
Abstract
The Caprini risk assessment model (RAM) has been validated in over 250 000 patients in more than 100 clinical trials worldwide. Ultimately, appropriate treatment options are dependent on precise completion of the Caprini RAM. As the numerical score increases, the clinical venous thromboembolism rate rises exponentially in every patient group where it has been properly tested. The 2013 Caprini RAM was completed by specially trained medical students via review of the presurgical assessment history, medical clearances, and medical consults. The Caprini RAM was completed for every participant both preoperatively and predischarge to ensure that any changes in the patient’s postoperative course were captured by the tool. This process led to the development of completion guidelines to ensure consistency and accuracy of scoring. The 2013 Caprini scoring system provides a consistent, thorough, and efficacious method for risk stratification and selection of prophylaxis for the prevention of venous thrombosis.
Keywords
Background
Pulmonary embolism (PE) and deep vein thrombosis (DVT), collectively known as venous thromboembolism (VTE), represent a major public health dilemma that affects 350 000 to 600 000 Americans annually. 1 Venous thromboembolism remains the most preventable cause of death in hospitalized patients and is known to cause significant morbidity with associated health-care expenditure. 2 After a primary thromboembolic episode, VTE recurs in approximately 25% of patients over the subsequent 10 years. Complications associated with VTE include postthrombotic syndrome after DVT (20%-50% incidence) and chronic thromboembolic pulmonary hypertension after PE (0.1%-3.8% incidence). 3 These conditions negatively impact quality of life and individual productivity while adding burden to the patient, their support system, and the health-care system at large.
There has been a marked increase in federal and national efforts over the last decade to increase both awareness and treatment of this avoidable outcome. In 2008, the Surgeon General and the Director of the National Heart, Lung and Blood Institute announced a “Call to Action to Prevent Deep Vein Thrombosis and Pulmonary Embolism.” The Call to Action emphasized public awareness about risk factors, triggering events, and symptoms of venous thrombosis and PE and encouraged the development of evidence-based practices for screening, prevention, diagnosis, and treatment of venous thrombosis and PE. 4 From 2006 through 2008 in recognition of the high attributable risk of DVT and PE due to hospitalization, the National Quality Forum, the Joint Commission, and the Centers for Medicare and Medicaid Services all instituted policies and measures to reduce VTE and promote appropriate prophylaxis to at-risk patients in the hospital setting. 5 In 2008, the eighth edition of the American College of Chest Physicians (AT8) guidelines for the prevention of VTE endorsed the need for an “active, formal strategy” to prevent hospital-induced VTE. The authors felt that available risk assessment models (RAMs) were minimally validated and impractical to use. 6 They proposed that thrombosis prophylaxis should be provided for groups of patients where clinical trial data were available. It has been subsequently shown that since many patients in clinical practice did not fit the criteria for clinical trials, a specific analysis of each individual’s risk factors was a better approach. The availability of the electronic medical record has facilitated collection of these data and assisted in the implementation of RAMs. As a result, over the past 5 years, individual thrombosis risk assessment has become accepted practice in most surgical specialties.
There are multiple quantitative VTE RAMs available for use in clinical practice. The Padua Prediction Score and IMPROVE RAMs were designed to address VTE risk in medical patients. 7,8 The ninth edition of the American College of Chest Physicians Antithrombotic Therapy and Prevention of Thrombosis guideline (AT9) has recognized only 2 risk assessment tools in the nonorthopaedic surgical population, the Rogers Score, and the Caprini Score. 9 The Rogers Score has been validated in general, vascular, and thoracic surgery in a single study. The score is based on variables that were found to be independent predictors of VTE risk such as surgical procedure, female sex, and a variety of other individual patient characteristics. 10 Unlike the Caprini RAM, the Rogers score does not take into account certain VTE risk factors including any personal or family history of VTE and thrombophilia. Several other issues have been identified with using this model. Firstly, the categorizations by which variables are assigned point values are not easy to follow and have been noted as “cumbersome” to use. 9,10 Secondly, the study that was used to validate this RAM did not clearly state which patients received prophylactic measures for VTE, and what type they received (ie, mechanical, pharmacological). 9
Caprini Risk Assessment Tool for VTE
A group of physicians, nurses, and scientists led by Dr Caprini developed a risk assessment scoring system first published in 1991. 11 Individual risk factors were assigned one or more points according to their relative risk of resulting in a thrombotic event. Factors such as surgery or cancer received 2 points, whereas varicose veins or oral contraception were assigned one point. The initial assignment of points was based on the relative risk of thrombosis for each risk factor using current literature at that time. For example, cancer or past history of thrombosis were stronger risk factors than swollen legs. The total score for each patient was compared to the incidence of clinically evident VTE events at 30 days to validate the model. An exponential increase in thrombotic events with increasing score has been observed for every group properly tested. This allowed for categorizing patients into low-, moderate-, and high-risk groups based on the thrombosis event rate for each group. Using this stratification data, the type, duration, and strength of prophylaxis could be tailored to the level of risk. The clinical VTE event rate for each group could be compared to the patients’ risk of bleeding, resulting in prophylaxis tailored to provide optimal thrombosis protection.
