
Abstract
This is a retrospective cohort study of adults with a primary diagnosis of deep venous thrombosis (DVT) unaccompanied by pulmonary embolism (PE), seen in 4 emergency departments in 2013 and part of 2014. The purpose was to assess the prevalence of home treatment of DVT in the present era of new oral anticoagulants. Among 96 patients with DVT and no PE, 85 (88.5%) were hospitalized and 11 (11.5%) were discharged to home. Most of the patients discharged to home received low-molecular-weight heparin, 9 (81.8%) of 11. None were prescribed new oral anticoagulants. Early discharge in ≤2 days occurred 28 (32.9%) of 85 patients. Most (64.3%) received enoxaparin and/or warfarin at early discharge. Rivaroxaban was prescribed in 7 (25.0%) of those discharged in ≤2 days. We conclude that in some emergency departments, patients with DVT are uncommonly discharged to home even though new oral anticoagulants are available.
Between 1990 and 1995, it had been suggested that home treatment of deep venous thrombosis (DVT) with initial treatment with low-molecular-weight heparin was safe, effective, and cost effective in carefully selected patients. 1 –3 In 1996, 2 randomized controlled trials further supported the observation that initial home treatment of DVT with low-molecular-weight heparin was effective and safe. 4,5 Many subsequent investigations showed patients treated entirely at home. 6 –19 However, there was a slow implementation of home treatment of DVT through 2006. 20 This, in part, may relate to logistical problems involving home injections of low-molecular-weight heparin, including teaching patients or family how to administer subcutaneous injections or obtaining home nursing care. These problems can be overcome through the use of new oral anticoagulant agents. The oral factor Xa inhibitors rivaroxaban and apixaban were approved for the initial and continuing treatment of DVT by the US Food and Drug Administration on November 2, 2012, and August 21, 2014, respectively. 21,22 In this investigation, we assess the prevalence of home treatment of DVT in the present era of new oral anticoagulants.
Methods
This was a retrospective cohort study of patients aged ≥18 years with a primary diagnosis of DVT unaccompanied by pulmonary embolism (PE), seen in 4 emergency departments in 2013. At one of these centers, patients were seen through August, 2014, and at another through September, 2014. The purpose was to determine the prevalence of home treatment of patients with a primary diagnosis of DVT unaccompanied by PE in the era of new oral anticoagulants. Collaborating sites were McLaren Oakland Hospital, Pontiac, Michigan; Summa Akron City Hospital, Akron, Ohio; St Mary Mercy Hospital, Livonia, Michigan; and University of Toledo, Medical Center of Ohio, Toledo, Ohio. The medical records of patients aged 18 years or older seen on the emergency service with a primary diagnosis (first-listed diagnosis) of DVT and no PE were manually reviewed. These records were identified by searching for patients discharged from the emergency service with International Classification of Diseases, Ninth Revision, Clinical Modification codes 451.1, 451.2, 451.8, 451.9, 453.2, 454.8, 453.9, 671.3, 671.4, and 671.9.
Deep venous thrombosis was diagnosed in the emergency departments by venous compression ultrasound. Pulmonary embolism was ruled out by computed tomographic (CT) pulmonary angiography in patients in whom PE was suspected. Computed tomographic pulmonary angiography was not performed routinely in those in whom PE was not suspected. Patients were excluded if they had PE in addition to DVT, a prior history of DVT, or if DVT was not the primary diagnosis. There were no specific criteria or guidelines for hospitalization. This investigation was approved by the Institutional Review Boards of each of the participating centers.
Statistical Methods
Differences of categorical variables were calculated by the 2-tailed Fisher exact test using GraphPad Software (San Diego, California). Differences in means of continuous variables were assessed by Student unpaired t test.
Results
During the period of investigation, 245 000 patients were seen in the emergency departments of the participating hospitals. Ninety-six patients were identified with a primary diagnosis of DVT and no evidence of PE. Among these, 85 (88.5%) were hospitalized and 11 (11.5%) were discharged to home. Most of the patients discharged to home received low-molecular-weight heparin, 9 (81.8%) of 11. Two (18.2%) patients with DVT limited to the calf veins received no anticoagulants.
Early discharge in 2 days or less occurred in 28 (32.9%) of 85 patients (Figure 1). Antithrombotic therapy prescribed at early discharge was enoxaparin alone, 7 (25.0%), enoxaparin with warfarin or warfarin alone, 11 (39.3%), rivaroxaban,7 (25.0%), inferior vena cava filter with no anticoagulant, 2 (7.1%), and no antithrombotic therapy, 1 (3.6%).
