
Abstract
Objective:
To investigate the effect of benazepril on plasma homocysteine (Hcy) levels and to analyze the correlation between the methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism and changes in Hcy levels in response to benazepril.
Methods:
A total of 231 patients with mild to moderate essential hypertension were enrolled, and benazepril was orally administered at a dose of 10 mg/d for 2 weeks. Plasma Hcy levels were measured by high-performance liquid chromatography at baseline and after 2 weeks of treatment. Genotyping of the MTHFR C677T polymorphism was performed by TaqMan probe technique.
Results:
There was no significant change in Hcy level after benazepril treatment for 2 weeks (P = .97). However, stratified by baseline Hcy levels, the patients with baseline Hcy <10 μmol/L had a significant increase in plasma Hcy levels (P = .003). The results from the multivariable linear regression analysis demonstrated a significant correlation between baseline Hcy levels and the changes in Hcy levels found in both the unadjusted (P = .002) and the adjusted model (P = .004). Strikingly, we found no significant effect modification by the MTHFR C677T polymorphism on the Hcy changes after benazepril treatment. There were also no statistically significant interactions of gene and environment factors (ie, gene smoking and drinking) on the changes in Hcy levels after benazepril treatment.
Conclusion:
Benazepril may cause an increase in plasma Hcy levels among patients with hypertension with low baseline Hcy levels, while effect modification by MTHFR C677T genotypes on the changes in Hcy levels in response to benazepril was not significant among patients with essential hypertension.
Introduction
Over the past 50 years, cardiocerebrovascular diseases have become a global public health problem of high incidence, high morbidity, and high mortality, causing increasing social and economic burdens. There are around 3 million people who die of cardiocerebrovascular disease annually, which accounts for about 45% of the total number of deaths in China per year. The traditional risk factors for cardiocerebrovascular diseases are well investigated, and hypertension is thought to be the most important factor that substantially contributes to the development of cardiocerebrovascular diseases. Interestingly, in recent years, hyperhomocysteinemia (HHcy), a newly independent risk factor for artery atherosclerosis and cardiovascular disease, attracts more and more attention. 1
Generally, plasma Hcy level greater than 10 μmol/L is thought as the critical point of HHcy and hypertension, with HHcy is defined as “H-type hypertension.” 2 The data from a 6-city study in China 3 show that the mean fasting plasma Hcy level of the adult population with hypertension is 15 μmol/L, and the respective incidences of HHcy in the male and female populations are up to 91% and 63%, respectively.
There are many factors that influence Hcy levels. Recently, a growing number of studies focused on the influence of antihypertensive drugs on Hcy levels administered to prevent cardiocerebrovascular diseases. A large cross-sectional investigation (N = 13 946) was carried out in the rural Chinese population with hypertension, and the odds ratio of HHcy was found to be 1.14 (95% confidence interval [CI]: 1.06-1.23) for participants with versus without antihypertensive treatment. 4 Several studies have already shown that thiazide-type diuretics can significantly increase plasma Hcy levels, 5,6 and the β-receptor blocker, metoprolol, decreases plasma Hcy levels. 7,8 Fan et al found that enalapril may cause an increase in plasma Hcy levels among the patients with hypertension having low baseline Hcy levels. 9 Šebeková et al revealed that the antioxidative effect of angiotensin-converting enzyme inhibitor (ACEI) in patients remained unaffected by plasma Hcy levels. 10 Westphal et al found that plasma Hcy levels were increased after captopril treatment, but this finding was not statistically significant, which may be due to a smaller sample size. 5 However, a contrasting result was reported from a case–control study by Poduri et al when they found that plasma Hcy levels declined after ACEI treatment. 7 Therefore, the effects of ACEI treatment on Hcy levels remain uncertain, and more studies are needed to resolve these controversies.
Methylenetetrahydrofolate reductase (MTHFR) is a key enzyme in the metabolism of Hcy. The mutation of MTHFR C677T is thermolabile, which prevents the transformation of the Hcy to methionine and thus increases the plasma Hcy level. The functional MTHFR polymorphism has a significant impact on the occurrence of cardiocerebrovascular diseases. Wald et al conducted a meta-analysis on 72 previous epidemiological studies involving 16 849 cases of ischemic heart disease and found that patients with the TT genotype who were prone to HHcy were at 21% increased risk of ischemic events compared with patients carrying the wild-type CC genotype. 11 Jiang et al 12 found effect modification by MTHFR C677T genotypes on the changes in blood pressure (BP) in response to benazepril among patients with essential hypertension. They also found 13 that the MTHFR C677T variant contributed to simvastatin’s effects on lowering Hcy levels among Chinese patients with primary hyperlipidemia, which indicates that there may be an association between MTHFR C677T genotypes and plasma Hcy levels in response to ACEI.
