
Abstract
Oral anticoagulants are essential drugs for the prevention of thromboembolic events in patients with atrial fibrillation (AF). Anticoagulants are, however, commonly withheld in older people due to the risk and fear of hemorrhage. Although the underutilization of anticoagulants in patients with AF has been demonstrated internationally, few studies have been conducted among aged care residents. The aim of this study was to determine the utilization of anticoagulants among people with AF residing in aged care facilities. We performed a non-experimental, retrospective analysis designed to evaluate antithrombotic usage in patients with AF in Australia residing in aged care facilities, using data collected by pharmacists while performing Residential Medication Management Reviews (RMMRs). The utilization of antithrombotic therapy and the appropriateness of therapy were determined based on the CHADS2, CHA2DS2-VASc, and HAS-BLED risk stratification schemes in consideration of documented contraindications to treatment. Predictors of anticoagulant use were determined using multivariate logistic regression. A total of 1952 RMMR patients with AF were identified. Only 35.6% of eligible patients (CHADS2 score ≥2 and no contraindications to anticoagulants) received an anticoagulant. As age increased, the likelihood of receiving an anticoagulant decreased and the likelihood of receiving an antiplatelet or no therapy increased. In patients at high risk of stroke (CHADS score ≥2), utilization of anticoagulants dropped by 19.7% when the HAS-BLED score increased from 2 to 3, suggesting that physicians placed a heavier weighting on bleeding risk rather than stroke risk. Prescribing of anticoagulants was influenced to a greater extent by bleeding risk than it was by the risk of stroke. Further research investigating whether the growing availability of direct oral anticoagulants influences practice in this patient population is needed.
Keywords
What Is Known and Objective
Atrial fibrillation (AF) is the most common sustained cardiac rhythm disorder and the most common cause of stroke in the elderly. The arrhythmia becomes more prevalent with aging and is likely to place significant stressors, both social and economic, on communities as the population ages. 1
Oral anticoagulants (OACs) are the treatment of choice for reducing stroke risk in people with AF. 2 Despite the clear benefits, anticoagulants are often underused in the elderly population and in particular residents of aged care facilities (ACFs), as they often have multiple factors, increasing their risk of both major bleeding and thromboembolic stroke. 3 –7 The severity of stroke contributes to the level of care and nursing home costs, so appropriate utilization of antithrombotics is paramount for individuals and the health system. 8
It is to be expected that some patients are not candidates for anticoagulants due to their bleeding risk profile; however, many patients do not receive beneficial treatment as bleeding risk is often overestimated. Underutilization of anticoagulants in this population has been commonly attributed to the inconvenience of INR monitoring for warfarin, poor patient compliance, or patient refusal. 3
To date, few studies have been conducted, investigating the utilization of antithrombotic therapy in people with AF residing in aged care settings. The available studies have indicated there is underutilization of antithrombotics in high-risk patients and overutilization in low-risk patients. 3,9 Larger, contemporary studies are required to present an accurate picture of utilization patterns of antithrombotics among ACF residents in light of the availability of contemporary guidelines, highlighting the benefits of anticoagulants in older patients and the introduction of direct oral anticoagulant medications (DOACs).
This study aimed to investigate the utilization pattern of antithrombotic therapies (anticoagulant and antiplatelet medications) in older people with AF in Australia who reside in ACFs.
Methods
We performed a non-experimental, retrospective study to investigate antithrombotic use for the prevention of stroke in AF in patients who had received a Residential Medication Management Review (RMMR). An RMMR is a service provided to a permanent resident of an Australian government-funded ACF. It is conducted by an accredited pharmacist when requested by a resident’s GP and undertaken in collaboration with the resident’s GP and members of the resident’s health-care team. A comprehensive assessment is undertaken to identify, resolve, and prevent medication-related problems and is provided to the resident’s GP. 10,11
The data for this study was obtained from the clinical decision-making software (Medscope®). Medscope® is a commercial tool designed to aid pharmacists in identifying issues with patient’s drug therapy while conducting medication reviews. At the time of the study, the database contained information from RMMRs conducted between January 2008 and June 2012 across Australia. All RMMRs involving patients >18 years and had a diagnosis of AF were extracted. At the time of the study, dabigatran (from April 2011) and rivaroxaban (from April 2012) were available via private prescription (with the patient paying the full cost of the medication), or through company-sponsored patient familiarization programs to selected patients (dabigatran from June 2011 and rivaroxaban from May 2012).
