
Abstract
Polymorphisms in vitamin K epoxide reductase complex subunit 1 (VKORC1) gene lead to interindividual variability in warfarin dose requirement. The characterization of genotype frequency distribution is required in different populations for construction of customized dosing algorithms to enhance the efficacy and reduce the toxicity of warfarin therapy. This study was carried out in Pakistani population to evaluate the contribution of common VKORC1 polymorphisms to warfarin therapy. A total of 550 stable patients taking warfarin were enrolled after medical history, physical examination, and laboratory investigations. Single blood sample was collected after informed consent. Genomic DNA was extracted and genotype analysis for VKORC1 1173C>T and VKORC1–1639G>A polymorphisms was done by polymerase chain reaction–restriction fragment length polymorphism assay. A number of samples were also analyzed by direct DNA sequencing for validation of results. Data were analyzed using SPSS version 20. Genotype frequency distributions of VKORC1 1173C>T and VKORC1–1639G>A were found to be different from other populations. Both of these polymorphisms did not demonstrate significant effect on warfarin dose requirement. Although Cytochrome P450 2C9 (CYP2C9) and VKORC1 polymorphisms together attributed only 3.8% variability in warfarin dose but it was statistically significant (p value = .004). It is concluded that there is a need to study genotype frequency distribution and their effect on warfarin dose variability among different populations due to diversity in outcome. At the same time, no effect on warfarin dose variation explained by VKORC1 polymorphisms and small variability explained by studied genotypes stresses the need for exploration of more genetic and nongenetic factors in Pakistani population.
Introduction
Warfarin has been the most commonly prescribed oral anticoagulant for various thromboembolic disorders. Warfarin results in anticoagulation by inhibiting vitamin K epoxide reductase (VKOR) enzyme. The gene coding for VKOR is VKOR complex subunit 1 (VKORC1). 1,2 Since VKORC1 breakthrough in 2004, several single-nucleotide polymorphisms (SNPs) have been identified in VKORC1 but very few of them have been found to be affecting the warfarin dose requirement. Out of these SNPs, 2 have shown significant effect on warfarin anticoagulant response. First one is a promoter polymorphism, VKORC1–1639G>A suggested to cause changes in VKORC1 transcription-binding site leading to decreased VKORC1 mRNA expression in human liver cells and decreased VKOR protein synthesis. Patients possessing A allele require less doses of warfarin as compared to those carrying G allele. Patients with genotype AA are at risk of bleeding if same dose given as required by those possessing GG genotype. The other SNP significantly affecting warfarin anticoagulant response is VKORC1 1173C>T. The carriers of TT genotype require less dose of warfarin as compared to those possessing CC genotype to produce same anticoagulation response. Both VKORC1–1639G>A and VKORC1 1173C>T have been found to be in linkage disequilibrium (LD). 3 –7
Different dosing algorithms have been constructed by researchers from data comprising of demographic factors along with the frequencies of common VKORC1 and CYP2C9 polymorphisms in their populations. The use of genotype-based dosing algorithms has shown better results in terms of improved efficacy, less adverse effects such as bleeding, and less frequent laboratory monitoring. 4,8 –12 We have already studied CYP2C9 polymorphisms and their effect on warfarin dose in Pakistani population. 13 That study data were used to assess the overall influence of both CYP2C9 and VKORC1 polymorphisms on warfarin dose requirement in present study. To expedite the use of VKORC1 genotyping along with CYP2C9 genotypes routinely in anticoagulation practice, it is imperative to determine the allelic frequency in different populations. A comprehensive dosing model that is applicable regardless of ethnicity can be developed by identifying the allelic frequency of common alleles in different ethnic populations. Pakistan, although among the top 10 populous countries in the world, has been underrepresented in pharmacogenetic studies.
The present study was carried out to determine the genotype frequencies of VKORC1–1639G>A and VKORC1 1173C>T polymorphisms in Pakistani population and to determine its effect on warfarin dose requirement. Furthermore, the combined effect of both CYP2C9 and VKORC1 polymorphisms on warfarin dose variance was assessed.