Plasma Hcy level is also affected by several environmental factors such as diet (deficiency of folic acid and vitamin 6), obesity, gender, smoking, drinking, and lack of exercise. 4,14,15 We hypothesize that there might be interactions between Hcy metabolic-related genetic variants and gender, obesity, smoking, and/or alcohol drinking in their associations with Hcy changes in response to ACEI.
In the present study, we examined the effect of benazepril on plasma Hcy levels in a cohort of patients with mild and moderate essential hypertension. We further investigated the effect of genetic modification by MTHFR C677T genotypes on changes in Hcy levels after benazepril treatment and the interactions between Hcy metabolic-related genetic variants and gender, obesity, smoking, and/or alcohol drinking insofar as manifested in their associations with the changes in Hcy levels.
Patients and Methods
Study Population
A total of 231 patients with mild to moderate hypertension were enrolled from the Huoqiu and Yuexi communities in Anhui Province, China, from July 2000 to January 2001. Participants who met the following criteria were recruited as patients with hypertension: (1) systolic blood pressure (SBP) was between 140 and 200 mm Hg or diastolic blood pressure (DBP) was between 90 and 120 mm Hg, (2) without any antihypertensive therapy 2 weeks prior to this study, (3) aged from 27 to 65 years, and (4) residence in specified communities for at least 2 years. To avoid any potentially severe adverse effects, patients with secondary hypertension, pregnancy, hypercalcemia, chronic cardiovascular disease, chronic cerebrovascular disease, chronic liver disease, renal diseases, or body mass index (BMI) greater than 33 kg/m2 were excluded. Patients who received any antihypertensive therapy within 2 weeks were also excluded. The study was approved by the ethics committee of Anhui Medical University, Hefei, China. The purpose and procedures of the study were carefully explained to all participants, and written informed consent was obtained.
Benazepril Treatment
After a washout period of 7 to 10 days, all patients were treated orally with benazepril (Giba-Geigy, Beijing, China) at a daily fixed dosage of 10 mg for 2 consecutive weeks. Patients were required to take their benazepril between 8:00 and 10:00
Blood Pressure Measurement
The patients were invited to our clinic center from 8:00 to 10:00
Plasma Hcy Examination
Venous blood samples were drawn between 8.00 and 10.00
Genotyping of MTHFR C677T
The central laboratory was responsible for the genotyping of MTHFR C677T (rs1801133) by TaqMan technique. The polymerase chain reaction (PCR) pairs of primers were GCACTTGAAGGAGAAGGTGTCT for the forward and TGTGTCAGCCTCAAAGAAAAGCT for the reverse. The probe sequences were ATGAAATCGGCTCCCGC for VIC and ATGAAATCGACTCCCGC for FAM. The assay was performed under universal conditions, with each reaction containing 4 ng dried DNA, 0.08 μL 40× assay mix, and 2.0 μL TaqMan universal PCR master mix made to a final volume of 4 μL with 1.92 μL sterile water. The PCR cycle conditions were as follows: initial denaturation at 95°C for 10 minutes, followed by 50 cycles of 92°C for 15 seconds and 60°C for 1 minute. All sample sets genotyped for the single-nucleotide polymorphism in our present study had overall call rates of ≥95%, after excluding samples that consistently failed. We selected 10% of total samples for replication, and concordance of 100% was repeated for all samples’ quality control.
Statistical Analysis
Epidata 3.1 Chinese version was used for database design, data entry, and data check. Mean ± standard deviation were calculated for continuous variables. The t-test was used to compare mean differences for continuous variables. The chi-square test was used for categorical variables. A multivariable linear regression model was used to evaluate the modification effect of the baseline Hcy levels and MTHFR C677T polymorphism on the changes in Hcy levels after benazepril treatment before and after adjusting for possible confounders, including age, gender, BMI, smoking, and drinking. Differences were considered to be significant at P < .05 for the 2-sided test. All statistical analyses were carried out using the R version 3.0.3 package.
