
Abstract
The cutoff values of D-dimer levels for diagnosing or predicting the occurrence of deep vein thrombosis (DVT) were evaluated in preoperative patients and compared to those in non-DVT patients. The levels of 8 different D-dimers were measured using the latex agglutination method or enzyme immunoassay before surgery in 262 orthopedic surgery patients to diagnose subclinical DVT or predict postoperative DVT. There were 15 patients with subclinical DVT and 47 with postoperative DVT, but 200 patients had no DVT at all. All 8 plasma D-dimer values were significantly higher in the patients with subclinical or postoperative DVT than in those without DVT or in healthy volunteers. There were differences in the cutoff values between the assays highly sensitive for low D-dimer levels and wild-range assays of D-dimers. Some D-dimer assays might therefore be more useful than others for diagnosing low levels of D-dimer. Although the measurement of D-dimer levels was useful for diagnosing subclinical DVT and predicting the risk of DVT, the cutoff values for the diagnosis or prediction of DVT varied. The cutoff values for the prediction of postoperative DVT were ≥1.7 µg/mL (D-dimer A-D) and ≥1.0 µg/mL (D-dimer E-H).
Introduction
Pulmonary embolism (PE) 1,2 is a potentially fatal disease and one of the most prevalent cardiovascular diseases; it is usually caused by deep vein thrombosis (DVT). Acute venous thromboembolism (VTE), 3 –5 including DVT and PE, is a serious complication that can occur after orthopedic surgery, including total knee arthroplasty (TKA) and total hip arthroplasty (THA). Orthopedic surgery is reported to be strongly associated with postoperative VTE, 6 –8 and the incidence of DVT after TKA and THA ranges from 41% to 85% and 42% to 57%, respectively, with screening in the absence of thromboprophylaxis. 9 Many studies have established the efficacy of low-molecular-weight heparin, fondaparinux, and direct oral anticoagulants (DOACs) such as anti-Xa and anti-IIa drugs as prophylactic treatments against VTE in patients undergoing orthopedic surgery. 10 –13 Direct oral anticoagulants 13,14 such as rivaroxaban, apixaban, and edoxaban have recently become available for prophylaxis after surgery and for the treatment of VTE. These anticoagulant therapies have significantly reduced the incidence of VTE but may increase the risk of bleeding after orthopedic surgery.
Fibrin-related markers (FRMs) such as D-dimer and soluble fibrin (SF) are considered useful for diagnosing thrombosis such as VTE. 15,16 Although the measurement of the D-dimer and SF levels can be used to predict the incidence of DVT after THA or TKA without anticoagulants, 17 their usage for predicting postoperative VTE is lost following the administration of fondaparinux or edoxaban. 14,18,19 Fibrinogen and fibrin degradation product (FDP) and D-dimer levels can also be used to diagnose disseminated intravascular coagulation (DIC) 20 and VTE, but adequate cutoff values have not yet been established. A D-dimer assay is used as an initial screening test in the emergency department to exclude a PE in Europe and North America. 21 The purpose of this test, which has a high negative predictive value (NPV), is to provide a fast and cost-effective way to triage patients with suspected PE for imaging tests. 22,23 It was recently reported that mild elevation of the D-dimer level suggested risks of subclinical and postoperative VTE. 14 In addition, elevated D-dimer levels have also been reported to suggest massive bleeding. 19
The objective of this study was to determine and compare the adequate cutoff levels of D-dimer kits to fibrin or fibrinogen units for diagnosing subclinical VTE and predicting postoperative VTE before surgery and to examine the relationships among the results of various D-dimer kits.
Materials and Methods
A total of 262 patients undergoing major orthopedic surgery (184 THA and 78 TKA; median age [25th-75th percentile], 67.0 years [60.0-74.0 years]; females, n = 213; males n = 49) who were treated with 30 mg of edoxaban (Daiichisankyo, Tokyo, Japan) and intermittent pneumatic compression for prophylaxis against DVT between January 1, 2013, and April 30, 2016, at Mie University Hospital were enrolled in this single-center study. Patients with a high bleeding risk, defined as a decrease of more than 2 g/dL in the hemoglobin, were excluded from the analysis. 18,19 All of the patients in the cohort received 30 mg of edoxaban once per day for 14 days beginning at least 12 hours after surgery. The findings from 50 healthy volunteers (HVs; median age, 20.0 years [18.0-21.5 years], female n = 24; male, n = 26) were compared to those of patients undergoing orthopedic surgery. We defined those with acute DVT as symptomatic DVT, whereas those with subclinical DVT had no symptoms in the present study. The presence of DVT in the patients who underwent orthopedic surgery was assessed by a whole-leg compression ultrasound examination using the standardized ultrasound criteria for venous noncompressibility before surgery and on days 4 and 14. 18,19 The study protocol was approved by the Human Ethics Review Committee of Mie University School of Medicine, and signed informed consent was obtained from each participant. This study was carried out in accordance with the principles of the Declaration of Helsinki.