Data extracted from Medscope® included a summary of patient demographic information, current medications, current diagnoses, and relevant pathology data (including INR, serum creatinine, and estimated glomerular filtration rate [eGFR]). All authors reviewed the RMMR data prior to analysis.
The original Charlson comorbidity index (CCI) was calculated based on the presence of 17 specific comorbidities. We calculated the CCI by adding scores assigned to each diagnosis. 12 The CHADS2 (congestive heart failure, hypertension, Age ≥75 years, diabetes, previous Stroke), CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years [double score], diabetes mellitus, previous stroke/TIA/TE [double score], vascular disease, age 65-74 years, sex class [female]) 13 and HAS-BLED (hypertension, abnormal renal/liver function, stroke history, bleeding history or predisposition to bleeding, labile INR [defined as unstable/high INRs as recorded in the medical record of our patients], patients >65 years of age, drugs predisposing patient to bleeding [NSAIDs] or alcohol use [>8 drinks per week]) risk stratification scores were used to determine stroke and bleeding risk. 14,15
A CHADS2 score of 0 indicated that no antithrombotic was needed, a score of 1 was considered an indication for an anticoagulant or an antiplatelet agent, and a score ≥2 indicated that an anticoagulant should be used unless contraindicated. A CHA2DS2-VASc score of 0 warranted no therapy and a score ≥1 warranted an anticoagulant in men (≥2 in women). These recommendations were based on guidelines published by The American College of Chest Physicians, The American Heart Association, The European Society of Cardiology, and The Scottish Intercollegiate Guidelines Network at the time of the study. 2,16 –18
The following were considered contraindications to warfarin or antiplatelet therapy: liver dysfunction, dementia, labile INR, bleeding risk, bleeding disorder, and alcohol misuse. Peptic ulcer disease was not included as a contraindication as the database did not specify whether the disease was currently active or not. Falls risk was not included as a contraindication to antithrombotic therapy. 2,19
Dabigatran was considered to be contraindicated in the presence of a prosthetic heart valve or if the patient had an eGFR <30 mL/min. The usual dose of dabigatran is 150 mg twice a day. As the drug is renally cleared, the dose should be reduced to 110 mg daily in patients with an eGFR of 30 to 50 mL/min and in patients >75 years of age. 20,21 There were no patients in the database who had received rivaroxaban.
Data were analyzed using SPSS version 20 (IBM). 22 For testing whether 2 categorical variables were independent or related, the chi-square test or Fisher’s Exact Test was used. A P value <.05 was considered statistically significant. In comparison with more than 2 groups of normally distributed data, the analysis of variance (ANOVA) was used to test whether the groups showed an overall significant difference. In case of an overall difference, Fisher PLSD post hoc test was used for a pair-wise comparison of the individual groups. Direct logistic regression was used to determine independent predictors of anticoagulant use.
The study received ethical approval from the Human Research Ethics Committee, (University of Tasmania).
Results
The characteristics of the study sample are outlined in Table 1. The mean age of residents was 86.5 ± 6.9 years and 66.1% (1290/1952) of the sample were female. Only 0.8% (15/1952) were at low risk of stroke (CHADS2 = 0), whereas 18.8% (364/1952) were at moderate risk of stroke (CHADS2 = 1) and 80.6% (1573/1925) had a CHADS2 score ≥2. Sixty-eight percent (1325/1952) of the study sample were aged 85 years and older, and hypertension was present in 57.9% (1130/1952) of patients.
Patient Characteristics.
