
Abstract
Objective:
The cutoff values of fibrin-related markers (FRMs) diagnosing or predicting the occurrence of a venous thromboembolism (VTE) were evaluated.
Materials and Methods:
Fibrin-related markers such as fibrin monomer complex (FMC), D-dimer, and fibrinogen and fibrin degradation products (FDPs) before surgery were measured in 326 patients undergoing orthopedic surgery to diagnose subclinical VTE or predict postoperative VTE.
Results:
Although the FMC, D-dimer, and FDP levels were all useful for the diagnosis of acute VTE, the FDP level was not useful for diagnosing subclinical VTE or predicting postoperative VTE. The results of several D-dimer assays closely correlated with other D-dimer assays. There were various cutoff ranges for diagnosing or predicting VTE. Some D-dimer assays were useful for diagnosing low levels of D-dimer and others were useful for diagnosing moderate to high D-dimer levels. Increased D-dimer levels were useful for diagnosing acute (cutoff values: 2.0-5.9 μg/mL) or about 10% of subclinical VTE (cutoff values: 3.4-5.3 μg/mL), for predicting about 10% of postoperative VTE (cutoff values: 3.4-5.3 μg/mL), and for excluding VTE.
Conclusion:
Although increased D-dimer levels were useful for diagnosing subclinical VTE and predicting the risk of VTE, there were various cutoff values for the diagnosis or prediction of VTE.
Introduction
Acute venous thromboembolism (VTE) 1 –4 is one of the most serious complications to occur after orthopedic surgery. A pulmonary embolism (PE) 5 –7 is a potentially fatal disease that is usually caused by deep vein thrombosis (DVT). Fibrin-related markers (FRMs) such as D-dimer, soluble fibrin (SF)/fibrin monomer complex (FMC), and fibrinogen and fibrin degradation products (FDPs) are useful markers for diagnosing thrombosis (TH), while FDPs are used in the diagnosis of disseminated intravascular coagulation (DIC) 8 and VTE. 9,10 A D-dimer assay is used as an initial screening test in the emergency department to exclude the diagnosis of PE. The purpose of this test, which has a high negative predictive value (NPV), is to provide a fast and cost-effective way to triage patients with VTE. 11,12
Orthopedic surgery has been reported to be strongly associated with postoperative VTE. 13,14 The incidence of VTE ranges from 41% to 85% after total knee arthroplasty (TKA) and from 42% to 57% after total hip arthroplasty (THA), with screening in the absence of thromboprophylaxis. 15 Many studies have established the efficacy of low-molecular-weight heparin as a prophylactic treatment against VTE in patients undergoing orthopedic surgery. 16 –18 Furthermore, direct oral anticoagulants 19,20 have recently become available for prophylaxis after surgery. These anticoagulant therapies have significantly reduced the incidence of VTE.
Although it was reported that the measurement of the D-dimer and SF levels can be used to predict the incidence of DVT after THA or TKA without the use of anticoagulants, 21 this ability to predict a postoperative VTE is canceled following the administration of fondaparinux or edoxaban. 20,22,23 It was recently reported that mild elevation of the D-dimer level suggested a risk for subclinical VTE and postoperative VTE. 20
The objective of this study was to determine the adequate cutoff levels of various D-dimer kits for diagnosing subclinical VTE and predicting postoperative VTE before surgery and to examine the relationships among various D-dimer kits.
Materials and Methods
Three hundred twenty-six patients undergoing major orthopedic surgery (241 THA and 85 TKA; median age [25th-75th percentile]: 68.0 years [60.0-75.0 years]; females: n = 263; males: n = 63) who were treated with 30 mg of edoxaban (Daiichi Sankyo, Tokyo, Japan) and intermittent pneumatic compression for prophylaxis against DVT between January 1, 2013, and February 29, 2016, at Mie University Hospital were enrolled to this single-center study. Patients with a high bleeding risk, defined as a decrease of more than 2 g/dL hemoglobin, were excluded from the analysis. All of these patients in the cohort received 30 mg of edoxaban once per day for 14 days, beginning 24 hours after lumbar anesthesia extubation.
The FRMs were also measured in 44 patients with acute VTE (median age: 46.5 years [38.0-62.0 years], females: n = 21; males: n = 23) in another group and 50 healthy volunteers (HVs; median age: 20.0 years [18.0-21.5 years], females: n = 24; males: n = 26) and were compared to those of patients undergoing orthopedic surgery. We defined acute VTE as symptomatic VTE, whereas those with subclinical VTE had no symptoms in the present study; 21 patients had PE, while 23 patients had proximal DVT. In these patients, blood sampling was performed within 3 days after the onset of VTE.
The presence of DVT in the patients who underwent orthopedic surgery was assessed by a whole-leg compression ultrasound examination using the standardized ultrasound criteria for venous noncompressibility before surgery and on days 4 and 14. 21 –23 The PE and acute DVT in patients with acute VTE were diagnosed by a whole-leg compression ultrasound examination and/or enhanced computed tomography. The study protocol was approved by the Human Ethics Review Committee of Mie University School of Medicine, and signed informed consent was obtained from each participant. This study was carried out in accordance with the principles of the Declaration of Helsinki.