Results
Baseline Characteristics of the Participants
A total of 231 patients with mild and moderate hypertension were used in the final data analysis. As shown in Table 1, age, BMI, height, weight, total cholesterol (TC), triglycerides (TGs), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), creatinine, baseline BPs, baseline Hcy, smoking and drinking status, community of residence, and MTHFR genotype distributions were compared between male and female patients, respectively. Only age, BMI, TC, TG, LDL-C, and baseline SBP were not significantly different between the 2 genders (ie, P > .05). The HDL-C was significantly higher in female patients than in male patients (P = .001), and there were significantly higher proportions of men than women who were smokers (P < .001) and drinkers (P < .001). Males had higher baseline Hcy levels (14.82 ± 11.51 μmol/L) than females (10.76 ± 4.87 μmol/L; P < .001). The percentages of HHcy (Hcy ≥ 10 µmol/L) were 71.15% and 48.82% in male and female patients, respectively, which differed significantly (P = .001). The distribution of MTHFR C677T genotypes was not significantly different between males and females (P = .54).
Baseline Characteristics of the Patients.a
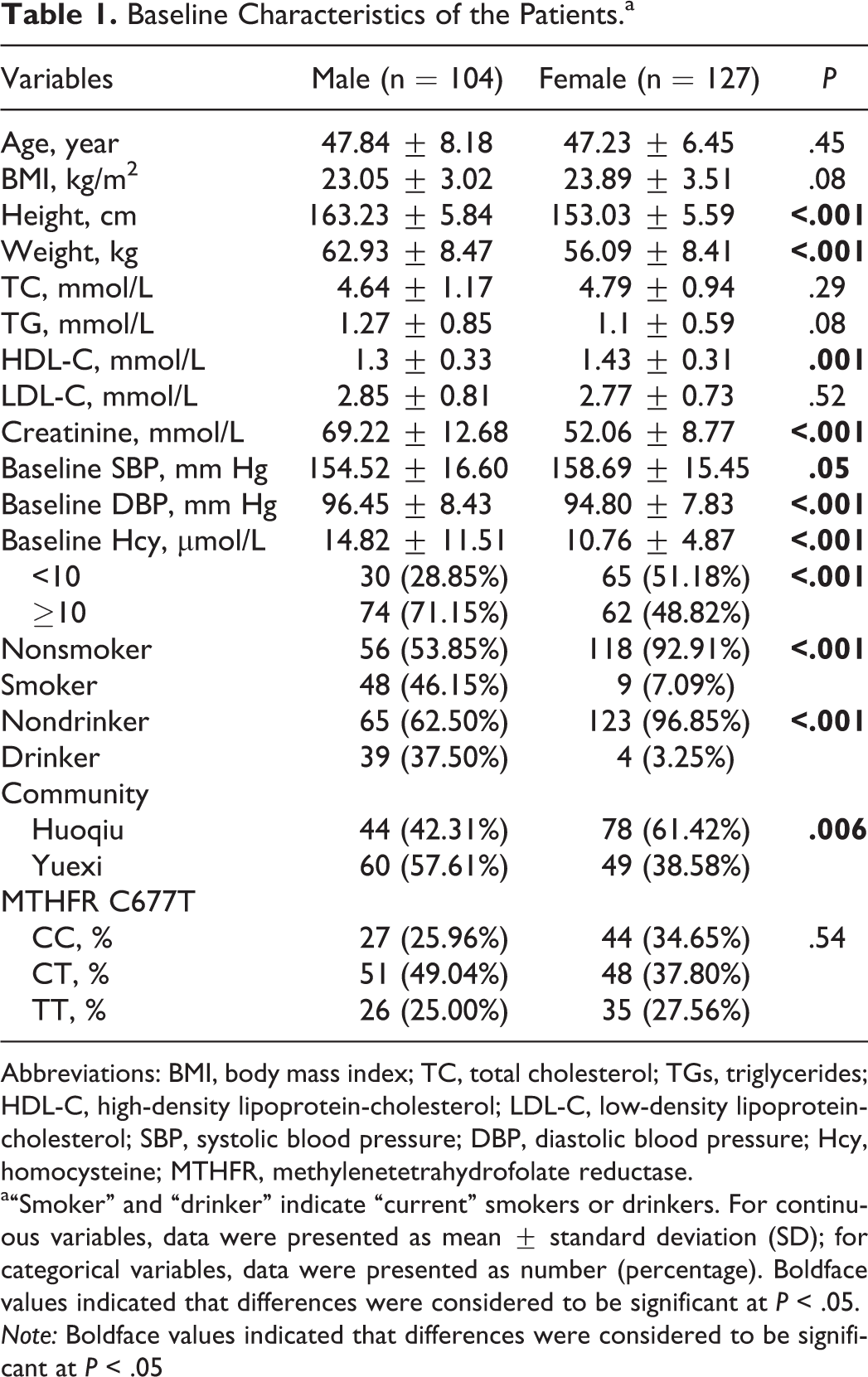
Abbreviations: BMI, body mass index; TC, total cholesterol; TGs, triglycerides; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; Hcy, homocysteine; MTHFR, methylenetetrahydrofolate reductase.