Materials and Methods
Study Settings and Protocol
The clinical data collection and laboratory investigations were done at 2 major clinical setups in Pakistan providing anticoagulation therapy—Armed Forces Institute of Cardiology Rawalpindi, and National Institute of Cardiovascular Diseases, Karachi. The analytical procedures were carried out at Centre for Research in Experimental and Applied Medicine, Army Medical College Rawalpindi in collaboration with Institute of Biomedical and Genetic Engineering Islamabad. The study protocol was approved by ethical committees of institutes.
Study Participants
The study was conducted in accordance with the current Good Clinical Practices 14 and the Declaration of Helsinki. 15 Study participants were adults of either gender between 18 and 65 years of age who were receiving warfarin therapy. Stable patients taking warfarin were recruited in the study after informed consent. A stable patient was defined as the one whose warfarin dose had been constant for at least 3 previous clinic visits over a minimum period of 3 months and had an international normalized ratio of the prothrombin time within the range of 1.5 to 3.5. 11,16 –18 The patients having hepatic and renal disease, any comorbid disease, or taking any concurrent medication or diet which would have affected warfarin therapy were excluded. All participants were Pakistani citizens belonging to different regions of Pakistan to provide representation from all areas. Each participant was evaluated by detailed medical history, physical examination, and laboratory tests.
Genotyping
A total of 550 patients were recruited in the study. A 2 mL of blood sample was collected in EDTA containing tube and stored at 4°C for genotyping. The genomic DNA from all of the samples was isolated mainly by standard organic method involving chloroform and phenol. 19 The protocol was slightly modified as per requirement of the laboratory working. DNA isolation kit was used (QIAamp DNA Mini; Qiagen Inc Valencia, CA, USA) to extract genomic DNA from some of the blood samples that were either less in quantity or somewhat clotted.
Polymerase Chain Reaction–Restriction Fragment Length Polymorphism Assay
Genotyping of the VKORC1–1639G>A and VKORC1 1173C>T polymorphisms were done by polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) assays. The sequences of forward (5′-GCCAGCAGGAGAGGGAAATA-3′) and reverse (5′-AGTTTGGACTACAGGTGCCT-3′) primers used for VKORC1–1639G>A were obtained from a reported study. 20 The sequences of forward (5′-AGAGACTTACTTAAGGTCTA-3′) and reverse (5′-TTCCAAGAAGCCACCTGGGC-3′) for VKORC1 1173C>T were kindly provided by Professor Pieter H. Reitsma. 21 The optimization of PCR with reproducible results was carried out. The PCR was carried out for each sample in a final volume of 20 μL containing, 40 ng genomic DNA (2 μL), 2 μL 10× PCR buffer without Mg2+, 1 μL of 25 mM MgCl2, 0.2 μL of 5 U/μL Taq DNA polymerase, 1 μL of 2 mM dNTPs, and 1 μL of each 20 nM forward and reverse primers. The final volume was adjusted to 20 μL with deionized water. The thermal stages included initial denaturation at 94°C for 5 minutes followed by 35 cycles of 45 seconds each of the following—94°C, 55°C, and 72°C. Final extension was carried out at 72°C for 10 minutes, and the product was subjected to digestion. The amplified DNA fragment harboring the VKORC1–1639G>A was digested with Msp1 restriction enzyme (New England Biolabs (NEB) Inc Ipswich, MA, USA), whereas for VKORC1 1173C>T, restriction enzyme Sty1 (NEB) was used. The digestion was carried out by adding 1 μL of respective enzyme (10 U/μL) and 3 μL 10× digestion buffer to 10 μL of the PCR product and adjusting the final volume to 30 μL with dH2O. The mixture was incubated at 37°C for 16 hours. The size of the RFLP bands was depicted with DNA size reference ladder.