The FRMs were measured in plasma before surgery, which was frozen at −80°C. The plasma levels of FDP and FMC were measured according to the latex agglutination method using LIASAUTO P-FDP (Sysmex, Kobe, Japan) and Auto LIA-FM (Sysmex), respectively. The plasma levels of D-dimer were measured according to the latex agglutination method using LIASAUTO D-dimer Neo (D-dimer A; Sysmex), LPIA-ACE D-Dimer II (D-dimer B; LSI Medience Corporation, Tokyo, Japan), INNOVANCE D-Dimer (D-dimer C; Siemens, Marburg, Germany), and VIDAS D-Dimer Exclusion II (D-dimer D; bioMerieux, Marcy l’Etoile, France), respectively.
Statistical Analysis
The cutoff values of FRM for predicting postoperative DVT and diagnosing acute VTE and subclinical VTE, excluding VTE, and evaluating VTE risk were analyzed. Diagnosing acute VTE: A receiver operating characteristic (ROC) analysis of FRMs was performed between patients with acute VTE and those without VTE. Diagnosing subclinical VTE: An ROC analysis of FRMs was performed between patients with subclinical VTE and those without VTE. Excluding VTE: The NPVs were analyzed between patients with subclinical VTE and those without VTE. Predicting postoperative DVT: An ROC analysis of FRMs was performed between patients with postoperative VTE and those without VTE. Evaluating VTE risk: An ROC analysis of FRMs was performed between patients with TH (subclinical or postoperative VTE) and those without VTE.
The data are expressed as median (25th-75th percentiles). Differences between groups were examined for significance using the Mann-Whitney U test. P-values of <.05 were considered to indicate a statistically significant difference. All of the statistical analyses were performed using the Stat-Flex software program (version 6; Artec Co Ltd, Osaka, Japan). In addition, the significance of differences in frequency was examined using the χ2 test and Fisher exact test.
Results
In this study, the plasma levels of FRM were measured in 44 patients with acute VTE and 326 patients undergoing major orthopedic surgery, and the relationships between FRMs including 4 D-dimer kits and DVT were examined. Although 16 patients (median age [range]: 76.5 years [70.0-79.5 years]; females: n = 12; males: n = 4) had no symptoms, distal and chronic DVT existed prior to the surgery. These patients were considered to have “subclinical VTE.” After surgery, a further 67 patients (median age [range]: 73.0 years [67.0-79.5 years]; females: n = 57; males: n = 10) were newly diagnosed with distal DVT (postoperative DVT). These patients were generally treated with 30 mg of edoxaban until 1 day before surgery.
The FDP, D-dimer, and SF levels were measured in frozen plasma from the 326 patients who underwent orthopedic surgery several days before surgery. The plasma levels of FDP, FMC, and D-dimers (A), -(B), -(C), and -(D) in HVs, patients without VTE, those with postoperative VTE, those with subclinical DVT, and those with acute VTE are shown in Table 1. The evaluation of the FRM levels as 4 D-dimer, FMC, and FDP values was significantly higher in patients with acute VTE than in patients with postoperative DVT, those with subclinical DVT, and those without VTE and HVs (Figure 1). Four D-dimer and FDP values were significantly higher in patients with acute VTE, those with postoperative DVT, and those with subclinical DVT than in patients without TH. In contrast, the FMC levels in patients with subclinical DVT were not significantly higher than those in patients without VTE. We also examined whether preoperative data could predict the development of postoperative TH.
The Fibrin-Related Markers in HV, Patients Without VTE, Those With Postoperative DVT, Those With Subclinical DVT, and Those With Acute VTE.
