
Abstract
Background:
Venous thromboembolic disease (VTE) is higher among patients with cancer. For those undergoing abdominal or pelvic surgery for cancer, it is suggested to extend thromboprophylaxis during 4 weeks with low-molecular-weight heparin over limited-duration of 7 days. There is no published local data from our country about compliance with recommended guidelines of extended prophylaxis (EP) in patients with cancer undergoing surgical procedures. Our aim was to evaluate the adherence rate to extended pharmacological thromboprophylaxis after abdominal–pelvic surgery for cancer, before and after an educational intervention program (EIP) geared toward surgeons.
Methods:
Prospective cross-sectional study before and after an EIP aimed for surgeons. All consecutive patients older than 65 years who underwent surgery for abdominal–pelvic neoplasm, at the Hospital Italiano de Buenos Aires, Argentina, between September 2013 and May 2014, were evaluated for inclusion.
Results:
A total of 120 patients were included, 60 before and 60 after the EIP aimed for surgeons. None of the initial 60 patients received EP, while 13 (21.6%) of 60 patients received prophylaxis for 28 days (all with colon or rectal cancer) after the intervention. There were no bleeding or death during 90 days of follow-up, and there were 7 of 120 VTE events, none in the group receiving extended thromboprophylaxis.
Conclusion:
The EIP for the surgical team significantly improved their adherence but only in the colon–rectal surgeries. The adherence to the recommended guidelines is still low. Reasons could be the subjective perception of elevated bleeding risk and the variable grade of recommendation in different guidelines.
Keywords
Background
Venous thromboembolic disease (VTE) is frequent and can lead to a fatal outcome. It is the third leading cause of mortality due to circulatory diseases. 1 –3 The incidence of postoperative fatal pulmonary embolism (PE) is at least 2 times higher among patients with cancer than in those without cancer undergoing similar surgical procedures. 4 –6 Among patients undergoing abdominal cancer surgery, VTE is the most common cause of death 30 days after surgery. 2,4,5
For high VTE risk patients undergoing abdominal or pelvic surgery for cancer, who are not at increased risk of bleeding, several guidelines (ACCP, NICE, ASCO) recommended to extend the pharmacologic prophylaxis for 4 weeks with low-molecular-weight heparin (LMWH) over limited-duration of 7 days the prophylaxis to the hospital stay. 6 –17 In addition, VTE risk increases sharply with advancing age, particularly after 65 years.
Although thromboprophylaxis after surgery for cancer has showed good adherence rates during hospitalization, the adherence rate of extended thromboprophylaxis (EP) in this group of patients after discharge is reported to be low, despite recommended guidelines. 4,8 We did not find any publication with regard to this in Argentina, but we believe that it is as low as those reported for other countries, according to international reports, which is less than 25% for this high-risk group of patients who received EP. 15
We carried out a prospective study to analyze the adherence rate of EP with enoxaparin for 28 days in patients of 65 years or older who underwent abdominal or pelvic surgery for cancer, before and after an educational intervention program (EIP). Secondary objectives were (a) to analyze the adherence rate in 3 different subgroups of cancer surgery: (1) colon and rectal cancer (CRC), (2) liver and pancreatic cancer (LPC), and (3) esophagus, gastric, and duodenum cancer (OGDC); (b) to analyze the rate of major bleeding and VTE complications during treatment; and (c) to detect barriers to appropriate adherence to thromboprophylaxis.
Methods
Design
Prospective cross-sectional study before and after 6 months of an interventional educational program aimed for surgeons.
Setting and Population
All consecutive patients who underwent surgery for an abdominal or pelvic neoplasm at the Hospital Italiano de Buenos Aires (HIBA) that belongs to the HIBA health maintenance organization (HMO) between September 2013 and May 2014.
Inclusion Criteria
Adults older than 65 years, belonging to the HIBA HMO and who live in Buenos Aires city, in which an abdominal and/or pelvic surgery was performed for cancer.
Exclusion Criteria
Contraindication to receive enoxaparin, high risk of bleeding (thrombocytopenia, coagulopathy, etc), history of thrombocytopenia due to heparin, severe renal failure (clearance of creatinine below 30 mL/min), patients who need full anticoagulation for any other reason (ie, atrial fibrillation), or patients participating in other investigational studies involving anticoagulants.
