
Abstract
Purpose:
To study the safety and efficacy of rivaroxaban—a direct oral anticoagulant—use in patients with active cancer and venous thromboembolism (VTE).
Patients and Methods:
Retrospective cohort study of 400 patients with active cancer and associated VTE, defined as deep venous thrombosis and/or pulmonary embolism. This single-center study was carried out from January 2012 to June 2015. The aim of this study was to determine the efficacy and safety, using the incidence of recurrent symptomatic VTE and major bleeding, respectively, throughout the treatment with rivaroxaban.
Results:
Of the 400 patients enrolled, 223 (55.8%) were female. A total of 362 (90.5%) patients had solid tumors and 244 (61%) had metastatic disease. A total of 302 (75.5%) received initial parenteral therapy with enoxaparin (median: 3, mean: 5.6, standard deviation [SD]: 6.4 days) followed by rivaroxaban. Ninety-eight patients (24.5%) were treated with on label rivaroxaban treatment. Recurrence rates were 3.25% with major bleeding occurring in 5.5% during the anticoagulant therapy (median: 118, mean: 163.9, SD: 159.9 days).
Conclusion:
Rivaroxaban can be an attractive alternative for the treatment of cancer-associated thrombosis.
Introduction
Venous thromboembolism (VTE), defined as deep venous thrombosis (DVT) and/or pulmonary embolism (PE), is a very common comorbidity in patients with cancer. Around 20% of patients with acute VTE have either a history of cancer or active cancer. 1 Previously undetected malignant disease is often diagnosed in patients during the first months after acute presentation of unprovoked VTE. 2
Treating cancer-associated thrombosis (CAT) is challenging because anticoagulant treatment with vitamin K antagonists (VKAs) leads not only to a high risk of recurrent VTE but also to a high risk of serious bleeding. 3 –5 Contrary to VKAs, low-molecular-weight heparins (LMWHs) can have predictable pharmacokinetic profiles and few drugs interactions. 6
The 2016 American College of Chest Physicians guidelines still suggest that the initial treatment for CAT should be carried out with injectable LMWHs over VKAs and over any direct oral anticoagulants (DOACs) such as rivaroxaban, apixaban, dabigatran, or edoxaban. 7 However, the adherence to LMWH is very low, particularly because of the inconvenience of daily injections and its cost. 8
In the 2 pivotal clinical trials, where oral rivaroxaban was evaluated for the treatment of VTE (EINSTEIN and EINSTEIN-PE trials), 9,10 the results were consistent with all DOAC trials for the VTE treatment when compared to heparin followed by VKA—same efficacy profile with significantly lower bleeding rates was observed in noncancer patients. 11 The subgroup analysis for the CAT treatment in these trials also suggests that DOACs have the same efficacy of standard therapy (enoxaparin followed by VKA) with less major bleeding. However, given the small sample size, a total of 354 in the rivaroxaban group and 301 allocated to enoxaparin and VKA arm, strong recommendations cannot be issued regarding the CAT treatment with DOACs. 12
Since major clinical trials comparing DOACs to LMWHs for CAT are underway, we have evaluated the efficacy and safety of oral rivaroxaban for CAT treatment at a single center in a large number of patients.
Patients and Methods
The review board of AC Camargo Cancer Center approved this study. This was a retrospective cohort in a cancer hospital. The aim of this study was to evaluate the efficacy (recurrence of symptomatic VTE or VTE-related death) and safety (major bleeding and clinically relevant no major bleeding) of oral rivaroxaban for CAT treatment. There were 400 consecutive patients assessed with active cancer and symptomatic acute VTE from January 2012 to June 2015.
Active cancer was defined as a diagnosis of cancer, other than basal cell or squamous cell carcinoma of skin, or treatment for malignancy within 3 months before the episode of VTE. The malignant disease was grouped as solid or hematologic cancer.
All VTE episodes were confirmed by objective tests (ultrasonography or helical computed tomography). Lower limb DVT was classified as distal when involving infrapopliteal segment and proximal veins when involving up to iliac–femoral veins. Upper limb DVTs were classified as distal when involving brachial and distal veins and proximal when involving internal jugular or axillary/subclavian veins.