a“Smoker” and “drinker” indicate “current” smokers or drinkers. For continuous variables, data were presented as mean ± standard deviation (SD); for categorical variables, data were presented as number (percentage). Boldface values indicated that differences were considered to be significant at P < .05. Note: Boldface values indicated that differences were considered to be significant at P < .05
Effect of Benazepril Treatment on Hcy Levels
Among all patients, there were no significant changes observed in the Hcy levels after benazepril treatment (P = .97). We then tested the hypothesis that the effects of benazepril on Hcy levels were modified by baseline Hcy levels. Stratified by baseline Hcy levels, the patients with baseline Hcy <10 μmol/L indeed had a significant increase in plasma Hcy levels (P = .003) after treatment. In contrast, those with baseline Hcy ≥10 μmol/L had no remarkable changes in plasma Hcy levels (P = .61; Table 2). Further multivariable linear regression evaluated the effect of baseline Hcy levels on the changes in Hcy levels after benazepril treatment, and the results found in Table 3 demonstrated that baseline Hcy levels were significantly related to the changes in Hcy levels in both the unadjusted (P = .002) and the adjusted model (P = .004).
Effect of Benazepril Treatment on Hcy Levels.a

Abbreviation: Hcy, homocysteine.
aFor continuous variables, data were presented as mean ± standard deviation (SD). Boldface values indicated that differences were considered to be significant at P < .05.
Multivariable Linear Regression of Effect Modification by Baseline Hcy Level of the Changes of Hcy Levels After Benazepril Treatment.a
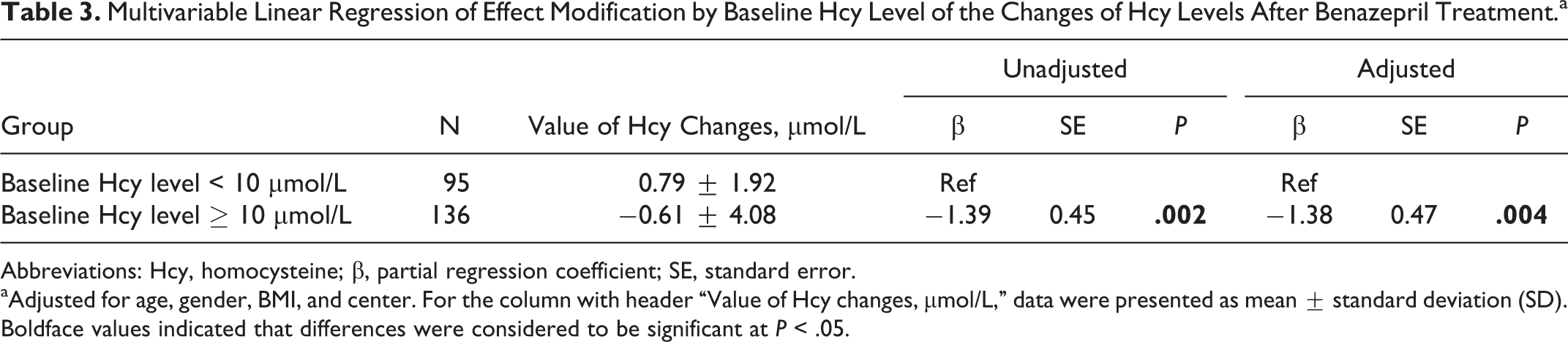
Abbreviations: Hcy, homocysteine; β, partial regression coefficient; SE, standard error.
aAdjusted for age, gender, BMI, and center. For the column with header “Value of Hcy changes, µmol/L,” data were presented as mean ± standard deviation (SD). Boldface values indicated that differences were considered to be significant at P < .05.