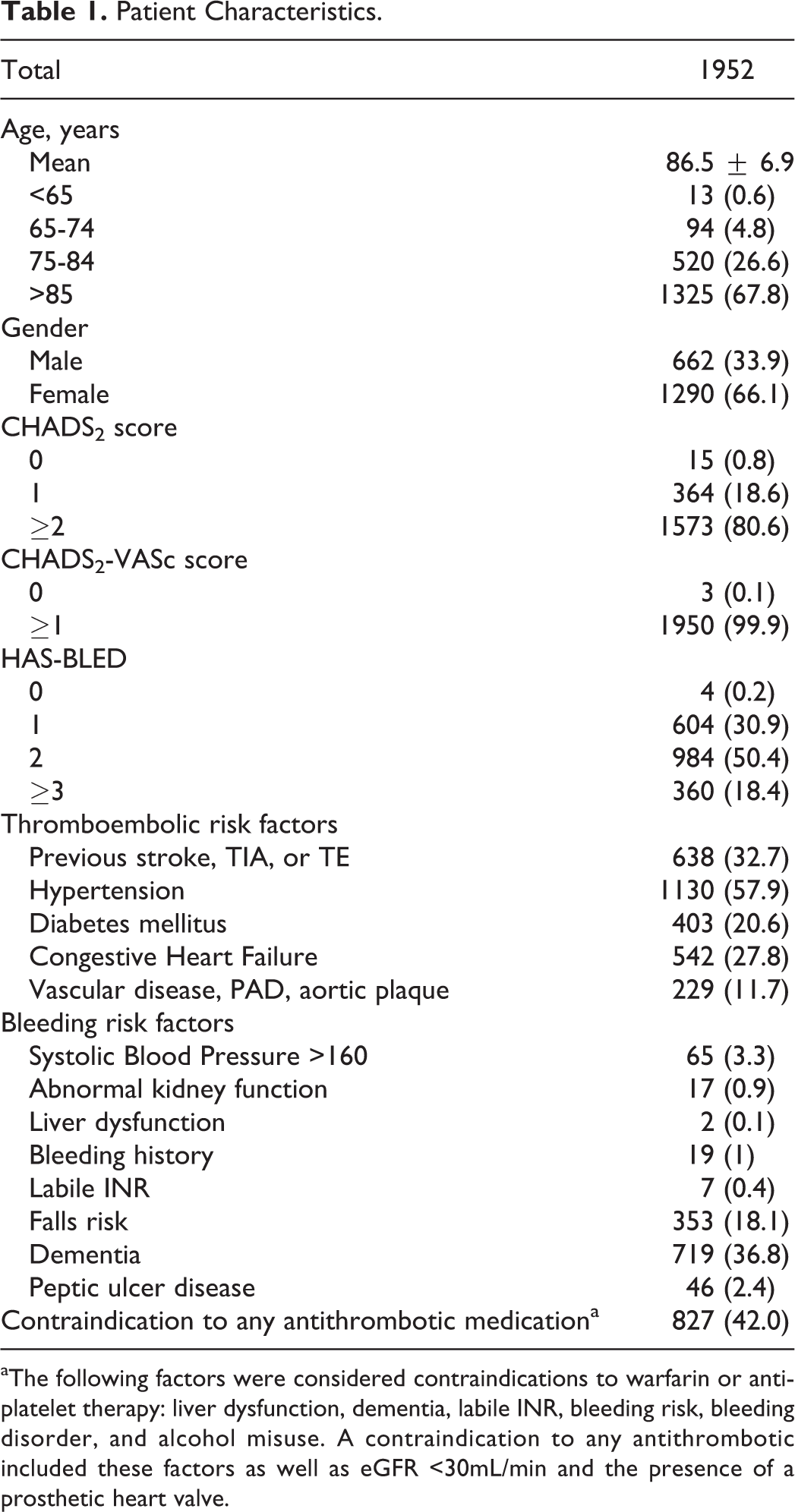
aThe following factors were considered contraindications to warfarin or antiplatelet therapy: liver dysfunction, dementia, labile INR, bleeding risk, bleeding disorder, and alcohol misuse. A contraindication to any antithrombotic included these factors as well as eGFR <30mL/min and the presence of a prosthetic heart valve.
A high risk of bleeding (HAS-BLED score ≥3) was noted in 18.4% of the population and documented contraindications to antithrombotic therapy were identified in 42.0% of patients (827/1952; contraindication to any antiplatelet agent, warfarin, or dabigatran). Slightly more men received an anticoagulant compared to women (30.2% (200/662) of men compared with 28.4% (367/1290) of women P < .001). Although dementia was considered a contraindication to antithrombotic therapy, it was observed in 36.8% (719/1952) of patients.