Definitions
A major bleeding includes those episodes of great severity requiring always hospitalization, for example, fatal bleeding and/or symptomatic bleeding in a critical organ (intracranial, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome) and/or bleeding causing a fall of 2 g/dL or more in hemoglobin levels or requiring 2 or more units of red blood cells transfusion. 18
Nonmajor clinically relevant (NMCR) bleeding includes those that does not meet the criteria for major bleeding but requires medical assistance, including surgical wound hematomas and transfusion (but only of 1 unit of red blood cells).
Finally, a minor bleeding episode includes self-limited bleeding that does not require hospitalization or transfusion such as epistaxis, gingival bleeding, petechiae, and/or bruises.
Deep venous thrombosis (DVT) is the presence of signs and/or symptoms of DVT confirmed with Doppler ultrasound or angiography showing at least a two-third occlusion of the flow in a lower and/or upper limb veins.
Pulmonary embolism is confirmed with 64-slice computed tomography pulmonary angiography that showed a filling defect in a subsegmental or larger pulmonary artery and was present in at least 2 consecutive images.
All patients were evaluated weekly by a clinical physician and a surgeon to detect bleeding (for the first 30 days) or symptomatic VTE (for 90 days). Patients receiving thromboprophylaxis at home were also assessed daily by the nurse responsible for the enoxaparin administration, until 2 days after the last dose of enoxaparin to detect bleeding complications.
Intervention
All surgeons, regardless of their experience (residents, attending surgeons, and the entire team) who performed abdominal and pelvic surgeries for cancer, received the same EIP. The contents of the EIP focused on examining the guideline recommendations, the studies on which these recommendations were made, the contraindications for enoxaparin, and examples of real-life typical cases were also given and openly discussed. 8 –18 The EIP was performed in 4 meetings of 2 hours each, every week, monthly. The EIP was developed for all the authors.
Surgically operated patients were evaluated to identify changes in the attitudes of surgeons in relation to the EP, through a cross-sectional surveillance at baseline (before educational intervention) and after the educational intervention. Surgeons were unaware of the monitoring timing to avoid biases in their attitudes in relation to antithrombotic prophylaxis. All costs related to the EP were covered by the HMO. The intervention was educational and was carried out only with surgeons. All patients were asked to provide oral informed consent to use their data from the electronic medical records, in accordance with local regulations in Argentina for an observational study. The protocol was approved by the Ethics and Research Committee of the Hospital Italiano de Buenos Aires (approval number 2309).
Statistical Analysis
All of the data analyses were performed with IBM SPSS software, version 19 (SPSS, Chicago, Illinois). Continuous variables are described as median with their standard deviations, and categorical variables are described as proportions with 95% confidence interval. The means were compared with a t test, and the proportions were compared with chi-square test or Fisher exact test. Statistical significance was considered when P < .05.
According to a prior local evaluation that showed 0% of EP use and international publications that showed less than 25%, 15 we assumed a reference value of 5%. To obtain an average improvement of 15% and considering an αerror of .05 and a power of 80%, the estimated required sample size was 53 patients. 15
Results
Before the educational intervention, 209 consecutive patients undergoing abdominal or pelvic cancer surgery were evaluated, 60 satisfied inclusion criteria and 149 didn’t because they did not belong to the HIBA HMO or they lived outside Buenos Aires city. Among these patients, 36 patients had CRC, 19 LPC, and 5 OGDC (Figure 1). Forty-six (76.6%) patients received adequate pharmacologic thromboprophylaxis with enoxaparin during hospitalization, on average for 6 days. Among patients who didn’t receive prophylaxis, there were no contraindications for prescription. The median length of hospital stay was 6.5 (5-8) days. None of these patients received EP after the hospital discharge, and the only reason was the lack of medical prescription because they were not aware of guideline recommendations. After completing the initial survey, we performed an EIP focused on thromboprophylaxis for all surgeons who treat patients with abdominal and pelvic cancer.