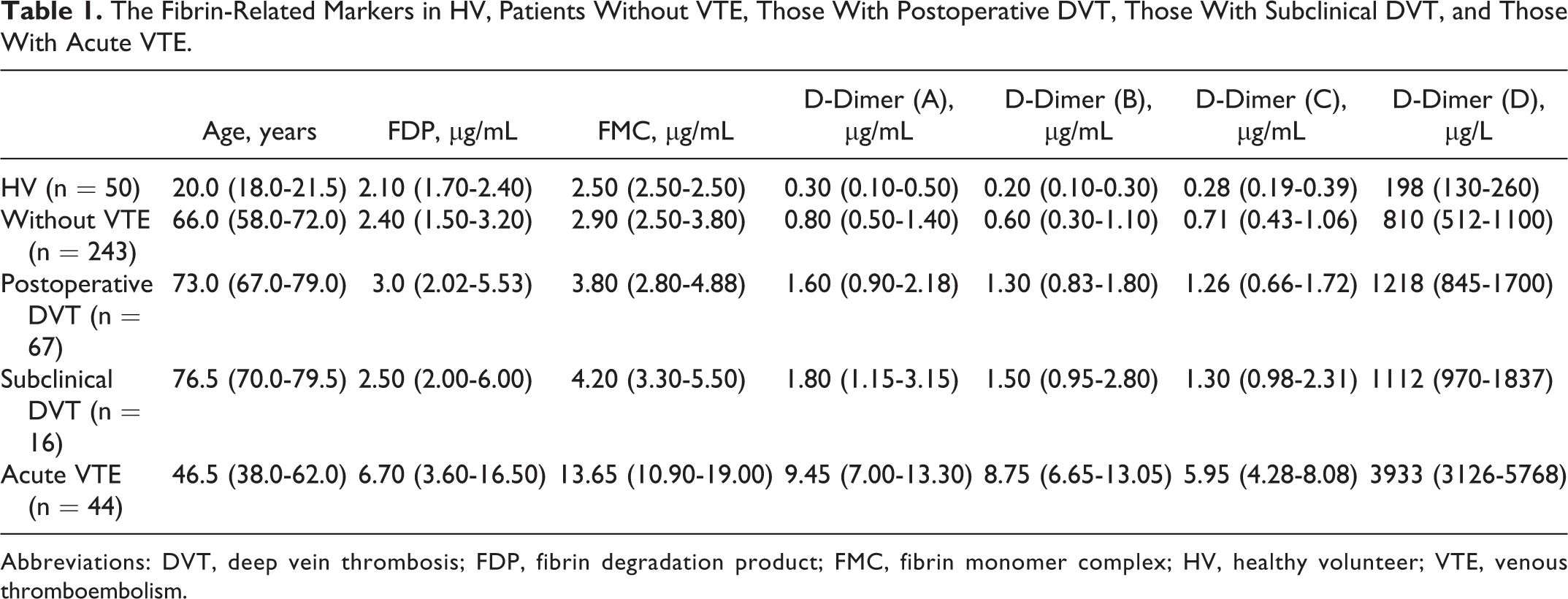
Abbreviations: DVT, deep vein thrombosis; FDP, fibrin degradation product; FMC, fibrin monomer complex; HV, healthy volunteer; VTE, venous thromboembolism.
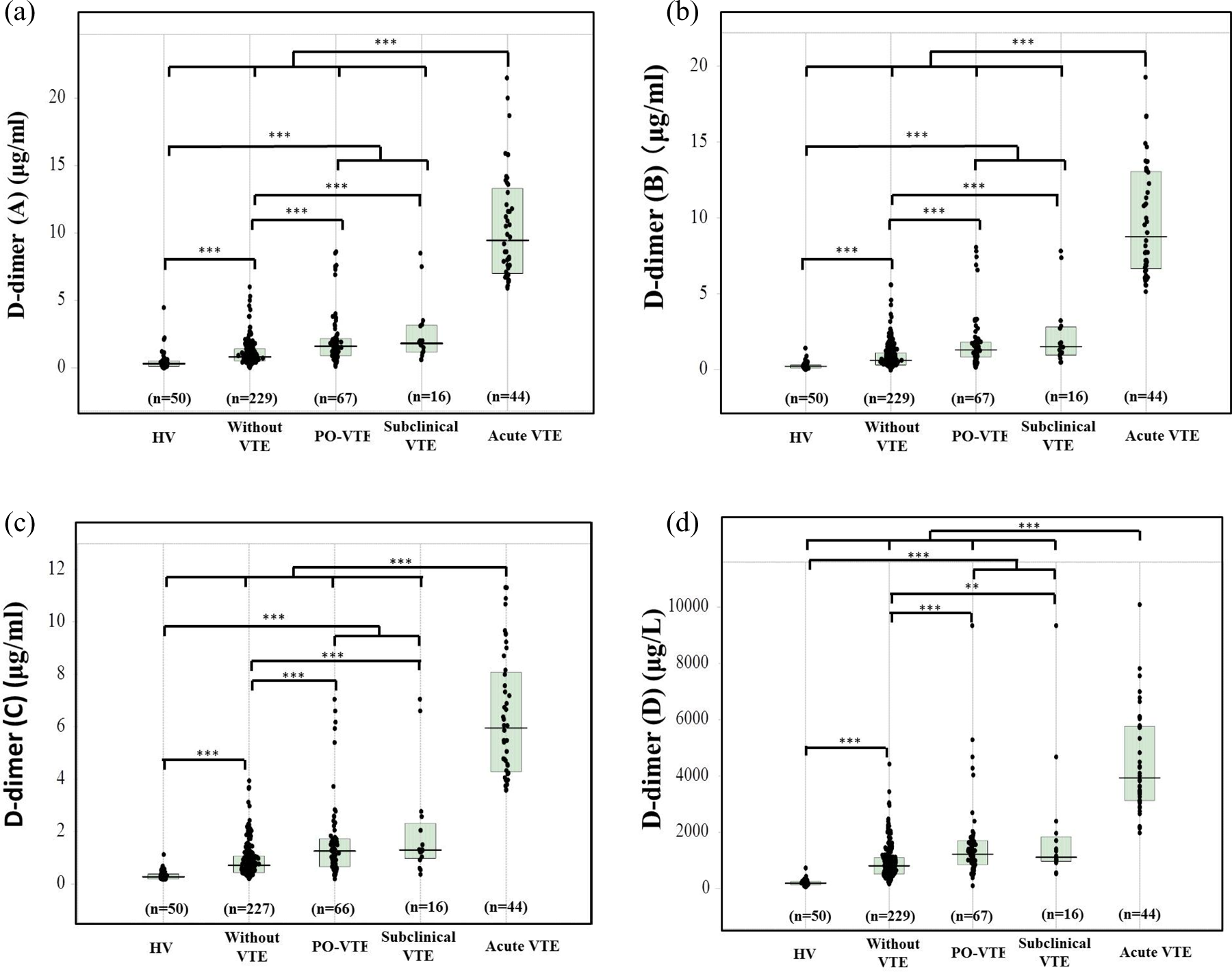
The plasma levels of D-dimers (A; a), (B; b), (C; c), and (D; d) in patients with acute VTE, subclinical VTE, or postoperative VTE and patients undergoing orthopedic surgery without VTE, and HVs. HVs indicates healthy volunteers; PO-TH, postoperative thrombosis; VTE, venous thromboembolism. ***P < .001; **P < .01; *P < .05.