Modification Effect of MTHFR C677T Polymorphism on the Changes in Hcy Levels After Benazepril Treatment
The MTHFR C677T polymorphism has been found to modulate drug effects, 15 and we investigated whether it would modify the effects of benazepril. The baseline Hcy levels for CC, CT, and TT genotypes were 10.80 ± 3.52, 10.08 ± 3.11, and 18.74 ± 14.49 μmol/L, respectively. It indicated that patients with the TT genotype had significantly higher Hcy levels than others (P < .001; Table 4). The pattern was similar in both males and females. We then assessed effect modification by MTHFR C677T genotypes in the changes of Hcy levels in response to benazepril. The data in Table 5 showed that the changes in Hcy levels after 2 weeks of treatment among the MTHFR genotypes were −0.14 ± 2.1, 0.23 ± 2.27, and −0.32 ± 5.56, respectively. These results supported the conclusion that there was no effect modification by the MTHFR C677T polymorphism of changes in Hcy levels after treatment in either unadjusted or adjusted models.
Baseline Hcy Levels of Patients With the 3 Different MTHFR C677T Genotypes.a
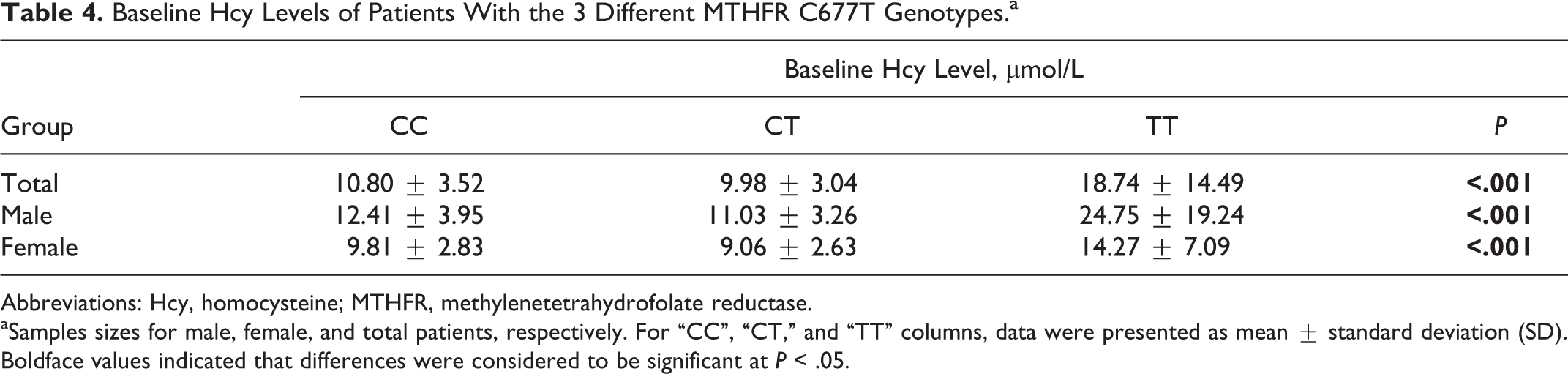
Abbreviations: Hcy, homocysteine; MTHFR, methylenetetrahydrofolate reductase.
aSamples sizes for male, female, and total patients, respectively. For “CC”, “CT,” and “TT” columns, data were presented as mean ± standard deviation (SD). Boldface values indicated that differences were considered to be significant at P < .05.