The plasma D-dimer levels were measured in samples obtained before surgery and frozen at −80°. The D-dimer levels were determined via the latex agglutination method or enzyme immunoassay using HemosIL D-Dimer HS 2000 (Instrumentation Laboratory, Bedford, Massachusetts; D-dimer A), LPIA-ACE D-Dimer II (LSI Medience Corporation, Tokyo, Japan; D-dimer B), LIASAUTO D-dimer Neo (Sysmex, Kobe, Japan; D-dimer C), Nanopia D-dimer (Sekisui Medical, Tokyo, Japan; D-dimer D), HemosIL D-Dimer HS 500 (Instrumentation Laboratory; D-dimer E), HemosIL AcuStar D-Dimer (Instrumentation Laboratory; D-dimer F), INNOVANCE D-Dimer (SIEMENS, Marburg, Germany; D-dimer G), and VIDAS D-Dimer Exclusion II (bioMerieux, Marcy l’Etoile, France; D-dimer H). D-dimers A-D used fibrin units and assayed the wild range, whereas, D-dimers E-H used fibrinogen units and were highly sensitive for low levels of D-dimer.
Statistical Analyses
The cutoff values of D-dimer for predicting postoperative DVT, diagnosing subclinical DVT, and excluding DVT were analyzed, and the DVT risk was evaluated. Predicting postoperative DVT: A receiver operating characteristic (ROC) analysis of D-dimer was performed between patients with postoperative VTE and those without VTE or HVs. Diagnosing subclinical VTE: An ROC analysis of D-dimer was performed between patients with subclinical VTE and those without VTE or HVs. Evaluating DVT risk: An ROC analysis of D-dimer was performed between patients with DVT (subclinical or postoperative VTE) and those without VTE or HVs.
The data are expressed as the median (25th-75th percentiles). Differences between groups were examined for significance using the Mann-Whitney U test. P values of less than .05 were considered to indicate a statistically significant difference. All of the statistical analyses were performed using the Stat-Flex software program (version 6; Artec Co Ltd, Osaka, Japan).
Results
Although 15 patients had no symptoms, distal and chronic DVT existed prior to surgery. These patients were considered to have “subclinical DVT” and were generally treated with 30 mg of edoxaban until 1 day before surgery. After surgery, a further 47 patients were newly diagnosed with distal DVT (postoperative DVT). A total of 200 patients who did not have either subclinical or postoperative DVT were defined as “patients without DVT.”
The plasma levels of D-dimers A-H in the HVs and in the patients without DVT, with postoperative DVT and with subclinical DVT are shown in Table 1. All plasma D-dimer A-H values were significantly higher (P < .001) in the patients with subclinical or postoperative DVT than in those without DVT or in the HVs (Figure 1).
Plasma D-Dimer Levels in Healthy Volunteers, the Patients Without DVT, Those With Postoperative DVT, or Those With Subclinical DVT.
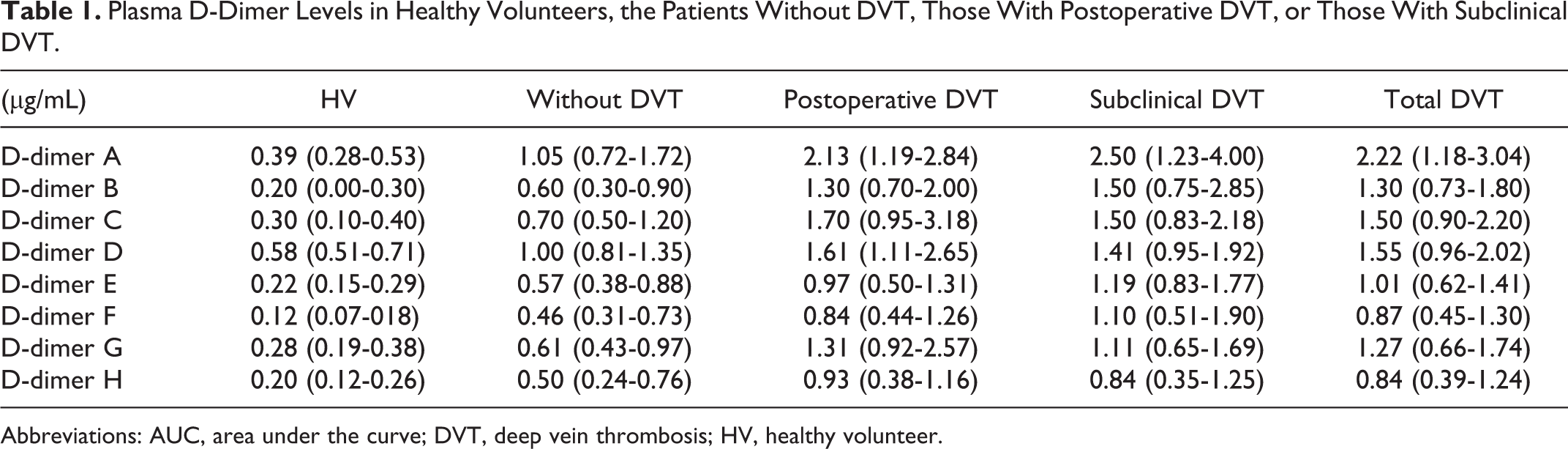
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; HV, healthy volunteer.