In the ROC analysis for the diagnosis of acute VTE (Table 2), the area under the curve (AUC) values, sensitivity, specificity, and odds ratio of D-dimer assays (A) to (D) and FMC were markedly high, with D-dimer (A) showing the highest values, while the AUC and odds ratio of FDP were not high.
The Diagnosis of Acute VTE.a
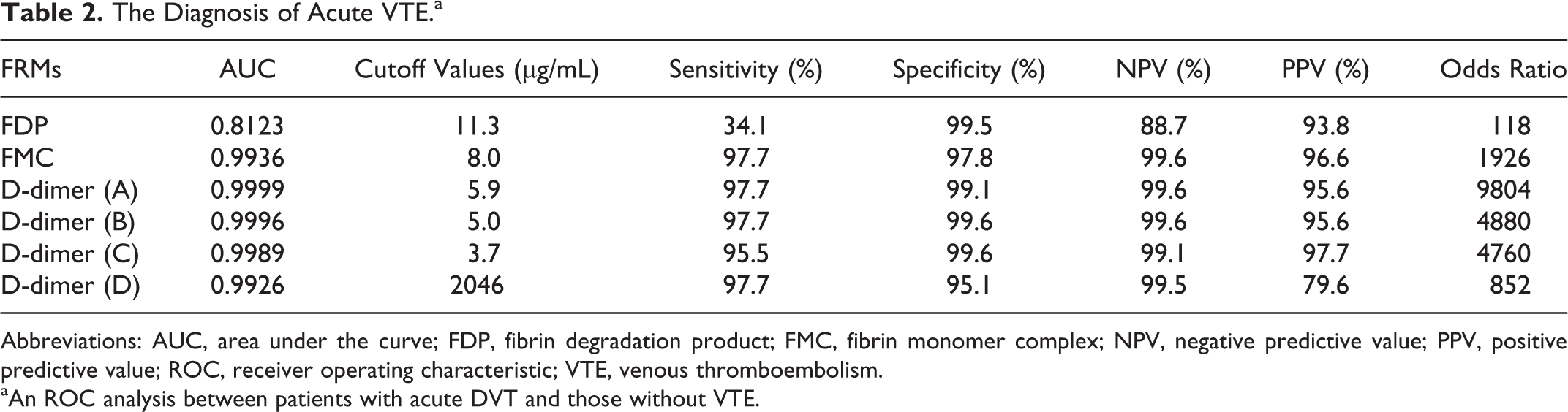
Abbreviations: AUC, area under the curve; FDP, fibrin degradation product; FMC, fibrin monomer complex; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic; VTE, venous thromboembolism.
aAn ROC analysis between patients with acute DVT and those without VTE.
In the ROC analysis for the diagnosis of subclinical DVT (subclinical DVT vs without VTE; Table 3), the lowest AUC and odds ratio were observed in FDP, and the adequate cutoff values and odds ratios among the 4 D-dimer assays were 3.4 to 5.3 μg/mL and 16.2 to 32.6, respectively. These cutoff values of the 4 D-dimers showed low sensitivity but high specificity. In the exclusion of subclinical DVT in these orthopedic patients (Table 4), the 100% of NPVs were as follows: D-dimer (A) 0.5 μg/mL, D-dimers (B) and (C) 0.4 μg/mL, and D-dimer (D) 524 μg/L. The cutoff values for an NPV of >97.5% ranged from 0.6 to 1.8 μg/mL and the odds ratios ranged from 3.3 to 7.4.