Effect Modification by MTHFR C677T Polymorphism on the Changes in Hcy Levels After Benazepril Treatment.a
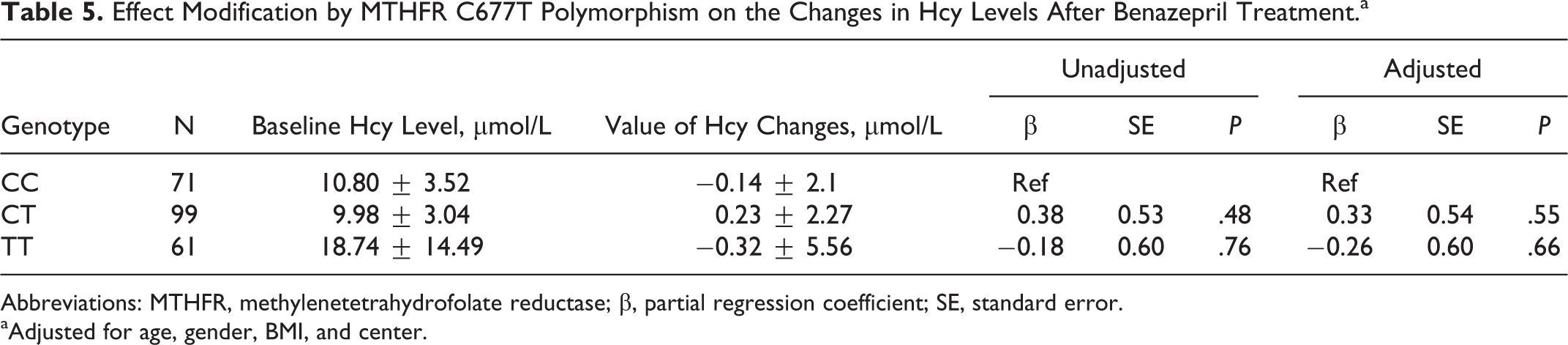
Abbreviations: MTHFR, methylenetetrahydrofolate reductase; β, partial regression coefficient; SE, standard error.
aAdjusted for age, gender, BMI, and center.
Effect Modification by Genotype in Subgroups Determined by Environmental Exposure
We have found that the baseline Hcy levels played a substantial role in the effects of benazepril treatment, while the MTHFR C677T polymorphism did not modify these effects. It remains elusive whether environmental factors would define population subgroups among which the MTHFR C677T polymorphism would modify the effects of benazepril treatment (gene–environment treatment interaction). We stratified by BMI, gender, smoking, and drinking to evaluate genetic modification by MTHFR C677T on the changes in Hcy levels after treatment. We found no evidence of effect modification by MTHFR C677T of changes in Hcy after treatment within any stratum of BMI, gender, smoking, or drinking (data not shown).
Discussion
Hypertension is a leading risk factor for cardiovascular diseases. More recently, many studies have shown that elevated Hcy is positively associated with hypertension risk. 16 –18 Cross-sectional data from the Third National Health and Nutrition Examination Survey showed that men and women in the highest quintile of Hcy had 2- and 3-fold increased risks of hypertension, respectively, compared with those in the lowest quintile. 16 This indicated that the increased risk of cardiovascular diseases associated with HHcy might be mediated in part by the positive association of Hcy with hypertension. The possible mechanisms by which homocysteine could facilitate the development of hypertension include the impairment of vascular endothelial and smooth muscle cell function. 19,20 Therefore, the occurrence of endothelial dysfunction could contribute to alterations in the endothelium-dependent vasomotor regulation. Elevated Hcy diminishes the vasodilation by nitric oxide, increases oxidative stress, stimulates the proliferation of vascular smooth muscle cells, and alters the elastic properties of the vascular wall.
