
Abstract
Effects of warfarin and new-generation direct oral anticoagulants (DOACs) on thrombus resolution after the treatment of deep vein thrombosis (DVT) are still unknown. The study aimed to investigate the effects of warfarin and DOACs on thrombus resolution after DVT treatment.
Introduction
In the light of current guidelines, low-molecular-weight heparin along with vitamin K antagonists, which are conventionally used for treating deep vein thrombosis (DVT), have been replaced by direct-acting oral anticoagulant (DOAC) as they are easy to use, elicit rapid anticoagulant effect, and have no need for monitoring. 1
Although anticoagulant drugs do not have a fibirinolytic effect, they might accelerate thrombus resolution by strongly inhibiting prothrombotic activity when being used for the treatment of DVT. The aim of the DVT treatment is to relieve the symptoms, suppress the progression of thrombus, and prevent pulmonary thromboembolism and other complications secondary to DVT by inducing adequate anticoagulation. 2
After the development of femoropopliteal DVT, the competition between residual venous thrombosis (RVT) and recanalization determines the clinical course of DVT. 3 The extent and duration of the balance created between these 2 factors by DOACs or warfarin, a vitamin K antagonist used in the treatment of DVT, are unclear. RVT is associated with post-thrombotic syndrome (PTS) and recurrent venous thromboembolism (VTE) after DVT, and it can increase the risk of developing cancer and cardiovascular diseases. 4
Owing to this information, the use of anticoagulants in the treatment of DVT has become crucial, but the extent of effectiveness of these drugs for recanalization and thrombus resolution is not clearly known. Therefore, we investigated the rate of recanalization and factors affecting recanalization upon administering anticoagulant therapy in patients with femoropopliteal DVT.
Methods
After obtaining the approval from Hitit University Faculty of Medicine Ethics Committee (decision no. 10/03/2021-403), the patients were retrospectively analyzed using the hospital data system.
Patients in whom DVT was associated with recent trauma or surgery (<1 month), cancer, hormone therapy, pregnancy or puerperal period, or hospitalization for more than 1 week were considered provoked DVT cases, whereas patients without these factors were considered unprovoked DVT cases.
In the treatment of DVT, warfarin was used in combination with subcutaneous enoxaparin at doses determined in accordance with the weight of the patient. This treatment was given until the international normalized ratio was within the therapeutic dose range (2.0-3.0), which is when the enoxaparin therapy was discontinued. DOACs were used at the doses recommended by the manufacturer and current guidelines. Oral anticoagulant (warfarin, rivaroxaban, apixaban, and dabigatran) therapy was discontinued when recanalization was observed during follow up.
Whole leg ultrasound scans of the included patients were performed by 3 senior radiologists using the same device (LOGIQ V2, GE Healthcare, Chicago, IL, USA). “Complete recanalization” was defined as the absence of RVT in the femoral and popliteal veins, presence of response to compression, and presence of venous flow for at least 6 months during follow up after the diagnosis of acute femoropopliteal DVT.
Patients were divided into 2 groups: complete recanalization and no recanalization. The groups were compared in terms of demographic data, etiology of DVT, and used anticoagulant drugs.
Statistical Analysis
The variables were investigated using visual (histograms and probability plots) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk test) to determine the normality of their distribution. Normally distributed, continuous variables were expressed as mean ± standard deviation, whereas non-normally distributed variables were expressed as median values with ranges. The categorical variables were expressed as number and percentage. The demographic parameters and follow-up data were compared using Mann–Whitney U test and chi-square test. The hazard ratio and 95% confidence intervals (CI) were determined using different cox proportional-hazards models to identify the independent predictors of recanalization with adjustment of the predefined possible risk factors. A P-value of <.05 was considered statistically significant, and statistical analyses were performed using the Statistical Package for the Social Sciences statistical software program for Windows version 15.0 (SPSS Inc., Chicago, IL, USA).
Results
We analyzed 1432 patients diagnosed with DVT in our clinic between January 2016 and January 2021. A total of 666 patients diagnosed with femoropopliteal DVT who had accessible complete medical records without missing data were included in the study.