Table 2 shows anticoagulant use in eligible patients (those without a documented contraindication to antithrombotic therapy) with respect to the CHADS2 score and HAS-BLED score. There were a total of 365 (32.4%) patients receiving warfarin therapy and 21 (1.8%) receiving dabigatran. Of the 30 patients within the overall cohort receiving dabigatran, 9 had documented contraindications to antithrombotic therapy and were excluded from this analysis. The utilization of anticoagulants dropped by 13.5% when the HAS-BLED score increased from 1 to 2 and dropped by a further 19.7% when the HAS-BLED score increased from 2 to ≥3 in those with a high risk of stroke (CHADS2 ≥2, P < .001). In contrast to this finding; there were a total of 474 patients without any documented contraindications to antithrombotic therapy receiving antiplatelet therapy alone. The utilization of antiplatelet drugs as lone therapy increased by 31% when HASBLED score increased from 2 to ≥3 (CHADS2 ≥2, P < .001).
The Use of Anticoagulants in Relation to CHADS2 Score and HAS-BLED Score.a,b
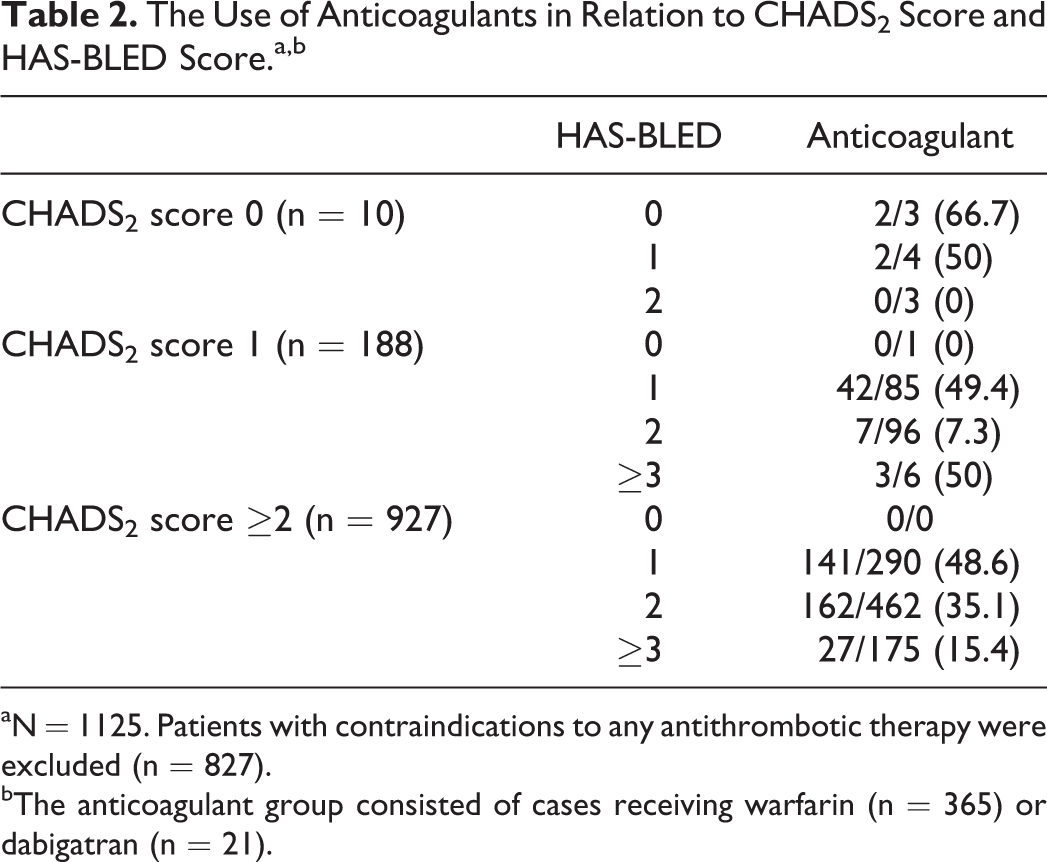
aN = 1125. Patients with contraindications to any antithrombotic therapy were excluded (n = 827).
bThe anticoagulant group consisted of cases receiving warfarin (n = 365) or dabigatran (n = 21).