The Diagnosis of Subclinical DVT.a
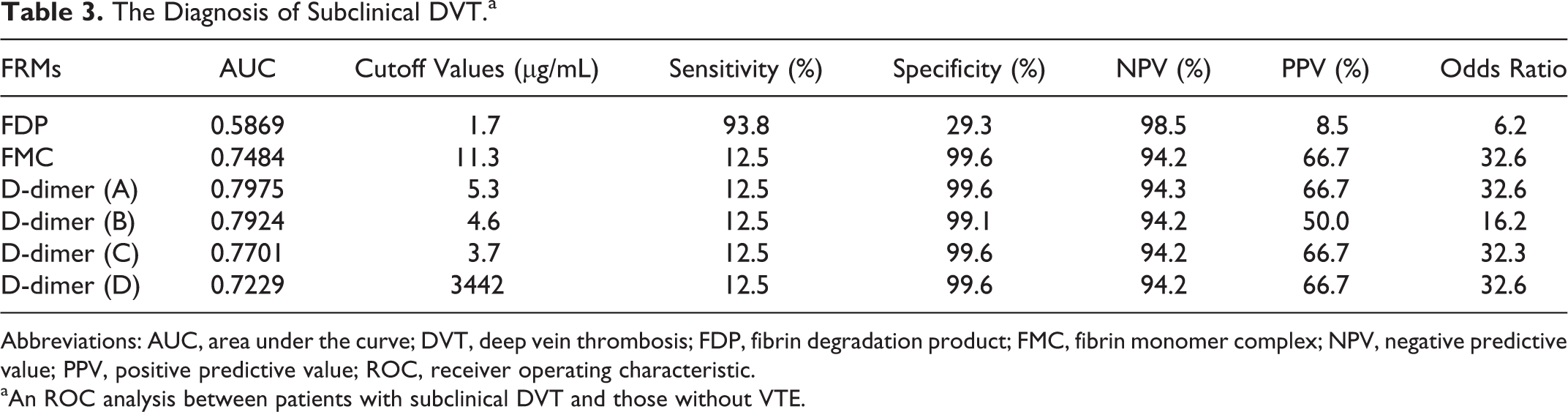
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; FDP, fibrin degradation product; FMC, fibrin monomer complex; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic.
aAn ROC analysis between patients with subclinical DVT and those without VTE.
The Exclusion of Subclinical VTE.a
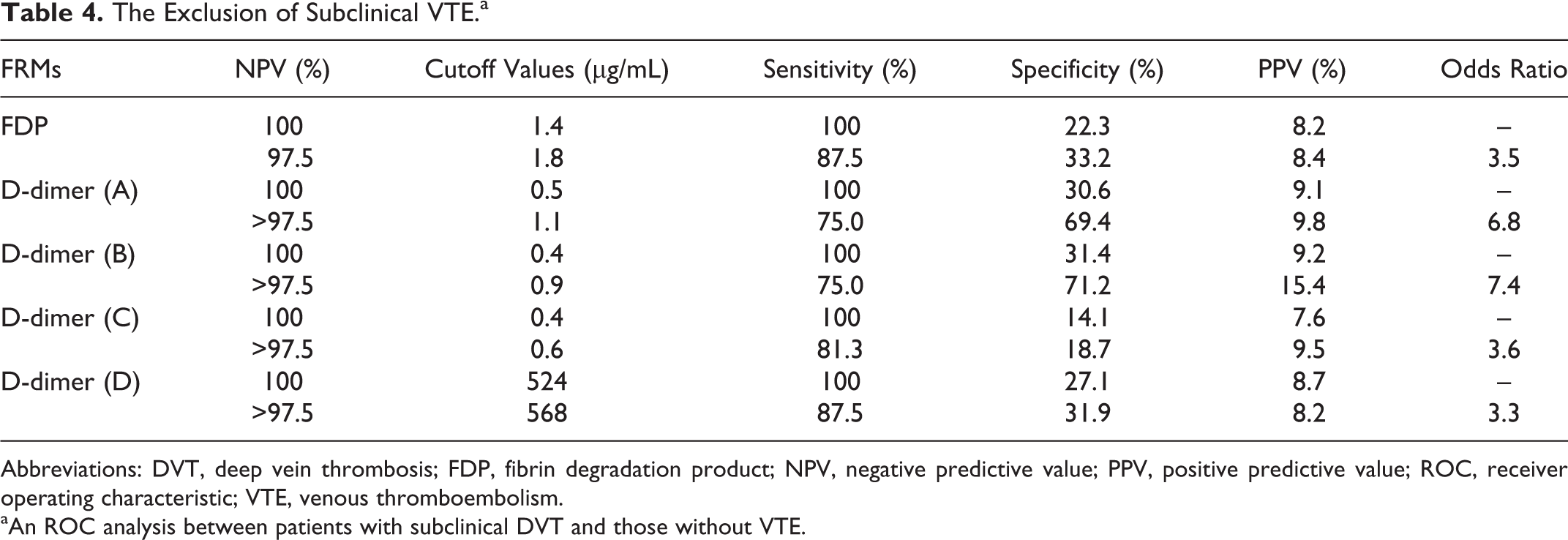
Abbreviations: DVT, deep vein thrombosis; FDP, fibrin degradation product; NPV, negative predictive value; PPV, positive predictive value; ROC, receiver operating characteristic; VTE, venous thromboembolism.
aAn ROC analysis between patients with subclinical DVT and those without VTE.
