization, pregnancy, use of oral contraceptives, operations, malignancy, antiphospholipid antibody syndrome, and lupus anticoagulants. The mostly known hereditary thrombophilia factors are the mutation of Factor V Leiden (FVL) G1691A, methylentetrahydrofolate reductase (MTHFR) C677T, G20210A variant of the prothrombin gene, and deficiencies of protein C, protein S, antithrombin III. 9 Hyperhomocysteinemia is the factor that can be hereditary or acquired. 10
Dyslipidemia and dyslipoproteinemia are the well-known risk factors of the arterial thrombosis. 3 Lipids and lipoproteins may affect hemostasis. 1 Triglyceride elevates the level of plasminogen activator inhibitor (PAI-1).1,11 Low-density lipoprotein cholesterol (LDL-C) activates platelets and induces tissue factor expression and it impairs fibrinolysis. Lipoprotein (a) is a genetical variant of an LDL-C and causes impaired fibrinolysis. 12 High-density lipoprotein cholesterol (HDL-C) inhibits platelet aggregation, decreases viscosity, and suppresses tissue factor activity so, it behaves as anti-atherothrombotic. 1
Hyperhomocysteinemia is also a risk factor for the vascular diseases. Homocysteine induces the synthesis of procoagulant factors by vascular endothelium, potentiates the auto-oxidation of LDL-C, promotes vascular thrombosis by reducing the activation of protein C and causes platelet aggregation. It is directly toxic to vascular endothelium and stimulates the proliferation of smooth muscle cells. 13 Even a lot of previous studies investigated homocysteine and dyslipidemia as a risk factor for pulmonary embolism (PE), none of the previous study investigated these two “well-known risk factors” in the same study. With this background in mind, we aimed to investigate the role of lipid status and homocysteine level on the development of PE.
Patients and Methods
Forty-six patients with proven PE, who applied to the Department of Pulmonary Diseases of the Ankara Ataturk Training and Research Hospital between January 2004 and December 2007, were retrospectively investigated. There were 21 (45.7%) male and 25 (54.3%) female patients, and the mean age was 57.9 ± 14.9 years. The diagnosis of PE was confirmed by ventilation/perfusion lung scan or spiral computed tomography (CT). The control group consisted of 44 healthy individuals. There were no PE and deep vein thrombosis (DVT) history in the control group. Patients with history of malignancy, on lipid-lowering drugs, vitamin B12 and folic acid, were not included in the study. The patients under the age of 18 and those pregnant were also not included to the study. Serum homocysteine and serum lipid levels were measured and compared in both groups. The study protocol was approved by the local Hospital Ethical Committee.
Laboratory Tests
Lipid parameters were measured by Dimension clinical chemistry system using a Flex reagent cartridge. Accepted normal levels were <200 mg/dL for total cholesterol, 30 to 200 mg/dL for triglyceride, <100 mg/dL for LDL-C, 35 to 60 mg/dL for HDL-C. High-performance liquid chromatography (HPLC) method was used to measure serum homocysteine levels and Chromosystems (Germany) kits were used. Values between 5 and 14 µmol/L were accepted as normal. Values above 14 µmol/L were regarded as hyperhomocysteinemia.
Statistical Analysis
Variables were compared according to mean and standard deviation. Student t test is used for lipid profile and Mann-Whitney U test for homocysteine levels to find whether there was any difference between groups' means. P ≤ .05 is accepted significant. SPSS for Windows Release 11.5 (2002) statistical software was used for statistical analysis. To assess the association between PE and homocysteine and lipid parameters Logistic Regression analysis was performed.