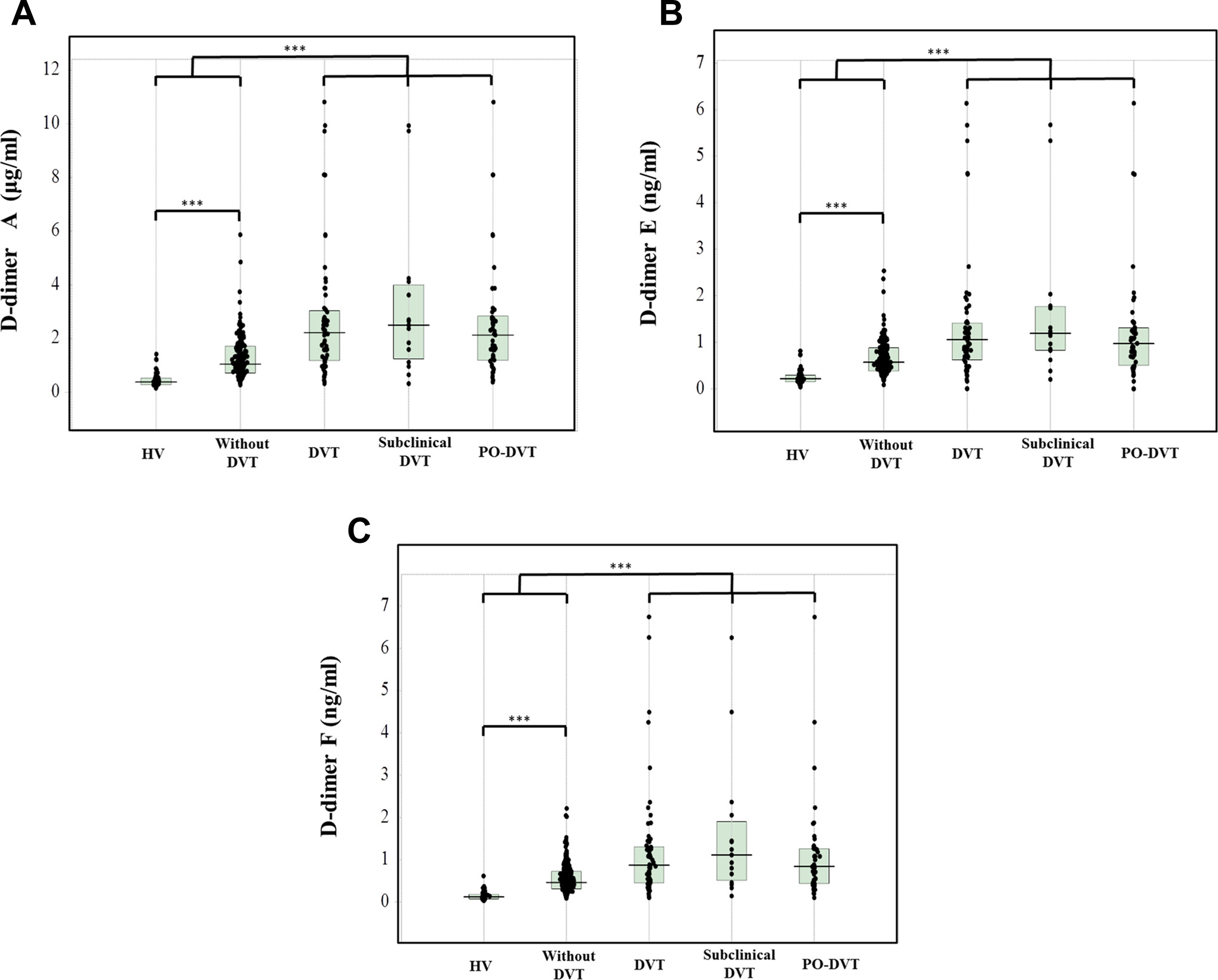
The plasma levels of D-dimer A (A), D-dimer E (B), and D-dimer F (C) in the patients with subclinical DVT or postoperative DVT and orthopedic surgery patients without DVT and healthy volunteers. DVT indicates deep vein thrombosis; HVs, healthy volunteers; PO-DVT, postoperative DVT. ***P < .001
Lower cutoff values with similar values for sensitivity and specificity were examined using ROC analyses, and higher cutoff values with positive predictive value (PPV) close to 50% were also examined.
In the ROC analysis for the prediction of postoperative DVT (patients with postoperative DVT vs patients without VTE and HVs; Table 2), there were no significant differences in the area under the curve (AUC) among D-dimers A-H. The lower cutoff values ranged from 0.70 to 1.32 µg/mL in D-dimers A-D and from 0.53 to 0.88 µg/mL in D-dimer E-H. The higher cutoff values ranged from 1.70 to 2.24 µg/mL in D-dimers A-D and from 1.00 to 1.32 µg/mL in D-dimers E-H. The odds ratios ranged from 3.88 to 10.41 among D-dimers A-H.