The demographic data of the patients are summarized in Table 1. The mean follow-up time was 23.6 ± 17.8 months (range 1-72 months; median 17 months). Recanalization was observed in 59.5% (396 of 666) patients during the follow-up period. We compared patients with (group 1) and without recanalization (group 2) and found that patients in group 1 were younger than those in group 2 (59.73 vs 64.97 years; P < .001). Although 56.6% male patients were recanalized, this rate was higher in female patients (64.0%), this difference was not statistically significant (P = .060).
Demographic Characteristics of Patients.

Abbreviations: CAD, coronary artery disease; CRF, chronic renal failure; DM, diabetes mellitus; HT, hypertension.
When the etiology of DVT was investigated, recanalization was observed in 63.6% and 58.1% patients with provoked and unprovoked DVT, respectively (P = .208). Comorbidities such as hypertension (HT), diabetes mellitus (DM), coronary artery disease (CAD), and cancer were significantly more common in group 2 than in group 1. There was no difference between the 2 groups in terms of the types of drugs used in treatment (P = .208). Similarly, a comparison of the usage of warfarin and new-generation oral anticoagulant did not show significant difference between the groups (P = .071).
For further analyses, Cox regression models were used to investigate the factors affecting recanalization; when the variables with significant differences between the 2 groups (age, HT, DM, CAD, and cancer) were examined, a relatively low rate of recanalization was observed in patients with CAD (Odds ratio [OR] 2.3; 95% CI: 1.6-3.4; P < .001) and DM (OR 1.5; 95% CI: 1.1-1.9; P = .009). In other models, factors such as gender and medication were added (Table 2), and it was indicated that the rate of recanalization may be 1.5 times higher in women than in men. No significant difference between the warfarin and DOAC groups was found in terms of drugs usage (OR 1.03; 95% CI: 0.8-1.4; P = .8339). However, the Cox regression analysis comparing all drugs individually revealed that rivaroxaban and apixaban showed similar effects as warfarin for recanalization (OR 0.7; 95% CI: 0.5-1.1; P = .082 and OR 0.8; 95% CI: 0.4-1.5; P = .468, respectively). However, recanalization was relatively less common in patients using dabigatran (OR 0.7; 95% CI: 0.5-0.9; P = .008) (Figure 1).