Results
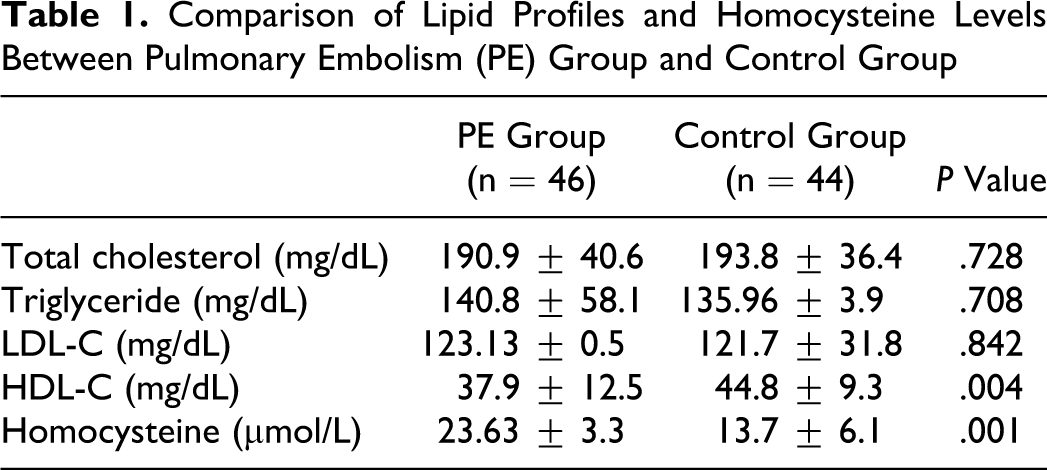
Of the patients, 16 (36.4%) were male and 28 (63.6%) were female, with a mean age of 52.5 ± 12.8 years. There was no statistically significant difference between the PE group and control group regarding age and gender (P > .05). The mean values of lipid profile and homocysteine levels are shown in Table 1 . There was no significant difference between the 2 groups in terms of total cholesterol (P = .728), triglyceride (P = .708), and LDL-C (P = .842). However, HDL-C levels were found significantly lower and homocysteine levels significantly higher in PE group compared to control group (P = .004, P = .001, respectively). Of the patients with PE, 33.3% had heterozygote MTHFR mutations, 11.9% had homozygote MTHFR mutations, and 54.8% had no MTHFR mutations. However, we did not study MTHFR mutations in control group.
Comparison of Lipid Profiles and Homocysteine Levels Between Pulmonary Embolism (PE) Group and Control Group
A multivariate logistic regression was performed on all parameters to identify the independent risk factors for PE. We found that 1 unit increase in homocysteine causes 10% increase in the risk of PE (OR, 1.097; 95% CI, 1.020 to 1.179). Moreover, 1 unit decrease in HDL-C causes 4% decrease in the risk of PE (OR, 0.956; 95% CI, 0.915 to 0.999).
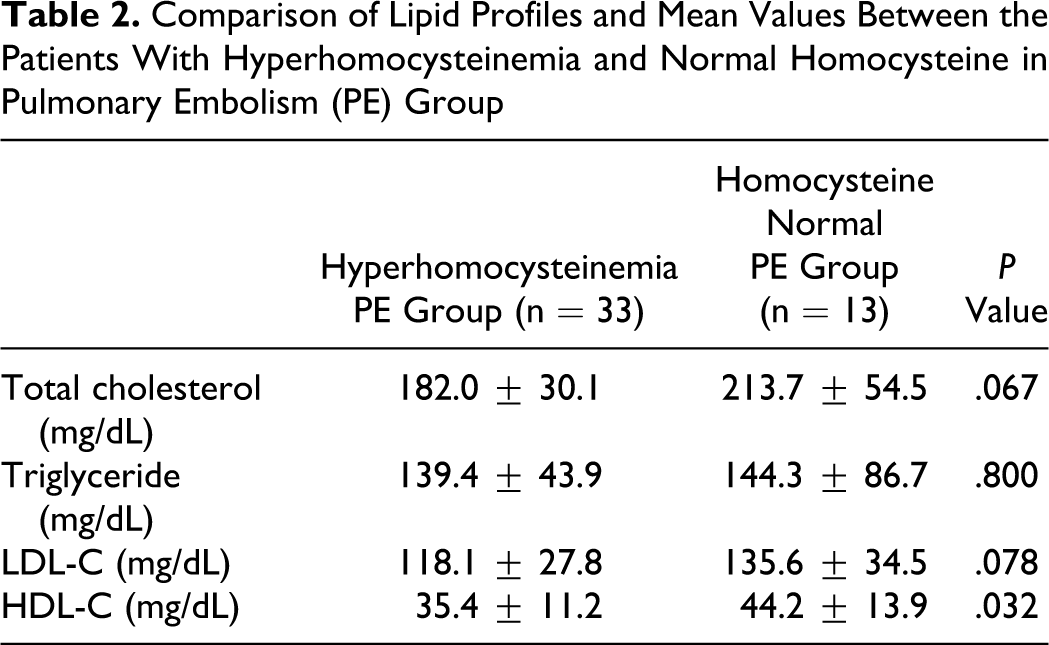
Comparison of lipid profiles and mean values between the patients with hyperhomocysteinemia and normal homocysteine in the PE group are shown in Table 2 . There was no statistical significance between the 2 groups in terms of total cholesterol (P = .067), triglyceride (P = .800), and LDL-C (P = .078). Meanwhile, HDL-C levels were lower in high homocysteine level PE group compared to normal homocysteine level PE group (P = .032; Table 2). Homocysteine was significantly correlated with HDL-C (r = −0.27, P = .002) but not with other lipid parameters.