Prediction of Postoperative DVT Versus Healthy Volunteers and Patients Without DVT.
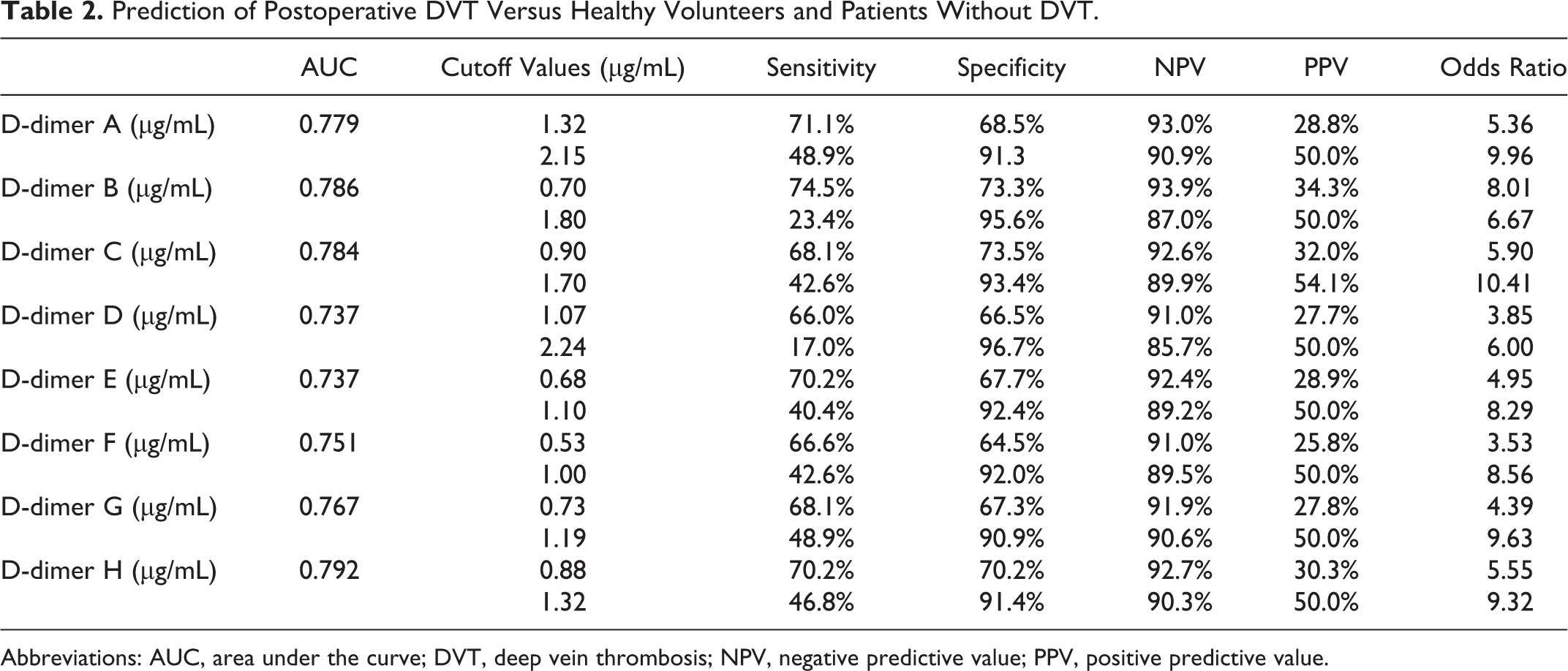
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; NPV, negative predictive value; PPV, positive predictive value.
In the ROC analysis for the diagnosis of subclinical DVT (patients with subclinical DVT vs patients without VTE and HVs; Table 3), the AUCs ranged from 0.776 to 0.899 among D-dimers A-H and were the highest for D-dimer F. The lower cutoff values ranged from 0.70 to 1.45 µg/mL in D-dimers A-D and from 0.63 to 0.92 µg/mL in D-dimers E-H. The higher cutoff values ranged from 2.10 to 2.53 µg/mL in D-dimers A-D and from 1.26 to 2.22 µg/mL in D-dimers E-H. The odds ratios ranged from 7.55 to 42.17 among D-dimers A-H.
Diagnosis of Subclinical DVT Versus Healthy Volunteers and Patients Without DVT.