Overall, 35.6% (330/927) of eligible patients (CHADS2 ≥2, and no contraindications to antithrombotic therapy) received an anticoagulant, 41.3% (383/927) received an antiplatelet medication only, and 23.1% (214/927) received no antithrombotic therapy. As age increased patients were less likely to receive an anticoagulant. Those receiving an anticoagulant were younger than those receiving an antiplatelet (P < .001). Similar results were noted when CHA2DS2-VASc was used to assess stroke risk (Table 3).
Recommended Versus Current Antithrombotic Therapy Based on CHA2DS2-VASc Score.a,b,c
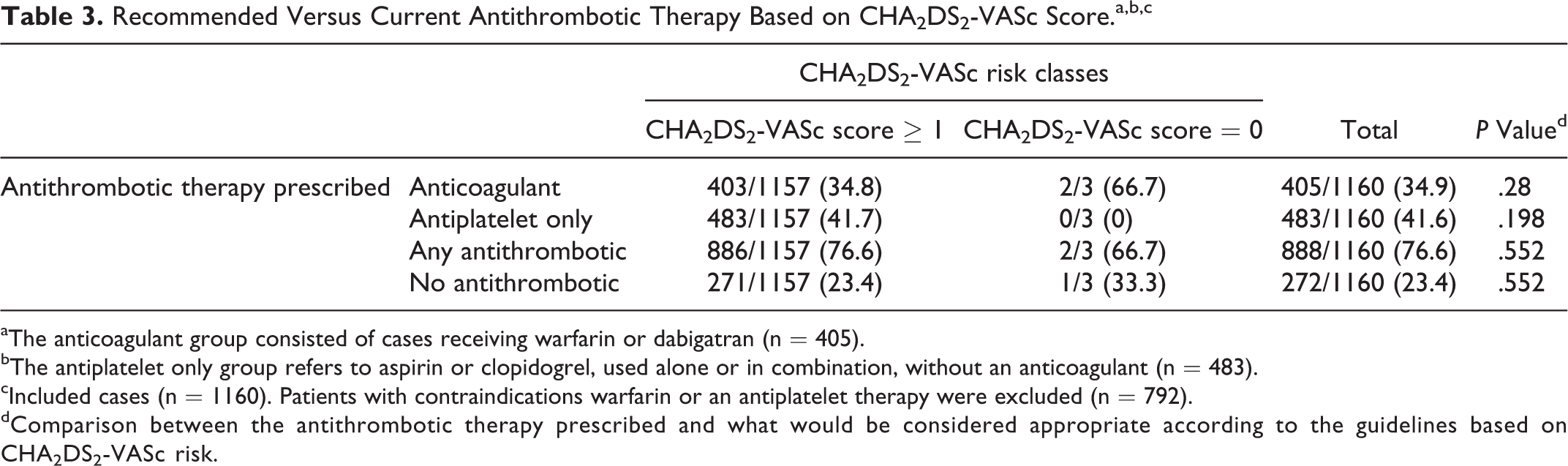
aThe anticoagulant group consisted of cases receiving warfarin or dabigatran (n = 405).
bThe antiplatelet only group refers to aspirin or clopidogrel, used alone or in combination, without an anticoagulant (n = 483).
cIncluded cases (n = 1160). Patients with contraindications warfarin or an antiplatelet therapy were excluded (n = 792).
dComparison between the antithrombotic therapy prescribed and what would be considered appropriate according to the guidelines based on CHA2DS2-VASc risk.
Only 30 patients in the sample received dabigatran, with one patient receiving a low dose when there was no apparent indication for a lower dose, and one patient receiving a low dose of dabigatran when the drug was contraindicated. The remaining patients received a dose appropriate given their age and renal function.
Logistic regression was performed to assess the impact of a number of factors on the likelihood that patients were prescribed an anticoagulant. The model contained six variables that were statistically significant in univariate analysis (age category, HAS-BLED score, CHADS2 score, previous documented stroke, TIA or TE, dementia and documented falls risk). The model was statistically significant (P < .001). The strongest predictor of receiving an anticoagulant was previous stroke, TIA, or TE (Table 4). Those who had had a previous stroke, TIA, or TE were eleven times more likely to receive an anticoagulant than those who had not (OR: 11.45, 95% CI: 8.03-16.31). History of dementia, documented falls risk, and a HAS-BLED score ≥3 were also significant negative predictors of anticoagulant usage.