DNA Sequencing
In order to validate the PCR-RFLP genotypes, direct sequencing of 100 samples was done through automated capillary sequencing method. Both SNPs were amplified using the same primers as mentioned in PCR. The sequencing reaction product was purified and loaded to ABI Genetic Analyzer 3130 (Applied Biosystem; Life Technologies Waltham, MA, USA) for sequencing.
The amplified PCR product was resolved at 200 bp in case of VKORC1 1173C>T polymorphism. The PCR fragment containing C allele was digested into 2 fragments of 144 and 56 bp, whereas T allele was not digested and resolved at 200 bp. The amplified PCR product was resolved at 290 bp for VKORC1–1639G>A. The PCR fragment containing G allele was digested into 2 fragments of 124 and 166 bp, whereas A allele was not digested and resolved at 290 bp.
Data Analysis
Data were analyzed using SPSS version 20.0. The genotypes and allele frequencies were estimated from the observed numbers of each specific allele, and 95% confidence interval was calculated. The expected Hardy-Weinberg (H-W) frequencies for genotypes were calculated using H-W Equilibrium equation. Genetic data for deviation from H-W equilibrium were tested using χ2 test. Analysis of variance (ANOVA) was applied for comparison of different VKORC1 genotypes with warfarin dose requirement. A p value of less than .05 was taken as statistically significant. The ANOVA was followed by post hoc Tukey test for pair-wise comparison if ANOVA gave p value of less than .05. Multiple linear regression was carried out to study the overall influence of both CYP2C9 and VKORC1 polymorphisms on warfarin dose requirement. A p value of less than .05 was taken as statistically significant.
Results
A total of 253 male and 297 female participated in the study with the mean age of 36.9 ± 12.1 years. A total of 516 samples gave successful results for VKORC1 1173C>T and 527 for VKORC1–1639G>A polymorphism. The allele and genotype frequency distribution along with expected H-W frequencies for both SNPs are given in Table 1. A p value of more than .05 in case of VKORC1 1173C>T implies that observed frequencies did not deviate from H-W equilibrium, whereas p value of less than .05 in case of VKORC1–1639G>A implies that observed frequencies are deviated from H-W equilibrium. The effect of VKORC1–1639G>A and VKORC1 1173C>T polymorphism on warfarin dose was determined, and the comparison has been summarized in Table 1. There was no statistically significant effect of different genotypes on warfarin dose requirement (p value >.05). Multiple linear regression was performed incorporating 4 common SNPs, that is, VKORC1 1173C>T, VKORC1–1639G>A, CYP2C9*2, and CYP2C9*3. The regression modeling revealed that total variation in warfarin dose explained by these SNPs was 3.8% (R 2 = .038) and was statistically significant (p Value = .004).
Allele and Genotype Frequency Distributions of VKORC1–1639G>A and VKORC1 1173C>T Polymorphisms Along With Their Relationship With Warfarin Dose.