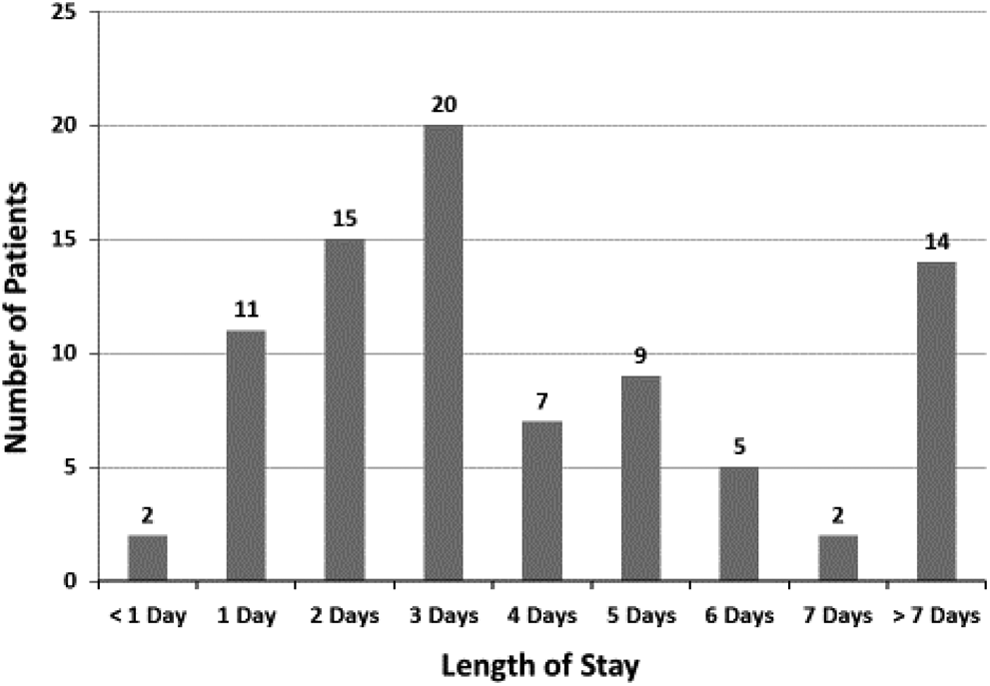
Length of stay in hospital in patients with a primary diagnosis of deep venous thrombosis.
Among those with no comorbid conditions, 11 of 40 (28%) were treated at home versus 0 of 56 (0%) treated at home with any comorbid conditions (P < .0001; Table 1). Comorbid conditions identified in hospitalized patients are shown in Table 2. Among 29 hospitalized patients with no comorbid conditions, 19 (65.5%) were younger than 60 years of age.
Age, Gender, Comorbid Conditions, Severe Leg Pain, and Proximal Site of Deep Venous Thrombosis.
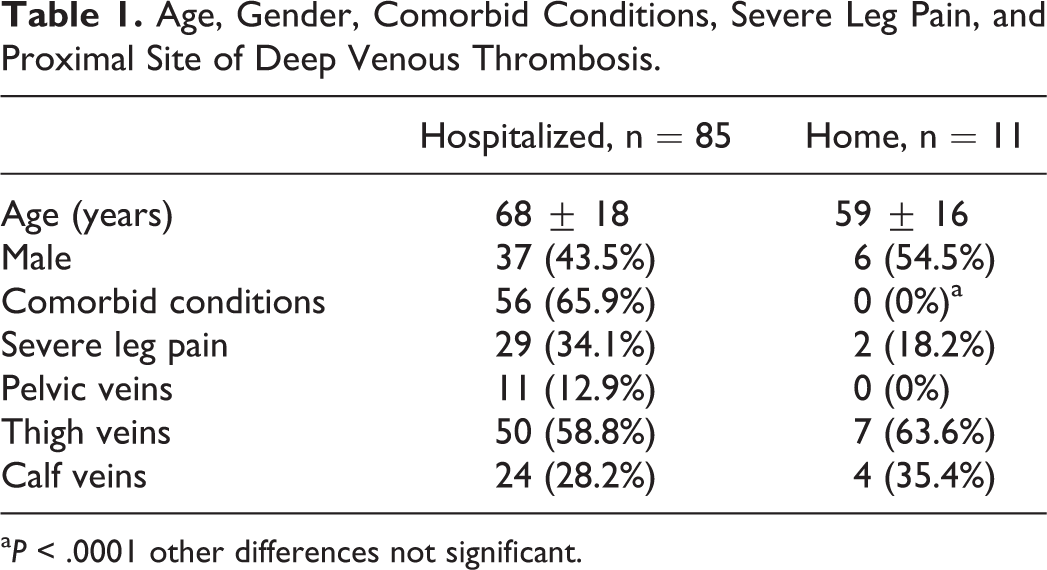
a P < .0001 other differences not significant.