Likelihood of Receiving an Anticoagulant.
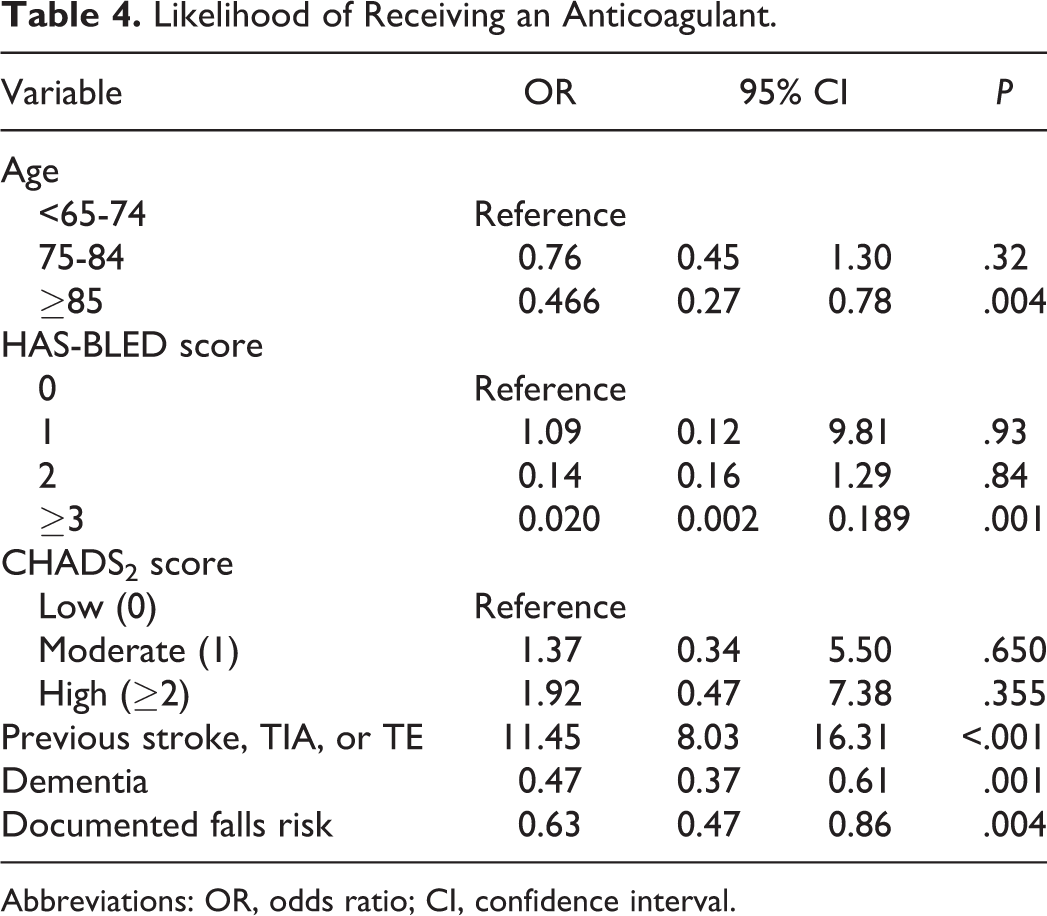
Abbreviations: OR, odds ratio; CI, confidence interval.
Discussion
Many residential care patients have AF with comorbid conditions that subject them to an elevated risk of thromboembolic stroke. Anticoagulants are typically reported to be underused and not used in accordance to guidelines. 23 –25 There is considerable overlap between stroke and bleeding risk factors, potentially causing uncertainty in the decision of whether to use OACs. Despite this, available data suggest that the net benefit falls in favor of reducing stroke risk rather than preventing bleeding, and so anticoagulants are recommended as thromboprophylaxis unless there are contraindications. 26 However, those who will gain the most benefit from anticoagulants are less likely to receive them and this issue is of particular prominence in patients residing in ACFs. 6,24,25,27 Our study found that of 1952 patients, 1157 were eligible for OACs according to the guidelines and accounting for the presence of contraindications, but only 403 (34.8%) received an anticoagulant (Table 3). This finding is in line with both local and international studies reporting that anticoagulants are commonly underutilized in ACFs. 27 –31
There is uncertainty regarding the reasons for underuse of anticoagulants. 23,28,32,33 This study found that patients who previously had a stroke, TIA, or TE were eleven times more likely to receive an anticoagulant than those without a history of thromboembolic events. HAS-BLED score ≥3, a documented diagnosis of dementia, and documented falls risk were found to be significantly independent negative predictors of anticoagulant usage.