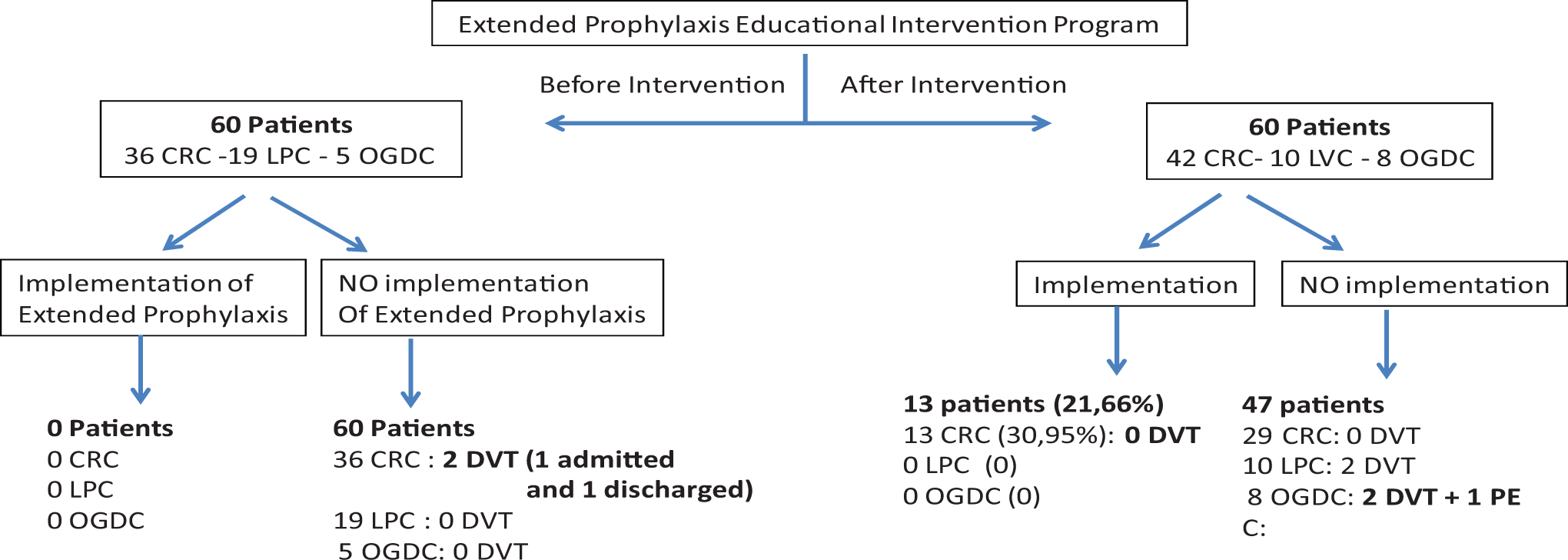
Population of patients undergoing cancer surgery before and after educational intervention program.
After the educational intervention was completed, the cross-sectional survey was repeated: 173 consecutive patients undergoing surgery for abdominal pelvic malignancies were evaluated, 113 were not included because they didn’t live in Buenos Aires city or they didn’t belong to the HIBA HMO, and finally 60 were included, 42 patients had CRC, 10 LPC, and 8 OGDC (Figure 1). During hospitalization, 58 (96.6%) patients received adequate pharmacological prophylaxis with enoxaparin for a median of 7 days. There were not any differences in the baseline characteristics between the groups (Table 1).
Baseline Characteristics of Patients Undergoing Surgery for Abdominal and Pelvic Cancer.