In the ROC analysis for the prediction of postoperative DVT (postoperative DVT vs without VTE; Table 5), the adequate cutoff values were as follows: FDP 3.3 μg/mL and FMC 11.3 μg/mL, while those in the D-dimer assays were 3.4 to 5.3 μg/mL. The FMC and D-dimers (A), (C), and (D) showed the high odds ratio (>18.5), while FDP showed the lowest odds ratio and AUC value. These cutoff values of FMC and the 4 D-dimers showed low sensitivity but high specificity.
The Prediction of Postoperative DVT.a
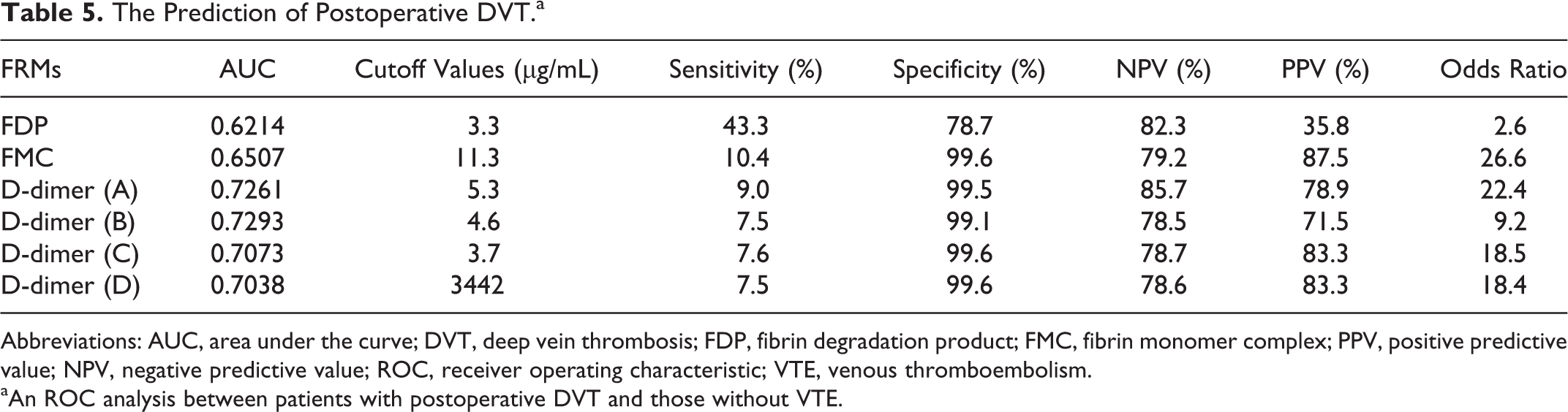
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; FDP, fibrin degradation product; FMC, fibrin monomer complex; PPV, positive predictive value; NPV, negative predictive value; ROC, receiver operating characteristic; VTE, venous thromboembolism.
aAn ROC analysis between patients with postoperative DVT and those without VTE.
In the evaluation of the risk for VTE (subclinical and postoperative DVT vs without VTE; Table 6), adequate cutoff values were as follows: FMC 11.3 μg/mL and D-dimers (A) to (D) 3.4-5.2 μg/mL. The highest odds ratio was 27.7 in FMC, and the lowest odds ratio was 2.5 in FDP. These cutoff values of FRMs showed low sensitivity but high specificity.