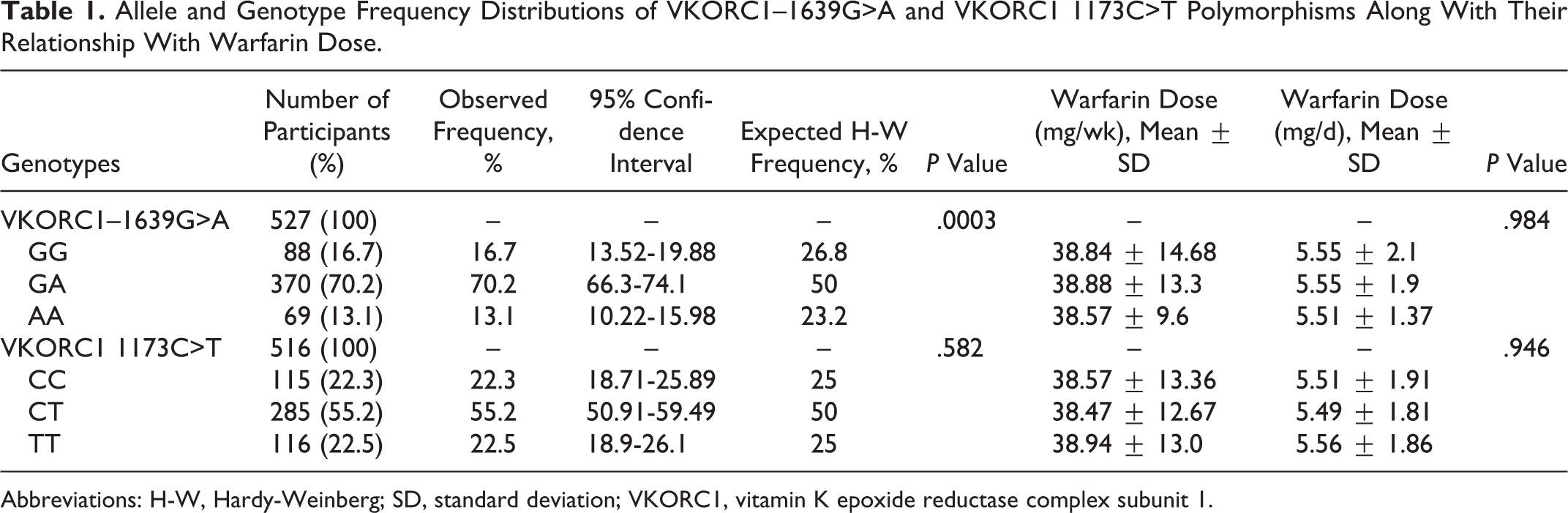
Abbreviations: H-W, Hardy-Weinberg; SD, standard deviation; VKORC1, vitamin K epoxide reductase complex subunit 1.
Discussion
This study was the first large scale study in Pakistan to report the population-based frequencies of VKORC1 1173C>T and VKORC1–1639G>A genotypes and their impact on warfarin dose requirement. The genotypes frequency distribution in Pakistani population was different from other international studies conducted in different populations as shown in Table 2. It is evident that different genotypes have diverse prevalence and effect in different populations and regions. These observations imply that every population has to have its own local frequency data. Even the population of geographically close countries may not be having same genotype frequency distribution as obvious from the results obtained from Pakistani population and those countries surrounding our geographical boundary. It is also evident from the comparison of results from studies conducted in different Asian countries that the word “Asian population” cannot be reflective of one homogenous population. Different countries in Asia have different genotypes frequency distribution so each region or country should be treated as an individual entity. It has been confirmed by some multiethnic studies conducted in Asia including participants belonging to different Asian countries. 50–52 The results of present study and the other reported studies in different parts of world in different ethnicities show how much genetic diversity is encountered all over the world. Although major part of human genome has been found to be similar among humans but still the small part is playing its part in this diversity. Different evolutionary changes have taken their toll over the period of centuries that have led to population heterogeneity across the world. Many genetic studies have been carried out to know the origin of their population to trace their ancestory. 53–57
Frequency Distribution of VKORC1–1639G>A and VKORC1 1173C>T Genotypes in Different Populations.