Every patient was informed that LMWH is recommended by the guidelines for initial treatment for CAT. Most of these patients decided for DOACs based especially on the high cost and subcutaneous administration of LMWH and due to the need of laboratory monitoring of VKAs. In the hospital setting, patients are treated with LMWH since their health insurance covers all expenses, but when they are discharged and they have to purchase their medication, LMWH is exchanged for rivaroxaban. In general, patients with PE and proximal DVT were referred for prompt hospitalization. When VTE was treated in hospitalized patients they received parenteral therapy with full dose of enoxaparin (1 mg/kg body weight twice daily) followed by rivaroxaban 20 mg once daily, once they are discharged. Outpatients, for whom hospitalization was not required, received on label rivaroxaban treatment (15 mg oral rivaroxaban twice daily for 3 weeks followed by 20 mg once daily).
Demographic details, medical history including patient’s gender, age, weight, creatinine clearance, parenteral agent initiated on, were recorded. To describe how the disease impacts patient’s daily life, Eastern Cooperative Oncology Group (ECOG) performance status was used. The ECOG score is divided into 5 grades—from 0, patients fully active, able to carry on all predisease performance without restriction, up to 5, dead. Additional VTE risk factors comprehending previous VTE event, use of antiplatelet medications, immobilization, recent surgery, combined treatments (chemotherapy, radiotherapy, and hormonal therapy), and percentage of upper versus lower DVT were registered.
Fatal PE, in the absence of autopsy, was defined as any death appearing within the first 5 days after PE diagnosis, in the absence of any alternative cause of death. Fatal bleeding was defined as any death occurring within the 5 days after a major bleeding episode, in the absence of an alternative cause of death.
The principal safety outcome was major bleeding defined as a decrease in hemoglobin level of ≥2 g/dL, transfusion of ≥2 units of packed red blood cells, bleeding that occurred in a critical site (intracranial, intraspinal, intraocular, pericardial, intra-articular, intramuscular with compartment syndrome, or retroperitoneal), or bleeding that was fatal. 13
Clinically relevant nonmajor bleeding was defined as overt bleeding that did not meet the criteria for major bleeding but was associated with medical intervention, unscheduled contact with a physician, interruption or discontinuation of anticoagulant drug, or discomfort or impairment of activities of daily living (ISTH bleeding definition criteria). 14
The major exclusion criteria were active bleeding or a high risk of bleeding, treatment with dual antiplatelet therapy, aspirin (≥165 mg daily) treatment of the index VTE with surgical thrombectomy, thrombolysis, and calculated creatinine clearance of <25 mL/min, hemoglobin level of <9 g/dL, or platelet count of <100 000 mm3.
Statistical Analysis
Continuous numerical variables were reported as means with standard deviation. Categorical variables were reported as percentages and compared using the χ2 test or Fisher exact test as appropriate. Statistical analyses were conducted with STATA software for Windows release 7.0 (STATACorp 2001, Statistical Software, College Station, Texas).
Results
The demographic and clinical characteristics of the patients along with the types of cancer are shown in Table 1.
Clinical Characteristics and Patients Demographics.