The Evaluation of Risk for Subclinical DVT and Postoperative DVT.a
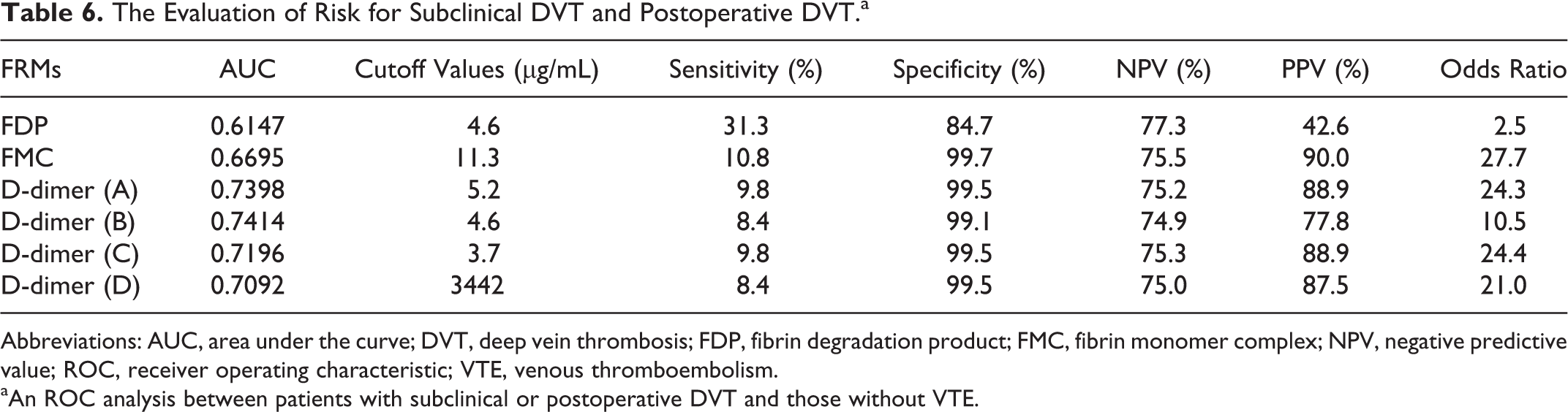
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; FDP, fibrin degradation product; FMC, fibrin monomer complex; NPV, negative predictive value; ROC, receiver operating characteristic; VTE, venous thromboembolism.
aAn ROC analysis between patients with subclinical or postoperative DVT and those without VTE.
The D-dimer (A) values were well correlated with the values of D-dimers (B) and (D) but not with the values of D-dimer (C; Figure 2). The slope was approximately 1 between D-dimers (A) and (B) and 1.5 between D-dimer (A) or (B) and (C) but was approximately 2 between D-dimer (A) or (B) and (D).
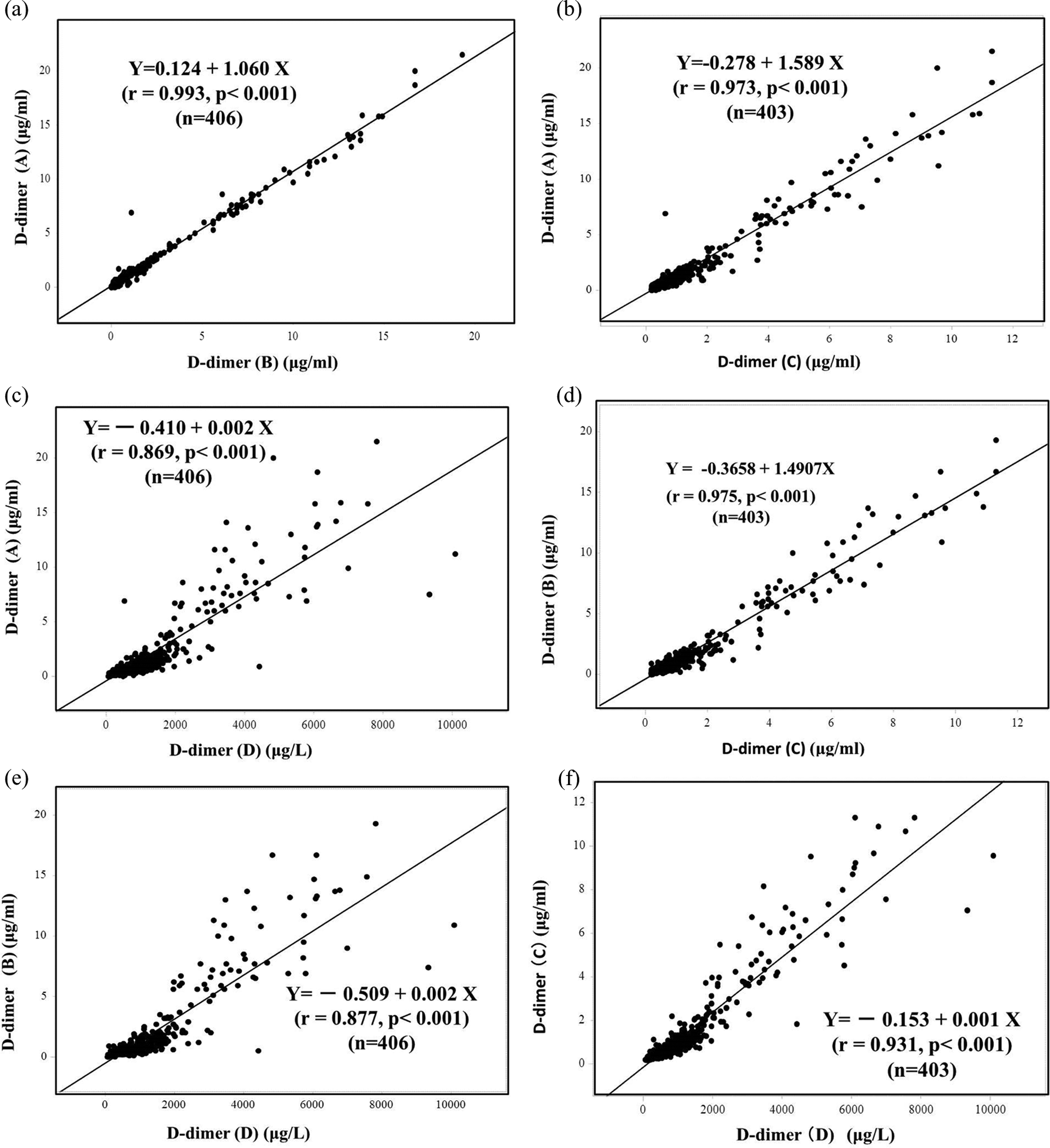
The relationship between (a) D-dimers (A) and (B), (b) D-dimers (A) and (C), (c) D-dimers (A) and (D), (d) D-dimers (B) and (C), (e) D-dimers (B) and (D), and (f) D-dimers (C) and (D). The D-dimer (A) values were well correlated with the values of D-dimers (B) and (D) but not with the values of D-dimer (C).