Folic acid is an excellent agent to effectively reduce the plasma Hcy. If the positive association of Hcy with an increased hypertension risk is causal, then it would be expected that the Hcy-lowering therapy based on folic acid supplementation could result in therapeutic efficacy in decreasing BP. A meta-analysis 21 including 12 clinical trials used patients with hypertension who were supplemented with high-dose folic acid identified that the pooled estimate of the effect of folic acid supplementation on SBP was −2.03 mm Hg (95% CI: −3.63 to −0.43; P = .04). A 20-year follow-up observational study 22 further confirmed that participants in the highest quintile of total folate intake had a significantly lower incidence of hypertension (hazard ratio: 0.48; 95% CI: 0.38-0.62; P trend <.01) than did those in the lowest quintile. It suggested that high-dose folate is longitudinally associated with a lower incidence of hypertension. Thus, the potential causal role of Hcy in the pathogenesis of hypertension is not only heightened by the demonstration that Hcy-lowering vitamin treatment is associated with a reduction in SBP and DBP 21,22 but also proven by the clinical trials that antihypertensive drug treatment can significantly influence the levels of Hcy. 4 –10
Benazepril is a kind of ACEI drug that is recommended as a first-line medicine for hypertension treatment. The main role of ACEIs is acting on the renin–angiotensin–aldosterone system, where they can inhibit the generation of angiotensin II, reduce the degradation of bradykinin, and extend the vasodilatation of bradykinin, which finally causes reduction in vascular dilatation and pressure. Fan et al 9 investigated a total of 130 Chinese patients with mild to moderate essential hypertension who were administered enalapril at a dose of 10 mg/d for 8 weeks. They did not find any significant influence on plasma Hcy levels by enalapril. However, after stratification by baseline Hcy levels, a significant increase in plasma Hcy levels (P = .02) among those with Hcy <10 μmol/L was observed. Their findings proved that enalapril may cause an increase in plasma Hcy levels among the patients with hypertension having low baseline Hcy levels. Similar to their findings, our present study results showed that the patients with baseline Hcy <10 μmol/L had a significant increase in plasma Hcy levels (P = .003) in patients after treatment with benazepril. Further multivariable linear regression confirmed that the baseline Hcy levels were significantly associated with the changes in Hcy levels in both the unadjusted (P = .002) and the adjusted models (P = .004). A large cross-sectional investigation (N = 13 946) in the rural Chinese population with hypertension further supported that the odds ratio of HHcy was 1.14 (95% CI: 1.06-1.23) for participants with versus without antihypertensive treatment. 4 In the data analysis, we used the 10 μmol/L Hcy level as a standard for grouping the basic value of Hcy. This was based on the American Heart Association/American Stroke Association’s guideline on stroke published in 2006, which provided the early warning reference value for stroke prevention in patients with ischemic stroke and transient ischemic symptoms. 23
However, a contradicting finding was observed in another study. Poduri et al 7 conducted a case–control study of 273 patients with essential hypertension and 103 normotensive controls. Their results demonstrated that ACEIs and β-blockers significantly decreased and hydrochlorothiazides significantly increased the plasma Hcy levels in patients with hypertension. Thus, their results suggested that ACEIs may provide additional beneficial therapeutic effects to essential patients with hypertension by decreasing Hcy levels. Westphal et al designed a preliminary, randomized, prospective treatment study in 40 patients with hypertension and investigated the influences of hydrochorothiazide (HCT) and captopril on Hcy levels and the major determinants (vitamins B6 and B12 and folic acid) of Hcy concentrations. 5 They found that there were no significant changes in Hcy and other determinants after captopril treatment. Maybe, the inconsistent results could be explained by the distinct baseline Hcy levels in each study. Our previous study regarding simvastatin treatment and Hcy levels found that simvastatin will have different effects as the initial serum Hcy concentration varies. 13 Furthermore, in the study of Poduri et al, 7 the baseline Hcy level was relatively higher 19.12 ± 6.94 μmol/L, and their study showed significant decrease in Hcy levels. Our findings provide important insights into the mechanisms of benazepril treatment on serum Hcy.
Additional recent studies have shown that diuretics used for the treatment of hypertension lead to an increase in Hcy levels in patients with hypertension. 5,6 Such studies proposed that HCT treatment increases Hcy levels, probably via an alteration in renal function or via an alternative mechanism that a decrease in the concentration of folate in red blood cells results from diuretics therapy. The plausible mechanism might give an explanation for our findings that benazepril did increase Hcy levels in patients with low Hcy levels. Elevation in Hcy after benazepril use may be of clinical importance. However, 1 limitation of our present study is that we didn’t measure the changes in renal function (ie, creatinine) and serum folate levels before and after benazepril treatment for 2 weeks. In addition, another potential limitation is that our study is not designed as a placebo-controlled randomized trial. Therefore, it is relatively difficult to draw the conclusion that the changes in Hcy level after the administration of benazepril were attributable solely to the drug itself.