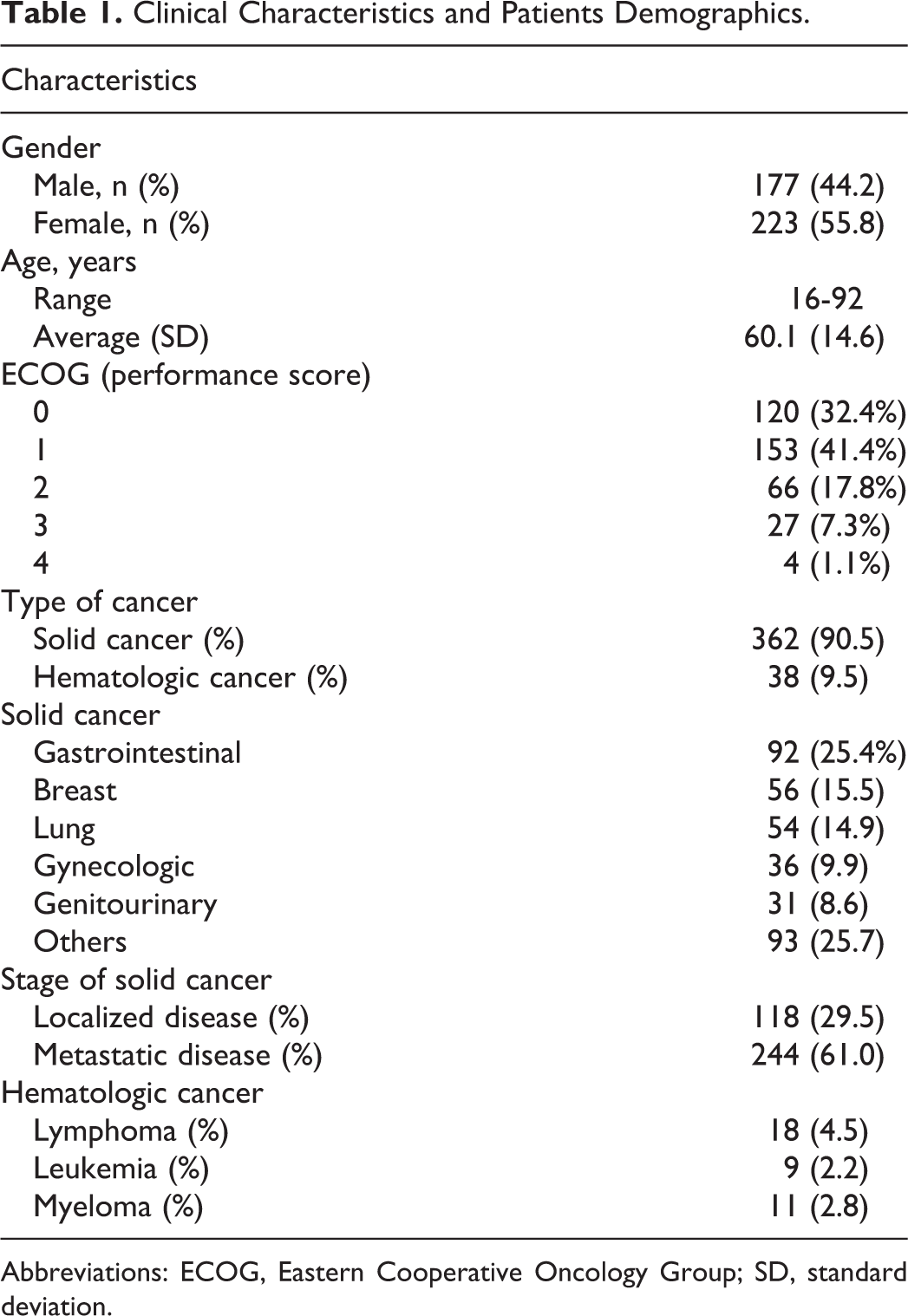
Abbreviations: ECOG, Eastern Cooperative Oncology Group; SD, standard deviation.
There was a predominance of female patients (55.8%). Age ranged from 16 to 92 years (median: 62, mean: 60.1, standard deviation [SD]: 14.6). Thirty-one (8.4%) patients had poor clinical performances, ECOG score of 3 or 4.
Approximately 90% of the patients had solid tumors and 61% had metastatic disease. The gastrointestinal tract was the most frequent site of cancer (25.4%), followed by breast cancer (15.5%). As observed from Table 2, a total of 116 (29.1%) patients presented with PE (with or without concomitant DVT) and 284 (70.9%) DVT alone.