Since its introduction in 1991, the Caprini RAM has been validated in over 250 000 patients in more than 100 clinical trials worldwide. 12 –22 One should note that the cutoff score between risk groups varies depending on the surgical population that is tested. AT9 defines the high-risk group as a score of 5 or greater for general surgery patients. 9 This cutoff point, however, is not appropriate for all surgical specialties. Since then, a score of 12 has been shown to be the very high-risk cutoff for those with hip fractures. 12 A companion manuscript submitted for publication in this journal involving total joint arthroplasty included 1078 patients to establish the very high-risk cutoff in this population. Krauss et al found that total joint arthroplasty patients with a score of 10 or greater were at high risk of VTE, and the authors presented data that this very high-risk group would benefit from traditional anticoagulants. 23 Patients with a lower score could safely receive aspirin according to their findings. A large, prospective, multicenter trial to test these concepts is currently in development.
Drugs administered to prevent VTE carry their own risks, specifically minor to major bleeding events. Thus, individualization of prophylaxis treatment based on calculated risk factors will prevent unnecessary prophylaxis for patients deemed low risk while providing prophylaxis for patients who are high risk. Ultimately, the appropriate treatment options are dependent on precise completion of the Caprini RAM. An inaccurate medical history or incorrect interpretation of criteria contained in the RAM could result in an erroneous Caprini score, thereby leading to an incorrect treatment assignment for the patient.
Recently, Pannucci and colleagues performed a meta-analysis of selected publications using Caprini scores to investigate benefits and harms of chemoprophylaxis among surgical patients individually risk stratified for VTE. They evaluated 13 studies; 11 (n = 14 776) contained data for VTE events, and 8 (n = 7590) contained data for clinically relevant bleeding with and without chemoprophylaxis. The most important finding was a 14-fold increase in VTE risk (from 0.7% to 10.7%) among surgical patients who did not receive chemoprophylaxis, and patients with higher Caprini scores were significantly more likely to have a thrombotic event. The benefit of perioperative VTE chemoprophylaxis was only found among surgical patients with Caprini scores equal to or greater than 7. 24 One must remember that this study selected the purest 13 of the nearly 100 clinical trials, and these results may not apply to all patient groups. This meta-analysis, however, demonstrates the value of the Caprini score in classifying patient risk to selectively use anticoagulants without exposing entire populations to anticoagulants, as was popular in the past.
The 2013 version is the most recent iteration of the Caprini RAM. 25 This version differs from preceding versions in that it includes additional risk factors not tested in validation studies but shown in the literature to be associated with thrombosis. These identified risk factors include BMI above 40, 26,27 smoking, 28,29 diabetes requiring insulin, 30,31 chemotherapy, 32,33 blood transfusions, 34,35 and length of surgery over 2 hours. 36,37
During our validation study of the 2013 Caprini RAM in arthroplasty patients, scoring was completed by specially trained medical students via review of the presurgical assessment history, medical clearances, and medical consults. Any questions or concerns were escalated to Dr Caprini. The Caprini RAM was completed for every participant both preoperatively and predischarge to ensure that any changes in the patient’s postoperative course were captured by the tool (Figure 1).

Caprini Risk Assessment Model (version 2013).
Completion Guidelines
The patient or the patient’s health-care advocate should complete the risk assessment tool. 38 In 2017, Fuentes et al tested multiple versions of a patient-friendly Caprini risk score worksheet until they created a tool that, when completed first by the patient, and then by a physician trained to interpret the Caprini RAM, yielded a high correlation of agreement. The average time to complete the tool was 5 minutes for the patient and then 6 minutes for the physician to finalize the score. 38 Having the patient complete the validated patient-friendly risk assessment in advance of the day of surgery in the presence of family members is vital, especially to provide details concerning family history of thrombosis and obstetrical complications (where applicable). Personal experience has taught us that on many occasions, questions regarding family history of thrombosis in first-, second-, and third-degree relatives are not asked or are addressed in a superfluous manner. 39 Patients who have this history have an increased level of risk, equivalent to those who have a personal thrombophilic defect. 40
Pannucci and Fleming have stressed the importance of face-to-face patient interviews rather than relying on record review. 41 One of the most common errors is failure to ask all of the pertinent questions. Retrospective database reviews are flawed since it is not known if all of the questions were presented to the patient or if their responses reflected an accurate interpretation of the question. This is especially true of obstetrical complications which may reflect possible antiphospholipid syndrome being carried by a preoperative patient later in life. These antibodies are a powerful stimulus for VTE. Family history is the most frequent issue that is overlooked. To reemphasize, a history of past VTE or family VTE history is one of the most prevailing risk factors responsible for postoperative thrombosis, including untimely death. 38
The immediate preoperative period on the day of surgery is strongly discouraged for completion of the Caprini RAM. It is an anxious time for the patient and family and a comprehensive, accurate assessment may not be captured. We have found that the presurgical testing visit is an optimal opportunity for the patient and family to fill out the patient-friendly form. The entire document is then reviewed by the health-care provider, preferably the person responsible for the preoperative history and physical. Knowledge regarding a detailed history and physical is necessary to precisely complete the tool for optimal patient outcomes with respect to thrombosis.