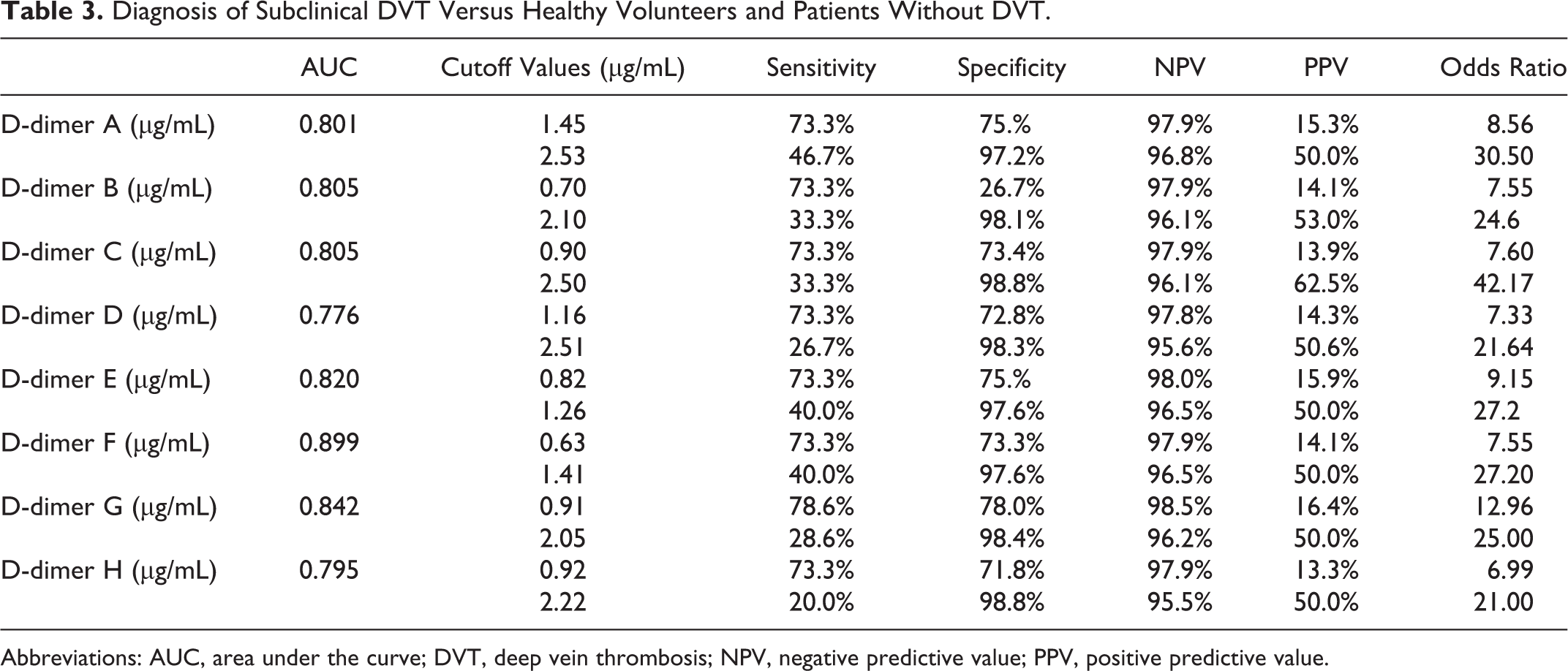
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; NPV, negative predictive value; PPV, positive predictive value.
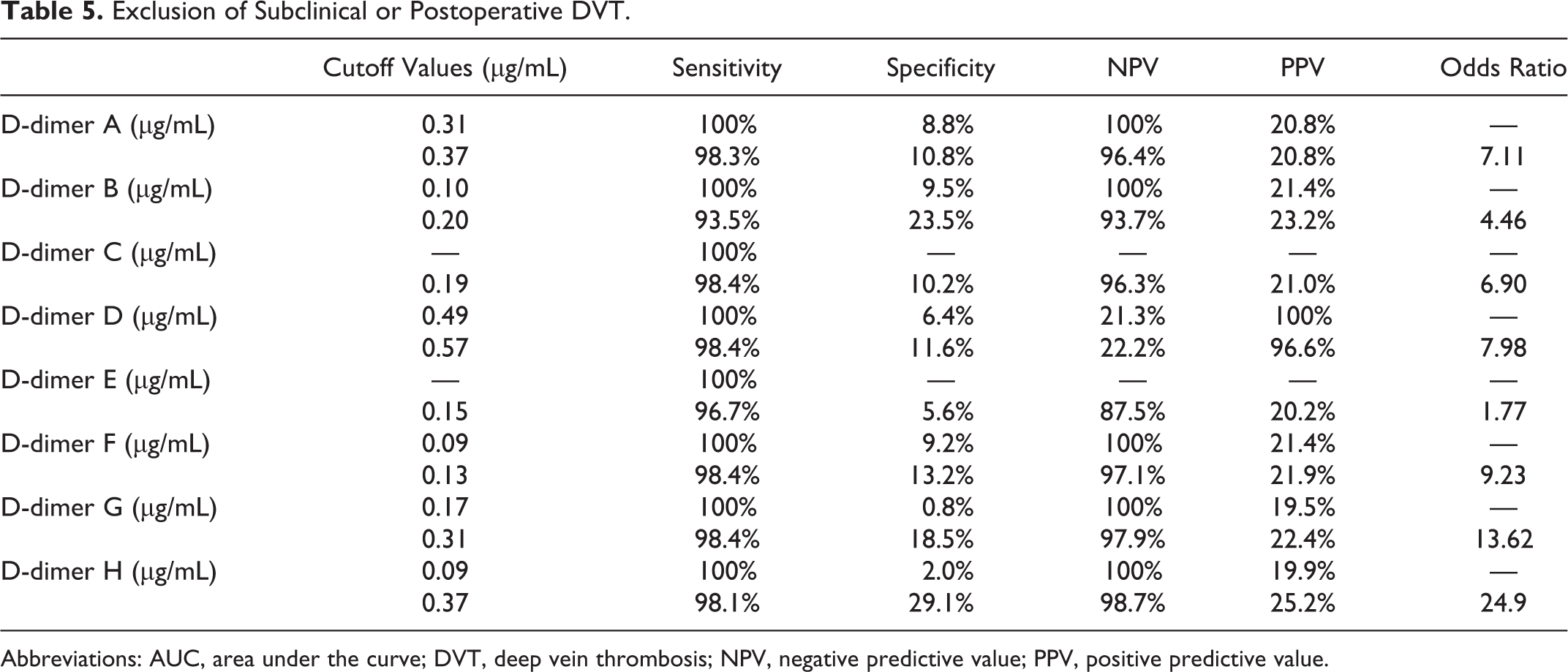
In the evaluation of the risk for DVT (patients with subclinical and postoperative DVT vs patients without DVT; Table 4), there were no significant differences in the AUC among D-dimers A-H. The lower cutoff values ranged from 0.70 to 1.37 µg/mL in D-dimers A-D and from 0.55 to 0.91 µg/mL in D dimers E-H. The higher cutoff values ranged from 1.30 to 2.02 µg/mL in D-dimers