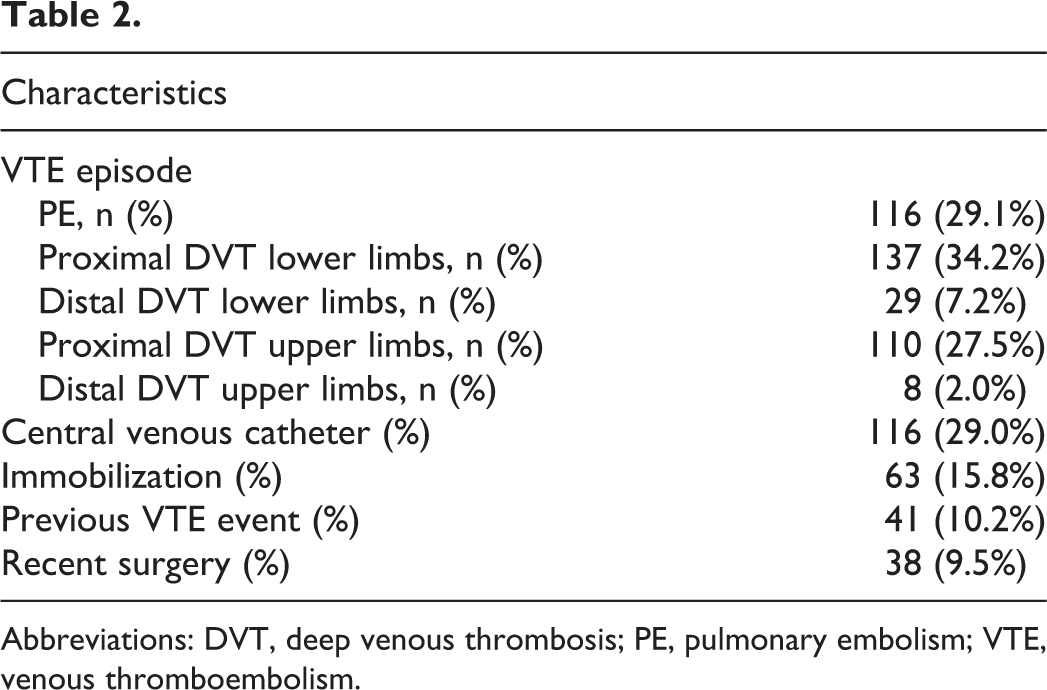
Abbreviations: DVT, deep venous thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
Previous VTE event had occurred in 41 patients. A total of 116 patients had long-term central venous access, which was associated with VTE in 77 patients.
Most of the patients (302 [75.5%]) received parenteral therapy with enoxaparin (median: 3, mean: 5.6, SD: 6.4 days) followed by rivaroxaban. Enoxaparin was prescribed during patients’ stay at the hospital. Ninety-eight (24.5%) patients were treated with on label rivaroxaban treatment.
The median time of anticoagulation in our study was 118 days (mean: 163.9, SD: 159.9). During 6-month anticoagulation period 117 (29.2%) patients died, of which, 115 was due to the cancer progression.
Venous Thromboembolism Recurrence
Recurrent VTE occurred in 13 (3.25%) of the 400 patients, during the course of anticoagulation. Of these 13 patients, 9 (69.2%) occurred in the first 2 months, 3 (23%) between 3 and 6 months, and 1 (7.8%) after 6 months of therapy (Figure 1). According to the site of the recurrences, 8 were DVT, whereas 5 were isolated PE. One of these 5 PE was fatal.