Discussion
Many reports have investigated the FRMs that are useful for the diagnosis of VTE including acute VTE and the exclusion of VTE. 22,24,25 Our findings suggest that FRMs may be useful for the diagnosis of subclinical VTE and for predicting postoperative VTE. In the diagnosis of acute VTE, the AUC values and odds ratios among FMC and the 4 D-dimer assays were markedly high, while those of FDP were not, suggesting that the half-life of FDP was not long and that it may not be adequate for detecting VTE, since FDP may reflect fibrinogenolysis. There were no differences in the AUC among the 4 D-dimers, but the odds ratio was the highest for D-dimer (A), suggesting that D-dimer (A) is a better marker than D-dimers (B), (C), or (D) for diagnosing patients with high D-dimer levels. These D-dimer (A) and (B) assays are used for diagnosing DIC and VTE in Japan, 26 whereas D-dimers (C) and (D) have been shown to be useful in the exclusion of VTE. 27,28
In the diagnosis of subclinical DVT, we determined different cutoff values for each of the 4 D-dimer assays. Although the odds ratios for FMC and the 4 D-dimers were high, these cutoff values were able to diagnose only 12.5% of subclinical DVT cases. The FDP may therefore not be useful for diagnosing subclinical DVT. The AUC and odds ratio suggest that the diagnosing ability of FRMs is lower for subclinical DVT than acute VTE. In the exclusion of VTE in these orthopedic patients, the 100% NPVs were as follows: D-dimer (A) 0.5 μg/mL, D-dimers (B) and (C) 0.4 μg/mL, and D-dimer (D) 524 μg/L. The cutoff value of D-dimer (D) was similar to that noted in a previous report. 12,27 In D-dimers (A) and (B), the cutoff values of 0.4 to 0.5 μg/mL might be close to the lower end of the detectable range. With an NPV of >97.5%, the cutoff values were from 0.5 to 1.1 μg/mL, suggesting that the levels of D-dimers (A), (B), and (C) were within the measurable range.
The FMC and the 4 D-dimer assays were potentially useful for the prediction of only 7.5% to 10% of postoperative DVT cases, which are considered to be pre-VTE before surgery, and its highest odds ratio suggested that FMC and D-dimer (A) might be the more useful assay. As patients with preoperative D-dimer levels that are higher than the cutoff levels are at risk of developing postoperative VTE, it might be useful to recommend that these patients receive anticoagulants after surgery. The cutoff values of FRMs for diagnosing subclinical DVT were not markedly high and were similar to those for postoperative DVT. In evaluating the risk for VTE (subclinical and postoperative DVT vs without VTE), the adequate cutoff values were as follows: D-dimer (A) 5.2 μg/mL, D-dimer (B) 4.6 μg/mL, D-dimer (C) 3.7 μg/mL, and D-dimer (D) 3442 μg/L. The cutoff values of D-dimer 3.4-5.2 μg/mL for the risk of VTE were similar to those of a previous report. 10 However, these cutoff values detected a risk of VTE in only 8.4% to 9.8% of cases.
Although D-dimer (A) was well correlated with D-dimers (B) and (D), there were various cutoff values and a suitable working range, suggesting that a standardization of D-dimer would be required for the diagnosis, prediction, and exclusion of VTE. 29 This difference in the slope between D-dimers (A) to (C) and D-dimer (D) depends on the unit of reference in D-dimers (A) to (C; fibrin units) and D-dimer (D; fibrinogen units).
In conclusion, increased D-dimer levels were useful for diagnosing subclinical VTE and predicting the risk of VTE in about 10% of patients undergoing orthopedic surgery. However, several different cutoff values for the diagnosis of subclinical VTE or for the prediction of postoperative VTE were identified.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid from the Ministry of Health, Labour and Welfare of Japan for Blood Coagulation Abnormalities and the Ministry of Education, Culture, Sports, Science and Technology of Japan. The FRMs assay systems in this study were provided by Sysmex.