A-D and from 0.90 to 1. µg/mL in D-dimers E-H. The odds ratios ranged from 4.1 to 8.43 among D-dimers A-H. The cutoff values for the exclusion of DVT (Table 5) ranged from 0.10 to 0.57 µg/mL in D-dimers A-D and from 0.09 to 0.37 µg/mL l in D-dimers E-H. The odds ratio was the highest for D-dimer H (0.37 µg/mL and 24.9).
Diagnosis of Subclinical or Post-DVT versus Healthy Volunteers and Patients Without DVT.
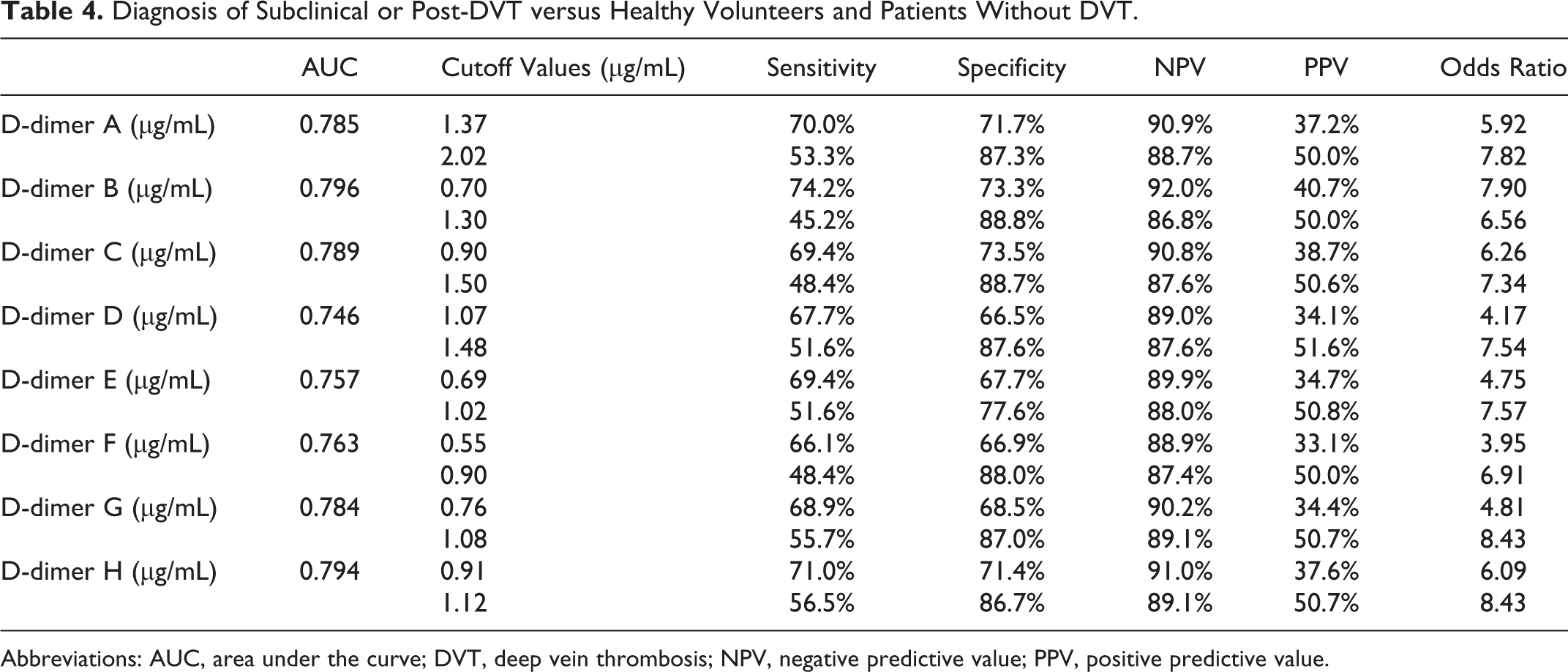
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; NPV, negative predictive value; PPV, positive predictive value.