The Caprini RAM is a dynamic tool, requiring ongoing evaluation of the patient during their hospital course and the postoperative recovery period. Changes in clinical status could result in a change in the score, thereby resulting in a new score and potentially a revised treatment option. For example, a postoperative infection necessitating a central line for antibiotics would increase a patient’s score, and subsequently, the incidence of VTE. A patient sent home after a short hospitalization may be unexpectedly immobile due to postoperative pain or weakness and might develop leg swelling due to inactivity. This may increase their chance of suffering a thrombotic event in the outpatient setting.
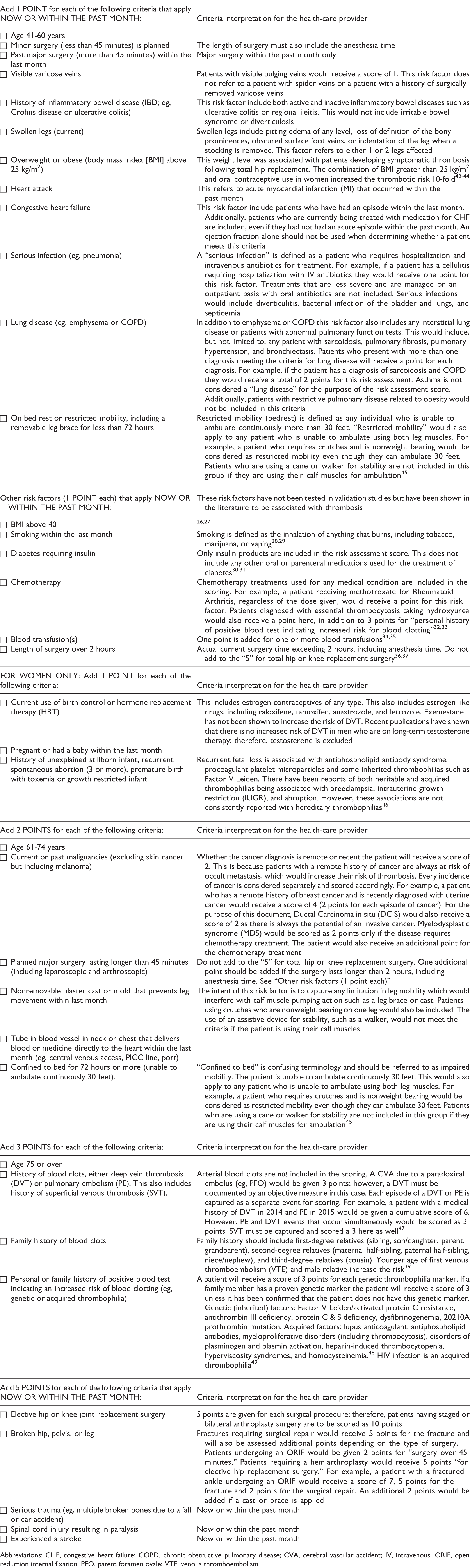
Accurate interpretation of the 2013 version of the Caprini RAM is discussed below. The Caprini RAM requires detailed patient information for successful risk assessment. Thus, a tool with patient-friendly text has been created for the 2013 version of the Caprini RAM and is now completed by all of our patients in presurgical testing, which occurs up to 21 days prior to surgery (Figure 2).

Patient-friendly tool (Caprini RAM version 2013) - side 1. Completed by the patient -side 2. Completed by the Healthcare Provider.
Conclusion
The Caprini RAM is a dynamic tool, requiring ongoing evaluation of the patient during their hospital course and the postoperative recovery period. Changes in clinical status could result in a change in the score, thereby resulting in a new score and potentially a revised treatment option. The 2013 Caprini scoring system provides a consistent, accurate, and efficacious method for risk stratification and selection of prophylaxis.
Abbreviations: CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular accident; IV, intravenous; ORIF, open reduction internal fixation; PFO, patent foramen ovale; VTE, venous thromboembolism.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.