The MTHFR is a key enzyme of Hcy remethylation metabolic pathways. 677C/T in the MTHFR gene is a common functional mutation. The mutation of MTHFR is thermolabile, which hinders the transformation of the Hcy to methionine and increases the plasma Hcy level. 24 A number of studies have proven that the T allele of the MTHFR C677T polymorphism increases the risk of atherosclerosis, coronary heart disease, stroke, and other cardiocerebrovascular diseases 25 –29 Some studies suggested that MTHFR C677T can interact with antihypertensive therapy to influence the change in Hcy levels and further modify the risk of cardiovascular outcomes 30 Jiang et al 13 provided a valuable clue that the MTHFR C677T genetic variant contributes to the lipid-lowering drug simvastatin’s effects on the Hcy levels among Chinese patients with primary hyperlipidemia. When Qin et al 31 randomly assigned 480 patients with mild or moderate essential hypertension into 3 treatment groups, they demonstrated that the MTHFR C677T polymorphism can not only affect Hcy concentration at baseline and postfolic acid treatment but also modify therapeutic responses to various dosages of folic acid supplementation. However, Fan et al 9 and Poduri et al 7 identified that there was no significant association between the MTHFR C677T genotypes and changes in Hcy levels in response to antihypertensive drug among patients with essential hypertension. Although our current study also demonstrated no effect modification of the MTHFR C677T genotypes on the changes in Hcy levels in response to benazepril, given that different classes of ACEI drugs were studied in the above referred studies of enalapril with or without folic acid supplementation by Qin et al, 31 of enalapril by Fan et al, 9 and of ramipril as ACEI drug by Poduri et al, 7 it appears that the MTHFR C677T genotype could modify the change in Hcy level caused by ACEI and folic acid but not certainly for ACEI drug alone. It clearly indicated that the impacts of the MTHFR C677T locus on change in Hcy level are dependent on folic acid, rather than a particular ACEI drug. Consistent results obtained by various empirical studies exhibited that the MTHFR C677T genotype could not modify the change in Hcy level caused by the various antihypertensive agents applied.
It is well known that complex traits such as Hcy change are generally caused by genetic factors and their interaction with the environment. Therefore, we further analyzed the gene–environment interactions in the changes in Hcy levels after benazepril treatment.
Obese patients have impaired liver function that affects the activity of the enzyme in the metabolic pathway of Hcy, which then affects the changes in Hcy level. One study found that BMI was positively correlated with plasma Hcy level. 32 However, there is no statistically significant interaction between BMI and MTHFR 677TT in association with changes in Hcy levels.
Gender is another important factor affecting Hcy level. Some studies showed that males had higher baseline Hcy levels than females. 4 This result might be due to the estrogen involved in the process of Hcy metabolism, but the specific mechanisms remain elusive. In this study, we did not find statistically significant interaction between gender and MTHFR 677TT in association with changes in plasma Hcy levels.
Epidemiological studies 13,14 showed that both smoking and drinking were risk factors for HHcy and were associated with the elevation in Hcy levels. It might derive from the fact that smoking and drinking interfere with metabolism of vitamin B6, vitamin B12, and folic acid, which will lead to plasma Hcy accumulation. However, our study did not find a statistically significant interaction between smoking or drinking and MTHFR 677TT in association with changes in plasma Hcy levels.
One limitation of this study was a small sample size that resulted in limited power for detecting significant associations. Another limitation for the present study was that we did not genotype the MTHFR A1298C locus. However, unlike the C677T locus, a large number of related publications showed that A1298C is controversially and inconsistently associated with plasma Hcy levels in different populations. 33 Furthermore, as described in our previous publication, 34 MTHFR C677T and A1298C are in high linkage disequilibrium (LD); that is, the 677T allele is in LD with 1298A, while the 677C allele is in LD with 1298C. Therefore, in some references, 35 the authors could observe that MTHFR C677T showed an opposite trend for both parameters, Hcy level and serum folate level, compared with A1298C. Based on the above-mentioned evidence, we felt that C677T is a representative marker, and it was not necessary for us to detect the other A1298C locus in our population.
In summary, our results suggested that benazepril can cause an increase in plasma Hcy levels among patients with hypertension having low baseline Hcy levels. There was no significant effect modification by MTHFR C677T genotypes in the changes in Hcy levels in response to benazepril, and this remained true within population subgroups defined by various environmental exposures (gene–environment treatment interactions). In consideration of the correlation between Hcy and cardiocerebrovascular disease, a proposed suggestion could be to supplement folic acid for patients with a mild elevation in Hcy when benazepril is used for treatment in clinical practice.
Footnotes
Acknowledgments
We gratefully acknowledge the assistance and cooperation of the faculty and staff of the Anhui Medical University and thank all of the participants in our study.
Authors’ Note
This study was conducted in accordance with the current regulations of the People’s Republic of China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (Grant Nos. 81373484, 81141116 and 30700454) and the Academic Leader and Reserve Candidate of Anhui Province (No. 05010543).