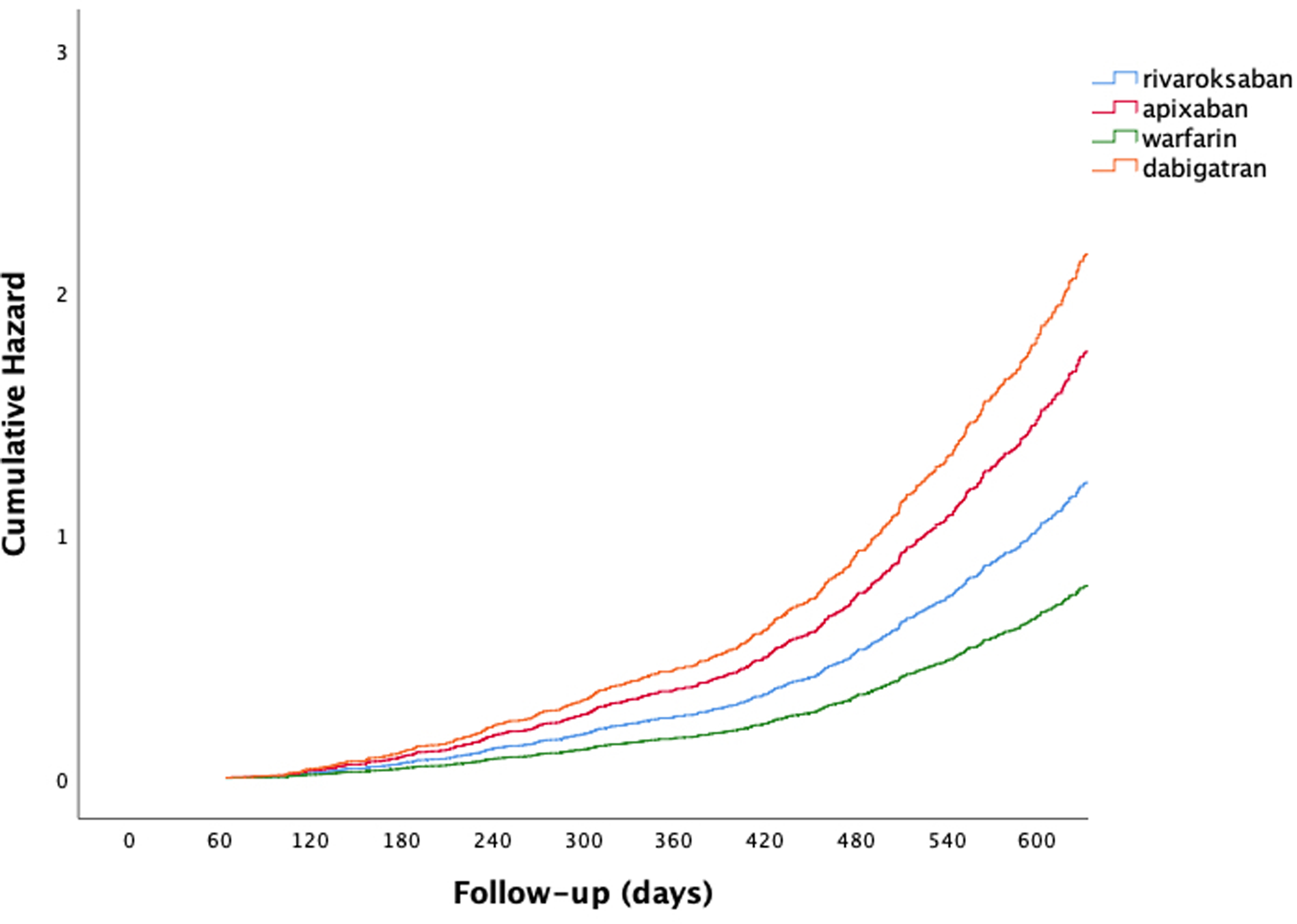
Cumulative risk in Cox regression analysis of 4 types of oral anticoagulants. Rivaroxaban and apixaban showed similar effects as warfarin (OR 0.7; 95% CI: 0.5-1.1; P = .082 and OR 0.8; 95% CI: 0.4-1.5; P = .468, respectively), while recanalization was relatively lower for dabigatran (OR 0.7; 95% CI: 0.5-0.9; P = .008). Abbreviations: CI, confidence interval; OR, odds ratio.
Distribution of Drugs Used in DVT Treatment.

Abbreviation: DVT, deep vein thrombosis.
Discussion
This study revealed the similar effects of warfarin and DOAC drugs on thrombus resolution in femoropopliteal DVT. In addition, DM, CAD, and male gender were revealed as the negative predictive factors for recanalization.
The development of recanalization after DVT depends on the balance between the inflammatory response elicited by the thrombus in the vein wall and spontaneous lysis. 5 Few studies have examined the time required for developing recanalization after DVT upon administering DOACs and warfarin. Rivaroxaban is the most studied DOAC. However, to the best of our knowledge, no study has compared the effectiveness of all actively used DOACs and warfarin for recanalization.
Few previous studies have examined the effects of rivaroxaban on thrombus resolution and recanalization after DVT. In the oral direct factor Xa inhibitor BAY 59-7939 in patients with acute symptomatic deep vein thrombosis study–DVT series, partial or total thrombus resolution was found in 45.9% and 43.8% to 59.2% patients who were administered different doses of rivaroxaban and enoxaparin/VKA therapies, respectively, in the first 21 days after DVT diagnosis. 6
In the Einstein-J study, 100 patients with acute DVT were examined and 26.7% thrombus resolution was observed on day 22 in patients under rivaroxaban therapy, whereas this rate was 15.8% in patients receiving standard therapy. 7 However, the number of patients in this study was limited and the follow-up periods were limited to days.