Comorbid Conditions in Hospitalized Patients.a
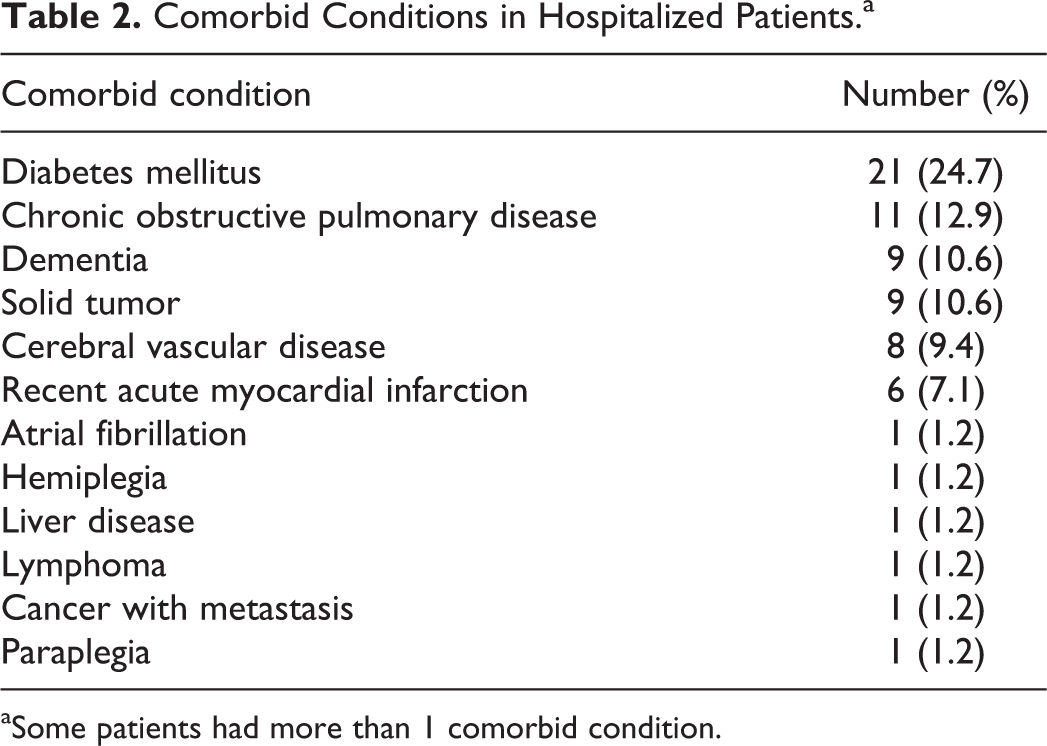
aSome patients had more than 1 comorbid condition.
Hospitalized patients tended to be older, but the difference was not statistically significant (Table 1). Genders were similar among hospitalized patients and those sent home (Table 1). There was no significant difference in the prevalence of DVT at various sites, comparing hospitalized patients with patients treated at home, but the number at each site was small in home-treated patients (Table 1).
Discussion
In the present era of new oral anticoagulants, only 11.5% of patients in 4 midwestern emergency departments with a primary diagnosis of DVT and no evidence of PE were discharged to home from the emergency department. New oral anticoagulants were not prescribed for patients treated entirely at home and were prescribed in the minority of those discharged from the hospital in 2 days or less. Hospitalized patients had a higher prevalence of comorbid conditions than home-treated patients, but other factors, with small numbers of patients, did not differ significantly.
Slow implementation of home treatment was observed before new oral anticoagulants became available. 20 By 2006, the proportion of the adult population hospitalized with a primary diagnosis of DVT was only 21% less than the proportion hospitalized in 1979. 20 However, early discharge within 2 days increased from 5% in 1979 to 21% to 25% in 2004 to 2006. 20 Our present data showed early discharge in one-third of hospitalized patients with DVT and no evidence of PE. Most received low-molecular-weight heparin and/or warfarin at discharge.
In 2004, outpatient treatment of DVT was recommended by the American College of Chest Physicians “if possible.” 23 The American Society of Health-System Pharmacists in 2004 indicated that outpatient treatment of DVT offers the opportunity to dramatically reduce the cost of treating DVT and improve the quality of life without compromising clinical outcomes. 24 In 2012, the American College of Chest Physicians in their evidence-based clinical guidelines recommended treatment at home over treatment in hospital in patients with acute DVT whose home circumstances are adequate and patients do not have severe leg symptoms or comorbidity. 25 However, these guidelines suggested treatment with vitamin K antagonists or low-molecular-weight heparin over new oral anticoagulants. 25
Cautious exploration of the safety of home treatment may explain its slow implementation. 20 At least 23 editorials, reviews, and tutorials urged a flexible, sensible, and cautious approach or cautioned for careful patient selection, necessary logistical support, infrastructure, organization, patient education, and compliance or monitored outcome; and these were cited previously. 20 Changes in clinical practice do not occur immediately with the evolving literature but occur over years. 26
Regarding the 2 patients with DVT limited to the calf veins who were discharged from the emergency department without treatment with anticoagulants, this was in accordance with the 2012 guidelines of the American College of Chest Physicians. 25 In patients with acute isolated distal DVT of the leg without severe symptoms or risk factors for extension, serial imaging of the deep veins for 2 weeks was recommended over initial anticoagulation. 25
A strength of this investigation is that it is the only one of which we are aware that assesses home treatment of DVT since the availability of new oral anticoagulants. A weakness is that few patients were found who were treated at home. This limited our ability to assess factors that impacted the decision for home treatment or hospitalization.
Our sample is small and not necessarily representative of practice in emergency departments throughout the United States, much less North America. However, in 4 emergency departments that are unaffiliated with each other, the admitting practices for DVT were similar. Patients with acute DVT usually were not discharged for home treatment, even though new oral anticoagulants were available. We conclude, therefore, that at the present time, it is not uniform practice to treat patients with acute DVT as outpatients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.