Exclusion of Subclinical or Postoperative DVT.
Abbreviations: AUC, area under the curve; DVT, deep vein thrombosis; NPV, negative predictive value; PPV, positive predictive value.
D-dimers A and B were well correlated with D-dimers C, D, E, and G, and D-dimer E was well correlated with D-dimers A-G, but D-dimer H was not well correlated with the other D-dimers (Table 6 and Figure 2). The correlation slope between any 2 D-dimer assays varied from 0.772 to 1.878.
Slope and Correlation Between Different D-Dimer Assays.
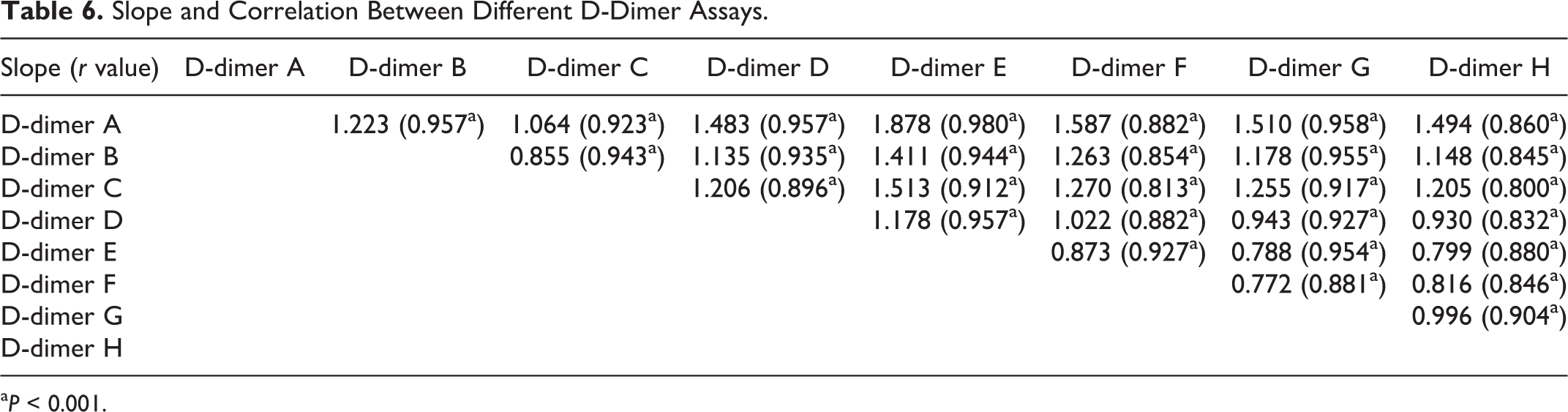
a P < 0.001.
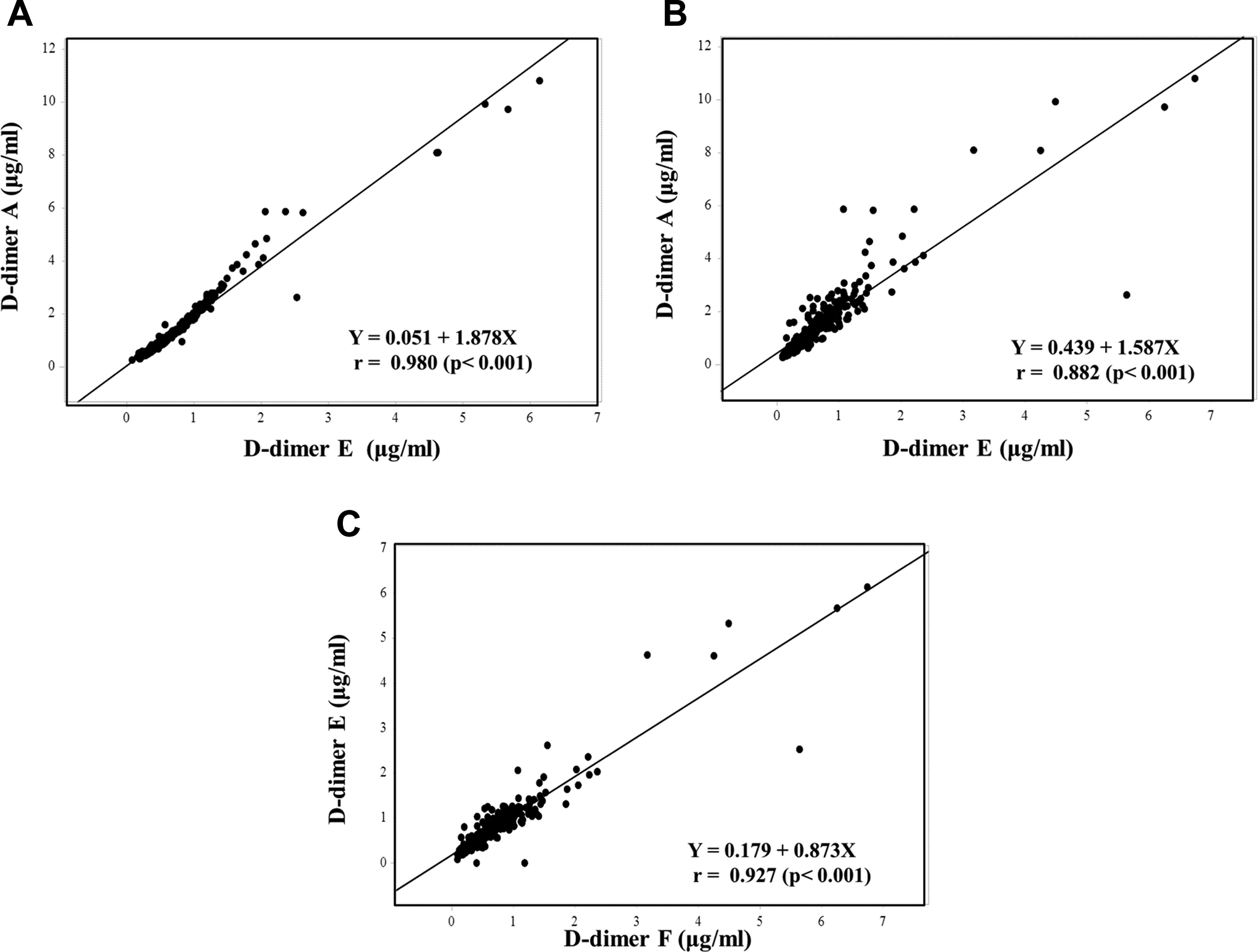
The relationship (A) between D-dimers A and E, (B) between D-dimers A and F, (C) between D-dimers E and F.
Discussion
Many reports have investigated D-dimers that are useful for the diagnosis of DVT, including acute DVT, and the exclusion of DVT. 18,24,25 Our findings suggest that D-dimers may be useful for the diagnosis of subclinical DVT, for predicting postoperative DVT and for the exclusion of DVT. The D-dimer assays were divided 2 groups: 1 group (D-dimers A-D) used fibrin units and a wild range, and the other (D-dimers E-H) used fibrinogen units and had high sensitivity for low D-dimer levels. Indeed, the plasma D-dimer A-D levels were higher than the plasma D-dimer E-H levels. D-dimer B and D assays are used for diagnosing DIC and VTE in Japan, 26 and D-dimers G and H have been shown to be useful in the exclusion of VTE. 27,28 However, the plasma D-dimer levels varied among D-dimers A-D and among D-dimers E-H, indicating the need for the standardization of D-dimers. 29