Comparison of Lipid Profiles and Mean Values Between the Patients With Hyperhomocysteinemia and Normal Homocysteine in Pulmonary Embolism (PE) Group
Discussion
In the present study, we found that patients with PE had higher homocysteine levels and lower HDL-C levels. In the literature, several studies showed that the patients with lower HDL-C levels and higher homocysteine levels were susceptible to arterial thrombosis and cardiovascular diseases. Hyperhomocysteinemia is a known risk factor for PE. Additionally, our findings suggested that a low HDL-C level might be a new possible risk factor for PE.
Dyslipidemia and dyslipoproteinemia are well-known risk factors for arterial thrombosis. 11 Venous thrombosis is a different entity from arterial thrombosis according to its thrombus appearance, etiology, and therapeutic approaches. Venous thrombosis is thought to be a multifactorial disease. 14 The relationship between dyslipidemia/dyslipoproteinemia and venous thrombosis was recently shown by a clinical study. 12 Hyperhomocysteinemia, alone or with other thrombophilic risk factors, may have a role in vascular occlusive pathology underlying varied clinical presentations. 15
Dyslipidemia is based on an elevated serum total cholesterol level or a low HDL-C, while conventional definitions rely on elevated serum triglycerides or low HDL-C. 16 Hyperlipidemia increases platelet size and platelet expression of glycoprotein IIIa and endothelial dysfunction. 14 Kawasaki et al showed that hypercholesterolemia plays an important role in pathogenesis of DVT, but on the other hand, there was no relation in the other 2 studies between hypercholesterolemia and DVT.12,17,18 In the same line, Glyn et al found that high cholesterol levels were related with coronary heart disease, but not with VTE. 19 Ray et al showed that the patients who take statin were protected from the development of VTE. 20 In this study, we found no relationship between high total cholesterol level and PE. In our study, none of the patients were on statin therapy.
Previous studies investigated the role of hypertriglyceridemia on the development of VTE.12,17,18,21 Doggen et al found that elevated triglyceride increased 2-fold VTE risk in postmenopausal women, also McColl et al showed that triglyceride increased the risk of VTE in obese young women.12,21 In contrast, we found no association between triglyceride and PE.
High-density lipoprotein cholesterol-C may reduce the risk of atherosclerotic lesions by the reverse cholesterol transport, anti-inflammatory and antioxidant effects, and attenuation of endothelial dysfunctions. 3 In previous studies, it has been shown that serum HDL-C levels are significantly low in PE11,22,23 and elevated serum HDL-C levels might decrease the risk of PE in postmenapausal women. 12 A recent study, by Wang et al showed that pulmonary arterial trunk embolism is negatively correlated with the level of HDL-C. 23 In contrast, other previous studies found no association between HDL-C and PE.3,16,4 Chamberlain et al found low HDL-C does not appear to be an important VTE risk factor. In our study, we also found serum HDL-C levels significantly low in the PE group compared to the control group.
Homocysteinemia is a predisposing factor to vascular abnormality by several mechanisms. It stimulates proliferation of vascular smooth muscle cells in the laboratory studies. It promotes platelet aggregation. Homocysteine may enhance binding of lp(a) to fibrin. High concentrations of homocysteine activates factor V, reduces protein C activation, inactivates the cofactor activity of thrombomodulin, suppresses thrombomodulin and anticoagulant heparin sulfate expression, and blocks tissue plasminogen activator binding to human endothelial cells. It also activates Factor XII, induces endothelial barrier dysfunction and inhibits yon Willebrand Factor processing and secretion. 10 Langman et al found plasma homocysteine levels significantly high in the patients with VTE compared to the controls. 24 A prevalence study by Den Heijer et al showed that hyperhomocysteinemia might be a risk factor for DVT. 25 In a meta- analysis by Ageno et al, hyperhomocysteinemia was an independent risk factor for VTE. 26 Similarly, we also found serum homocysteine levels significantly high in patients with PE.
There are some limitations of the study that have to be mentioned. First, this is a retrospective study. Second, we did not follow-up patients and look for recurrence of PE in the study population.
In conclusion, we determined significant statistical homocystine elevation and decrease in HDL-C in patients with PE. Further studies are warranted to answer “Is low HDL-C level risk factor for PE? and Is high HDL-C protective for development of PE?”
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.