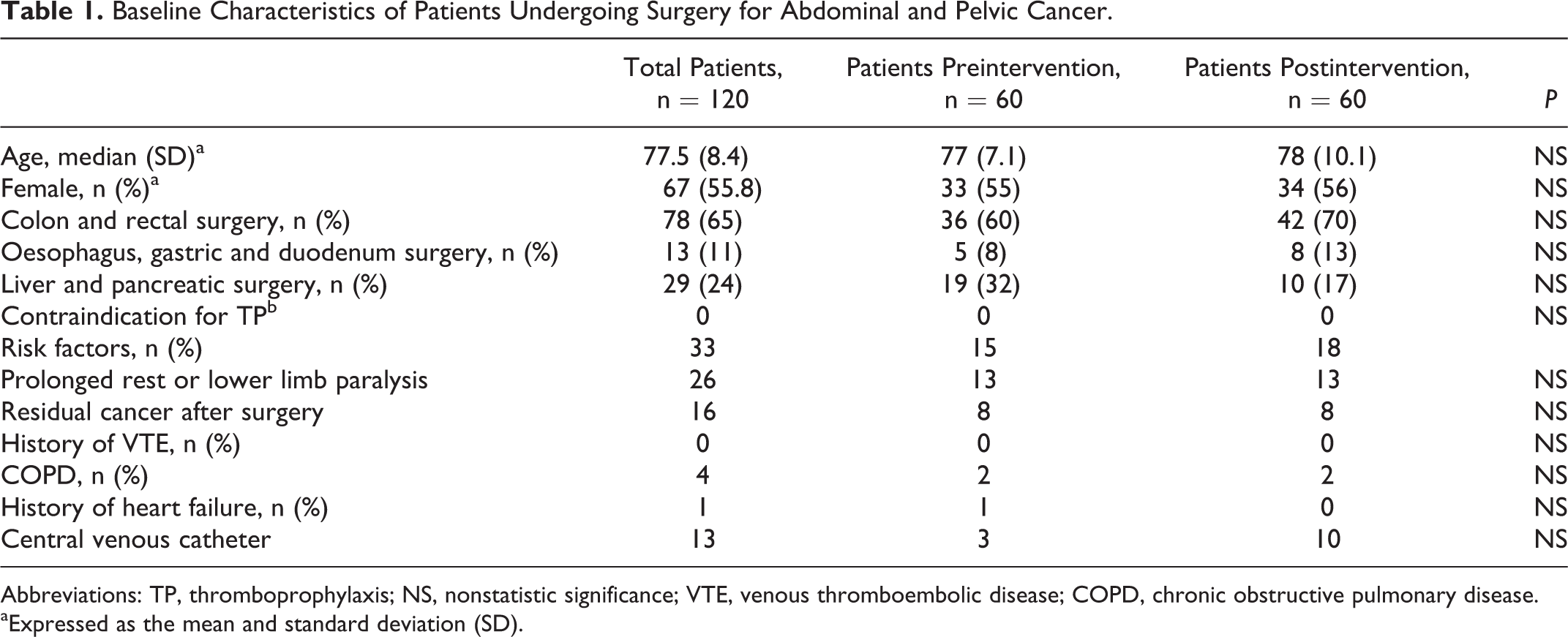
Abbreviations: TP, thromboprophylaxis; NS, nonstatistic significance; VTE, venous thromboembolic disease; COPD, chronic obstructive pulmonary disease.
aExpressed as the mean and standard deviation (SD).
In 28 (47%) patients, the prescription for EP after the hospital discharge was made but was finally accomplished in 13 for the entire 28-day period. All these patients belonged to the CRC group. Taken together, the improvement in adequacy of thromboprophylaxis after the intervention was 21.6% (13 of 60; P < .0001). However, in the CRC group, the adherence improvement was 31% (13 of 42; P < .0002).
During the 90-day survey, no deaths nor symptomatic episodes of major, NMCR, or minor bleeding were registered. Considering the entire cohort, 7 (5.8%) of the 120 patients had symptomatic VTE events, none of which had received thromboprophylaxis during hospitalization nor extended after discharge. Among patients before the EIP, there were 2 (3.33%) of 60 proximal symptomatic DVT (1 during hospitalization and the other 15 days after discharge, both in the CRC surgery group). After the EIP, there were 5 (8.3%) of 60 symptomatic VTE events, 4 proximal symptomatic DVT during hospitalization (2 in the LPC and 2 in the OGDC group), but none of these patients had received prophylaxis during hospitalization. One (2.32%) of 43 patients, who didn’t receive extended thromboprophylaxis, developed a symptomatic PE (in the OGDC group) 17 days after discharge.
Discussion
This study shows that, despite the evidence that patients in whom an abdominal or pelvic cancer surgery is performed are at a very high risk of VTE 2 –4 and that even when clinical practice guidelines recommend extend pharmacological thromboprophylaxis for 28 days after surgery, there was no adherence to the recommendations in our hospital. This finding is consistent with previous reports in which the adherence is below 25%. 15
The EIP had impact over those surgeons who were the most motivated and committed to the project, which in this study were those who care for patients with colorectal cancer but not for the other 2 subgroups.