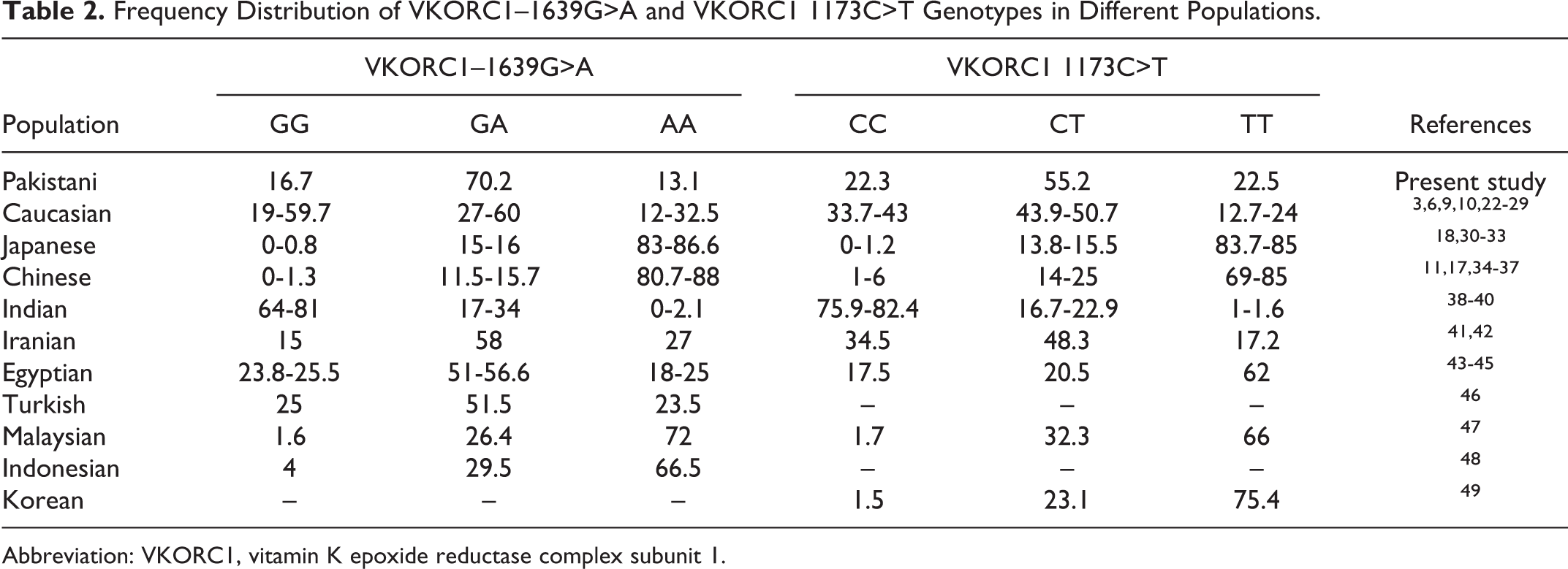
Abbreviation: VKORC1, vitamin K epoxide reductase complex subunit 1.
There are some notable findings regarding VKORC1 genotyping and their effect on warfarin anticoagulant therapy in present study. One is that there was no significant effect of VKORC1–1639G>A and VKORC1 1173C>T polymorphisms on warfarin dose requirement. The other one was that no LD between VKORC1 1173C>T and VKORC1–1639G>A genotypes was found in the present study. A number of studies have shown the presence of LD between VKORC1–1639G>A and VKORC1 1173C>T genotypes. 17,38,47 On the basis of this LD, some studies have grouped different VKORC1 SNPs into certain haplotypes, and further effect on warfarin dose requirement was then studied on the basis of these haplotypes. 12,52,58 But in our study, we did not find LD existing between these 2 SNPs. It may be due to large number of patients with heterozygous variant genotype (GA) which also made VKORC1–1639G>A not following H-W equilibrium. It is suggested that existence of either too less or too many heterozygous genotypes in data can cause deviation from Hardy-Weinberg Equilibrium (HWE). We have excluded the genotyping technique error by carrying out direct DNA sequencing as well. Pakistani population is heterogeneous and this could lead to changes in genotype presentation and number. 59–61 A number of other studies have also shown such deviation from HWE without affecting the results. 6,12,62–64 As far as the status of LD among these SNPs is concerned, a recent Italian study also reported nonexistence of LD between VKORC1 1173C>T and VKORC1–1639G>A genotypes. 10 A number of studies have revealed that different VKORC1 SNPs group differently to form haplotypes because of diverse LD relationship in different populations and their distribution varies in different populations. 8,38,52,58,65 In light of our results, it is imperative that frequency and LD studies for commonly reported VKORC1 SNPs 65,66 ought to be carried out in different populations including Pakistan to identify the haplotype structure in these particular populations.