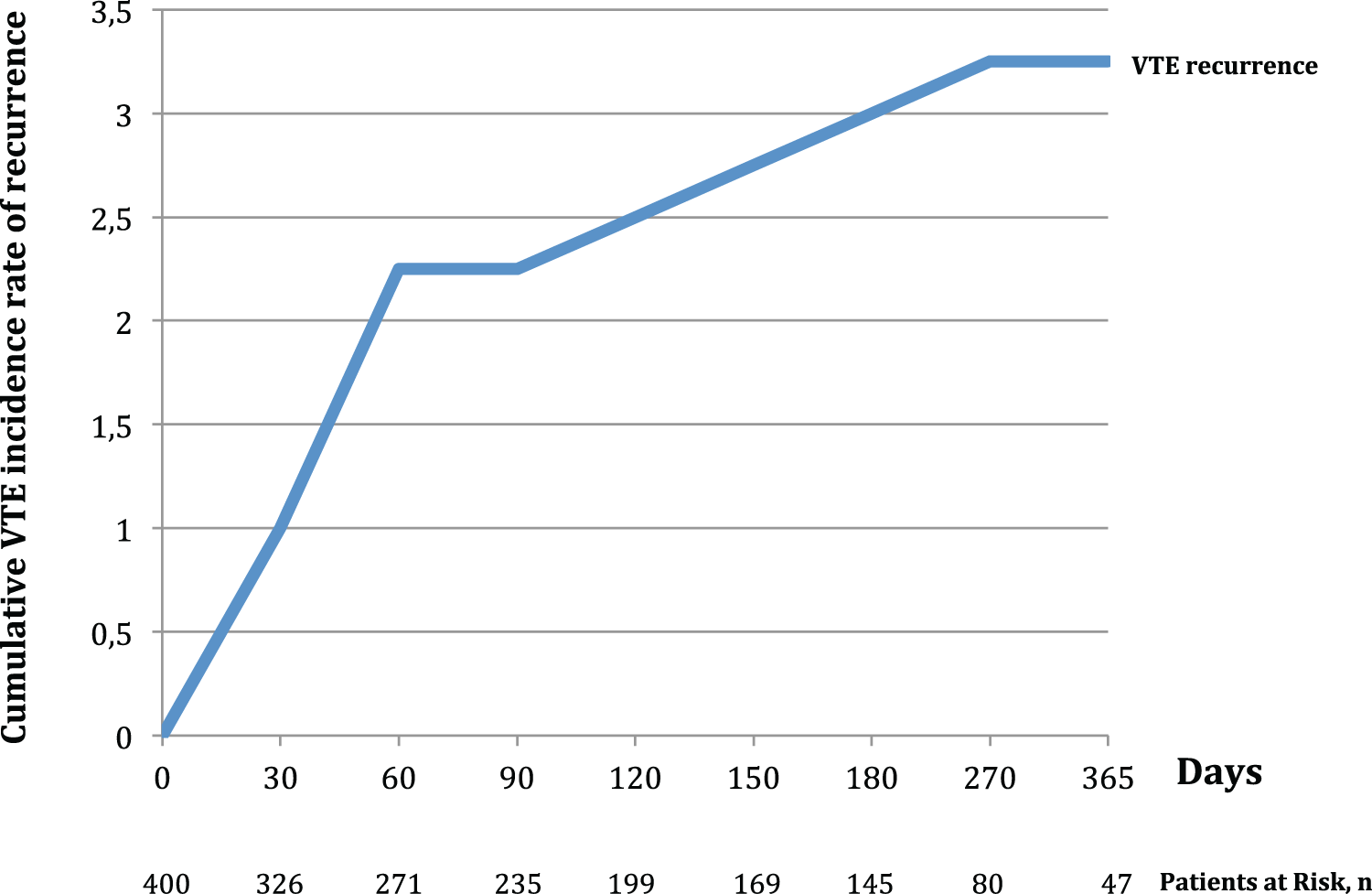
Kaplan-Meier curve for cumulative incidence of VTE recurrences.
There were higher rates of recurrent VTE in patients with previous episodes of VTE than in those without (4 [10.8%] of 37 vs 9 [2.5%] of 350; P = .034). There was no significant difference (increase) in the incidence of VTE recurrence between on a label regimen of rivaroxaban (4.1%) compared to LMWH + rivaroxaban (3.0%) group (P = .530).
Major Bleeding
Major bleeding occurred in 22 (5.5%) of the 400 patients and in 1 was fatal. Of these 22 patients, 13 (59%) occurred in the first 2 months, 7 (32%) between 3 and 6 months, and 2 (9%) after 6 months of anticoagulation (Figure 2).