It was noted that 36.8% of patients had dementia within the sample. Observational studies have found that patients are less likely to be treated with OACs in accordance with guidelines in the presence of dementia. 27,34 This is challenging, as patients with AF and dementia tend to have more severe strokes. 35
Guidelines recommend that a HAS-BLED score ≥3 is not grounds for withholding therapy or replacing anticoagulant therapy with antiplatelet therapy, but rather, is a signal to address potentially modifiable risk factors such as hypertension and smoking. 18 In addition, antithrombotic therapy should be selected based on the risk of thromboembolism. 36 Our study found that as the HAS-BLED score increased from a score of 1 to 2, utilization of anticoagulants in high-risk patients eligible for OAC therapy declined (see Table 3) and utilization of antiplatelet therapy increased. This finding is not uncommon in aged care facilities. 37 In addition, HAS-BLED score ≥3 was the strongest negative predictor for anticoagulant usage. 18
It is likely that fear of major bleeding is the most likely reason for the reducing use of OACs with increased HAS-BLED score. This observation is consistent with findings from the ORBIT-AF registry. 38 Some physicians associate low cognition, frailty, and high falls risk with increased bleeding rates despite lacking evidence. Although there was no way of measuring frailty in this study, falls risk was documented in the database. Patients with a documented falls risk were less likely to receive an anticoagulant (P < .005; see Table 4) in this study. In addition, OACs tend to be used less in older patients with limited life expectancy, patients with cognitive decline, and a high comorbidity level, all of these characteristics being prevalent among ACF patients. 30,31
There were only a small number of patients in the study receiving dabigatran, and no patients receiving rivaroxaban. This was to be expected as dabigatran only became available to AF patients in Australia as a private prescription in April 2011, and from June 2011 through a company-sponsored patient familiarization program. Rivaroxaban only became available as a private prescription for stroke prevention in AF during 2012.
There has been minimal investigation conducted exploring strategies to improve thromboprophylaxis in the ACF setting. Some studies suggest concerns that age, bleeding, cognition, physical function and ethnicity are incorporated into the treatment decision more so in ACFs than in the general population. 33 The ethical dilemma of prescribing in patients with a limited life expectancy, particularly drugs with the potential for adverse effects is another issue complicating stroke prevention in ACF residents with AF. More research is required around optimizing thromboprophylaxis in this setting.
Our findings are potentially limited by the retrospective nature of the study. This could have resulted in an overestimation of utilization of antithrombotics. The study was also potentially limited by the quality of documentation within Medscope®. In addition, patients with polypharmacy, who are receiving narrow therapeutic index drugs such as warfarin, with cognitive problems or falls risk may more likely receive an RMMR, and to some extent this may skew data when comparing it to a wider community. However, this study is the largest investigation of antithrombotic utilization in residential aged care AF patients in Australia, and as such, provides a valuable illustration of potential areas of concern surrounding the management of AF.
What Is New and Conclusion
This study outlines key issues in the prescribing patterns of anticoagulants in ACF residents. A high proportion of Australian ACF residents with AF who were at high risk of stroke were not prescribed an anticoagulant. In addition, a large proportion of these high-risk patients were not prescribed an anticoagulant when the HAS-BLED score increased from 2 to 3. Our results suggest that clinicians may be overly cautious when withholding anticoagulants in ACF residents. More research is needed to investigate this issue and implement strategies to reduce the risk of stroke in this growing population. Further research investigating whether the growing availability of DOACs influences practice in this patient population is needed.
Footnotes
Authors’ Note
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Luke Bereznicki reports receiving a grant from Aspen Pharmacare Australia, and receiving personal fees for the provision of expert advice from Boehringer Ingelheim Pty Ltd. outside the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.