During the EIP, all surgeons reported an understanding of the importance of the EP and stated their intention to actively engage with improved adherence to guideline recommendations. However, after the educational intervention, adherence to the recommendations of extended pharmacological thromboprophylaxis still remained low.
All surgeons simultaneously received the same educational intervention, but it only had an impact on 1 of the 3 subgroups, ruling out the difference in the type of intervention as a potential cause for the lack of adherence.
Within the group of patients evaluated in which surgery was performed for LPC, esophageal, and OGDC, there wasn’t any change in the attitude of prescription of EP after the educational intervention. The main reason reported for the low adherence of extended thromboprophylaxis with enoxaparin was the lack of prescription by the surgical team, despite the absence of contraindications in those patients. We believe that some possible causes for not prescribing prophylaxis could be the subjective belief of an elevated bleeding complication risk and that the levels of the different guideline recommendations are variable and some not strong enough. The level of recommendation is 1B for the ACCP guideline, 1A for the NICE guideline, strongly recommended for the Cochrane Database of Systematic Reviews in 2013, and in the case of the ASCO guideline requires the presence of at least a history of VTE, obesity, or residual cancer. Another cause could be the difficulty in logistics for implementation of prophylaxis at home, particularly to find trained nurses to administer subcutaneous LMWH. These variables should be measured in future research.
In the group of patients with CRC, there was a substantial improvement in prescribing thromboprophylaxis, although adherence should still be improved. It became clear that the group of surgeons who take care of patients with CRC was the most involved with the program, and this seems to be a the key factor in this kind of educational program success.
In those patients who were prescribed EP, the median number of days received was 28. No patient needed to stop prophylaxis before the indicated prescript time. The thromboprophylaxis was safe and no bleeding or deaths was registered during the follow-up. There were 7 (5.8%) of 120 cases of symptomatic VTE (all of them occurred in patients who didn’t receive extended thromboprophylaxis), which suggests very high VTE risk in these patients when thromboprophylaxis is not prescribed.
There were not any VTE events registered in patients receiving extended thromboprophylaxis, whereas 2 symptomatic VTE (1 DVT and 1 PE) were diagnosed, at 15 and 17 days, respectively, in those who did not received it.
Limitations
First, this study was conducted in a single level-3 complexity hospital and involved a limited number of patients. We believe that this experience should be repeated in other institutions, involving more physicians and patients to be validated. Second, most of the patients did not receive extended thromboprophylaxis and the main reason was the lack of medical prescription by the surgeon at charge, due to concerns about potential bleeding issues, even when those patients didn’t have objective elevated risk factors. However, in some patients, the main barrier was the inability to organize the implementation of Enoxaparin administration, due to logistical problems, mainly related to the long distance from the patients’ residence to our hospital. We believe that this barrier may be easily solved by training programs aimed at patients and their families for self-administration of enoxaparin. Although the number of patients is not sufficient to find a statistically significant difference in terms of avoiding VTE events, the sample size for this study was not calculated to assess this outcome but the difference in attitude for carrying out adherence to prescription thromboprophylaxis before and after the EIP.
Strengths
All patients were selected consecutively, reflecting the actual practice of medicine in our hospital. All patients were followed up looking for complications and no patients were lost at 90-day follow-up.
In conclusion, the EIP had a good impact (31%) but only in the CCR group. The rate of symptomatic VTE complications was high in this group of patients when they do not receive thromboprophylaxis.
To our knowledge, this is the first study in Argentina reporting adherence to guideline recommendations of extended thromboprophylaxis after abdominal cancer surgery. Although adherence is still low, this study shows that adherence can be improved with strategies such as EIPs. The knowledge of the local medical behavior and the potential barriers to the implementation of extended thromboprophylaxis may allow improved adequacy in prescribing it, and this will positively impact the safety and quality of care of our patients.
Footnotes
Authors’ Note
FV, CV, and JS contributed to conception and organization; FV, SB, and JS contributed to coordination and patient data; CV and SB contributed to analysis; FV contributed to manuscript; all authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received an unrestricted grant from Sanofi S.A.