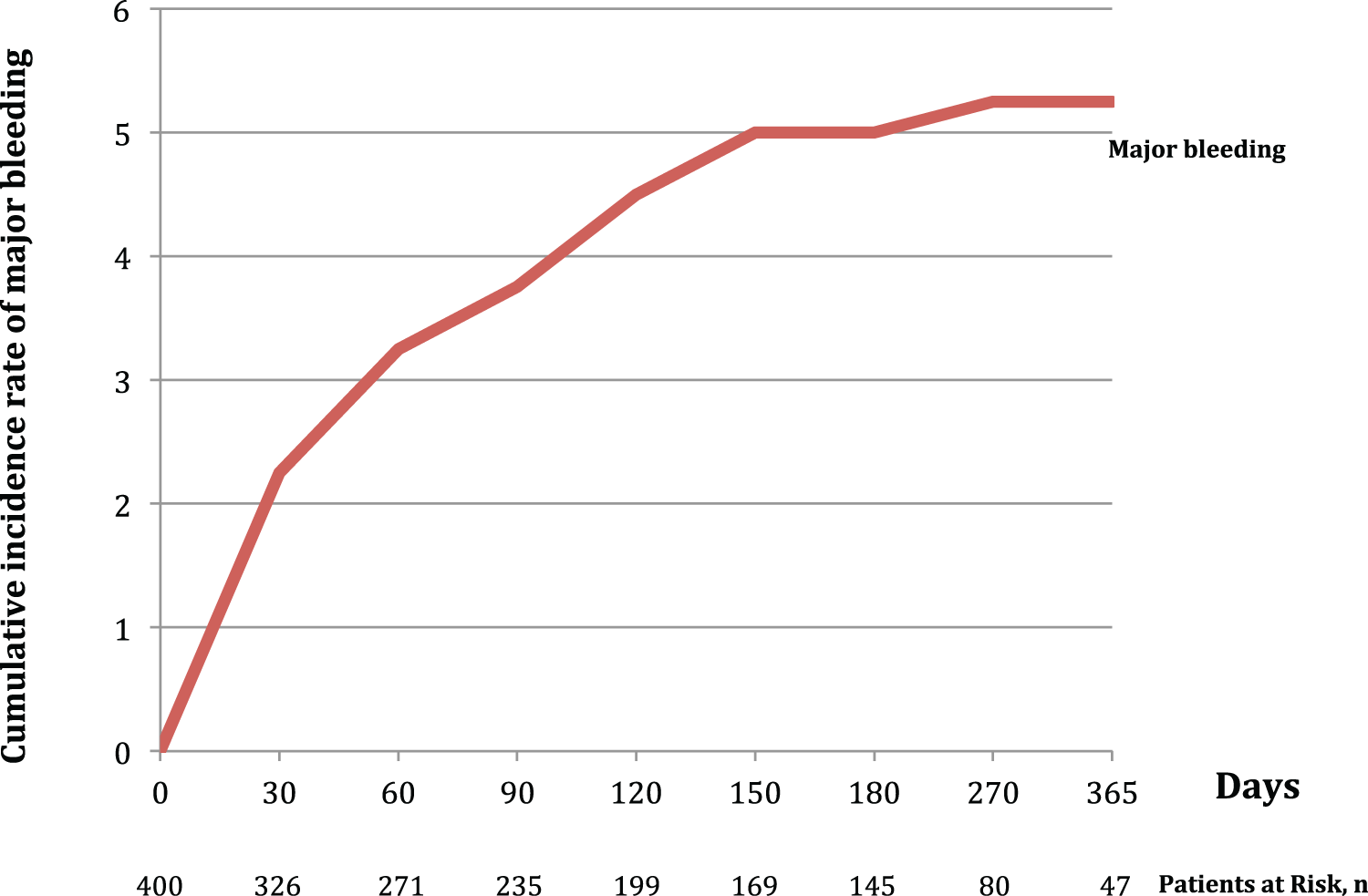
Kaplan-Meier curve for cumulative incidence of major bleeding.
A nonsignificant difference was observed in the incidence between on a label regimen of rivaroxaban (3.2%) compared to LMWH followed by rivaroxaban (6.3%) group (P = .958).
Nonmajor Bleeding
Nonmajor bleeding occurred in 61 (15.2%) patients. Patients with higher ECOG score are more likely to have any bleeding (10.8%, 15.7%, 24.2%, and 25.8%, in patients with ECOG scores 0, 1, 2, and 3 + 4, respectively; P = .053).
Discussion
This retrospective cohort analysis allowed describing a large number of patients with active cancer treated with rivaroxaban for VTE.