In our study, similar effects of warfarin and rivaroxaban on thrombus resolution were observed during the median follow-up period of 17 months (OR 0.7; 95% CI: 0.5-1.1; P = .082 and OR 0.8; 95% CI: 0.4-1.5; P = .468, respectively).
Most researchers agree that thrombus resolution and recanalization generally occurred in the first 3 months after DVT. 8 However, the persistence of RVT and inadequate thrombus resolution are associated with the development of PTS, 9 which generally occurs after 1 to 2 years of the onset of DVT with an incidence rate of 20% to 50%.10,11
Therefore, it can be concluded that inadequate thrombus resolution and slow recanalization are important in the development of PTS. Although the development rates of PTS between the groups were not examined in our study, the similar recanalization rates of warfarin in patients on rivaroxaban and apixaban therapy may help in suppressing the development of PTS in these patients in the future.
A study conducted by Karathanos et al 12 compared the rates of PTS development after using rivaroxaban and warfarin and it was shown that rivaroxaban was more effective than warfarin in preventing the development of PTS.
The remarkable effect of rivaroxaban in improving recanalization, resolving thrombus, and preventing PTS has not yet been observed in other DOACs.
Wik et al 13 also found a difference between the effect of dabigatran and warfarin on the prevalence of PTS and development of recurrent DVT. When the drug groups were individually evaluated in this study, the similar effects of rivaroxaban/apixaban and warfarin on thrombus resolution and recanalization were observed; however, we did not observe the same effect in patients using dabigatran probably because a small number of patients used dabigatran.
It is still unclear whether the risk factors for idiopathic DVT and atherosclerotic cardiovascular risk factors are common.
In the previous studies, VTE was not found to be a risk factor for atherosclerosis in 2 large cohort studies.14,15 However, in recent studies, the relationship between idiopathic DVT and atherosclerosis has been demonstrated, albeit not clearly. 16
In our study, low thrombus resolution after DVT was found in patients with DM and CAD. As researchers, we believe that atherosclerotic events such as DM and CAD should be considered risk factors for the development of DVT and thrombus development after DVT. However, multicenter studies are needed to confirm this theory.
In addition, thrombus resolution was 1.5 times higher in women than in men included our study. Male gender is considered a risk factor for atherosclerotic diseases; atherosclerotic diseases are less common in women than in men. As high thrombus resolution and low incidence rate of atherosclerosis was seen in women in our study, it might reflect the relationship of sex of the patient with incidence rate of atherosclerosis and DVT resolution.
In a meta-analysis study conducted by Gregson et al, 17 risk factors for atherosclerotic cardiovascular diseases such as smoking, obesity, and advanced age were found to be the risk factors of VTE.
In conclusion, the treatment of DVT is important to prevent the potential risks that may arise when if not treated effectively.
D-dimer is degradation product of cross-linked fibrin that increase in the setting of acute thrombosis and that is valuable in the setting of new diagnose. In normal range of D-dimer levels, we can exclude acute thrombosis but of the note false negative tests might occur after initiation of anticoagulation. 18 Nowadays, D-dimer testing is recommended in patients with unlikely clinical findings, whereas patients with strong clinical evidence should directly go to imaging without D-dimer testing. 19
Currently, the use of DOACs is recommended by guidelines for the treatment of VTE.1–16,20 However, there are a few studies showing thrombus resolution after DVT using DOACs.
Limitations
The major limitation of our study is its single center and retrospective nature. Multicenter studies in which patient groups can be prospectively examined may yield reliable results. In addition, a registry-based study can provide effective evidence. In our study, we aimed to examine the effectiveness of DOACs currently available in the market. The nonrandomized use of DOAC in this study can be considered as another limitation. In addition, major bleeding, which is a major complication for all anticoagulant drugs, was not examined in this study.
Another important limitation is that we did not investigate the D-dimer and fibrin levels to assess the fibrinolytic activity.
Conclusion
We have shown that DOACs, especially rivaroxaban and apixaban, are as effective as warfarin in thrombus resolution. Furthermore, we believe that thrombus resolution may also depend on the gender and comorbidities present in the patient, particularly the presence of atherosclerotic cardiovascular risk factors.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.