The other noteworthy finding in present study is the effect of VKORC1 SNPs on warfarin dose requirement. In Pakistani population, both VKORC1–1639G>A and VKORC1 1173C>T polymorphic alleles did not have any significant effect on warfarin dose requirement. Majority of studies have demonstrated that the presence of variant alleles in VKORC1 1173C>T and VKORC1–1639G>A polymorphisms results in significant reduction in warfarin dose requirement. 6,10,22,23,43 Few other studies also reported similar results as ours, in which polymorphism did not show significant effect on warfarin anticoagulant response. 41,51,67 One aspect of this finding is that we have only analyzed the effect of 2 of the commonly reported VKORC1 SNPs but there are many more SNPs and mutations in other genes that have been recently studied in different populations and found to be significantly affecting the warfarin dose. 38,65,66,68,69 These polymorphisms have not only been found to be responsible for increased sensitivity to the warfarin anticoagulant response but some have been responsible for warfarin resistance which means patients possessing variant allele require more dose as compared to wild-type genotype. 4,9,10,24,70 It has also been suggested that the presence of VKORC1 Asp36Tyr polymorphic allele that leads to increased warfarin dose requirement even overrides the dose reducing effect of VKORC1–1639A allele. 71,72 This implies that there may be other VKORC1 SNPs prevalent in Pakistani population having more significant effect on warfarin dose requirement as compared to these 2 studied SNPs. There may be a possibility of existence of currently unidentified environmental factors or unknown genetic variants linked to VKORC1 genotype expression, which could influence vitamin K metabolic pathway. Another explanation comes from a recent study that has pointed out the existence of mechanisms and factors other than VKOR playing significant role in recycling of vitamin K. 73 At the same time, only 3.8% variance in dose was explained by the commonly studied SNPs (VKORC1 1173C>T, VKORC1–1639G>A, CYP2C9*2, and CYP2C9*3). In our study on CYP2C9 genotypes, for CYP2C9*2 polymorphism, there was statistically no significant difference in dose requirement among different genotypes. For CYP2C9*3, patients with homozygous variant genotype (*3/*3) warfarin dose was significantly lower than homozygous wild type (*1/*1), but the dose requirement of heterozygous variant genotypes was not significantly different. 13 That is why the overall variability caused by all 4 SNPs to the warfarin dose is small (3.8%). There is a wide range of dose variability explained by these genotypes, reported in other international studies. 10,11,24,30,31,34-35,42,46,49,72 This implies that the studied SNPs are not the significant contributor to warfarin dose variability in Pakistani population. Other SNPs and their regulators may have more contribution to warfarin dose variance in our population. Another aspect supporting our finding is that there are more than 30 gene products regulating warfarin pharmacokinetics or pharmacodynamics, and genetic polymorphisms in these genes affect warfarin anticoagulant response. Polymorphisms in some of these genes have been studied in some populations. These studies have reported substantial prevalence and significant effect on warfarin dose by these gene products. 24,34–36,44,46,62,66,69,72 These polymorphisms may be considered to be prevalent and substantial contributors to warfarin dose variability in Pakistani population. Further studies on such polymorphisms are recommended to identify the major genetic factors in Pakistani population.
Conclusion
From this study, it is concluded that the frequency distribution of VKORC1–1639G>A and VKORC1 1173C>T genotypes in Pakistani population is different from that reported in other world populations. As both VKORC1 SNPs were not found to be affecting warfarin dose requirement and also the overall effect of common CYP2C9 and VKORC1 polymorphisms on dose variance was not significant, so there is need for analysis of other SNPs in VKORC1 and CYP2C9 as well as polymorphisms in other genes reported to affect warfarin therapy.
Footnotes
Acknowledgements
The authors are thankful to National University of Sciences and Technology (NUST) for facilitating to carry out this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to Higher Education Commission of Pakistan for funding this project.