One of the largest online databases of VTE patients, the Registro Informatizado de Enfermedad TromboEmbólica (RIETE), provide “real-world” information of VTE recurrences and major bleeding in patients with CAT. 15 In the RIETE study, 44 704 patients were enrolled, of whom 7911 had active cancer. The anticoagulation treatment was not standardized and included the use of LMWH, unfractionated heparin, Fondaparinux, or VKA. During the course of anticoagulant therapy (mean: 181, SD: 210 days), 178 (4.3%) patients with cancer, developed recurrent PE and 194 (4.7%) had recurrent DVT. In our study, we observed 1.25% and 2% of recurrent PE and DVT, respectively, throughout anticoagulant therapy (mean: 163.9, SD: 159.9 days). Major bleeding was observed in a large proportion of patients in the RIETE study (8.9% vs 5.5%) of our population.
Current guidelines recommend a 6-month course or longer of LMWH over the treatment with VKA or DOAC for patients having cancer with VTE, because LMWH has been shown to be more effective. These recommendations are based mainly on a single trial (CLOT trial), where despite the 50% relative risk reduction in recurrences in patients treated with dalteparin (hazard ratio [HR]: 0.48; P = .0002), nonsignificance was observed but trending high rates of major bleeding (6% vs 4%; P = not significant), when compared to heparin followed by VKA. 16 –18
A subgroup analysis of the EINSTEIN program showed that in patients with CAT, recurrent VTE occurred in 16 (5%) of the 354 patients allocated to rivaroxaban and 20 (7%) of the 301 patients allocated to enoxaparin and VKA (HR: 0.67, 95% CI: 0.35-1.30). Major bleeding occurred in 8 (2%) of the 353 patients receiving rivaroxaban and in 15 (5%) of the 298 patients receiving standard therapy (HR: 0.42, 95% CI: 0.18-0.99), suggesting that rivaroxaban might be an attractive option for treating CAT. In our patients, we observed 3.25% of VTE recurrences and 5.5% major bleeding. Our data are consistent with the EINSTEIN subgroup analysis, same efficacy profile with acceptable bleeding rates.
A single-center experience treating CAT with rivaroxaban was recently reported. Two hundred ninety-six patients with VTE received rivaroxaban and there was no control group. Patients enrolled in this study had at least 3 months of follow-up. Of these, 118 (40%) had an active malignancy and 178 had no cancer. There was no difference in VTE recurrence between the malignant (3.3%) and the nonmalignant (2.8%) groups (P = .533). A trend to higher rates of major bleeding (2.5% vs 0%; P = .06) and nonmajor clinically relevant bleeding (5.9% vs 0.6%; P = .08) was observed in patients with cancer. 19 In spite of the fact that it is a small sample of patients with CAT treated with rivaroxaban, this study may also indicate low rates of VTE recurrences.
The drawbacks of our study are its retrospective design and the fact that there is no control group. However, the amount of patients enrolled is quite large and the results are favorable to the use of rivaroxaban in this setting. Besides, the treatment regimens were not standardized and some patients received initial therapy with LMWH. Nevertheless, as mentioned, there were no significant differences regarding the VTE recurrence or bleeding between on a label regimen of rivaroxaban compared to LMWH followed by rivaroxaban group.
Although LMWH is effective in patients with CAT, it is inconvenient. At first, it requires daily subcutaneous injections, particularly in patients with cancer, who receive frequent intravenous chemo or immunotherapy and second LMWH is very expensive in some countries. The cost of LMWH in our country is very high (6 times higher than rivaroxaban), a strong reason for patients to prefer oral treatment. For these reasons, many patients having cancer with VTE continue to be treated with VKA or DOAC worldwide.
Finally, we have also evaluated patients who received parenteral therapy with LMWH followed by 20 mg rivaroxaban once daily, instead of the studied initial 15 mg rivaroxaban loading dose twice daily. Even though there were higher rates of major bleeding with the off-label strategy, 6.3% compared to 3.2% in the on-label group, no significant differences were observed between the groups. Recently a report from our group indicated that transitioning directly from LMWH to rivaroxaban is safe and well tolerated. 20
Conclusion
The results of this retrospective cohort analysis suggest that rivaroxaban may be a convenient option to treat patients with CAT. Additional studies are warranted to confirm this concept and to compare rivaroxaban (and other DOAC) with LMWH in patients having cancer with symptomatic VTE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.