Increased D-dimer levels are reportedly useful for the diagnosis of DVT. 16,17 Plasma D-dimer A-H levels were also significantly high in the patients with subclinical DVT, suggesting that increased D-dimer levels may indicate subclinical DVT. In the diagnosis of subclinical DVT, we determined different cutoff values for each of the 8 D-dimer assays. Lower cutoff values were sensitive for more than 73% of subclinical DVT cases, but the odds ratios ranged from 7.5 to 12.6. Higher cutoff values were sensitive for 20% to 46.7% of subclinical DVT cases and the odds ratios ranged from 21.7-42.2. There were no marked differences in the usefulness between D-dimers A-D (wild-range D-dimers) and D-dimers E-H (highly sensitive for low D-dimer levels).
Plasma D-dimer A-H levels were also high in patients with postoperative DVT, suggesting that increased D-dimer levels may predict postoperative DVT. The 8 D-dimer assays were potentially useful for the prediction of postoperative DVT, which is considered to be pre-VTE before surgery. The AUC and odds ratio for predicting postoperative DVT were lower than those for diagnosing subclinical DVT. These findings show that increased D-dimer levels indicate a hypercoagulable state and an increased risk of thrombosis. These cutoff values were similar to those noted in a previous report. 14 Increased SF may be useful for the prediction of DVT. 14 As patients with preoperative D-dimer levels that are higher than the cutoff levels are at risk of developing postoperative VTE, it might be useful to recommend that these patients receive anticoagulants after surgery.
In the exclusion of subclinical or postoperative DVT in these orthopedic patients, the cutoff values for 100% sensitivity were very low, and those for approximately 97.5% sensitivity were also low. The cutoff value of D-dimer H was different from that noted in a previous report. 14,22,27 As such, the exclusion of subclinical or postoperative DVT using D-dimers is difficult.
Although D-dimers A and B were well correlated with D-dimers C, D, E, and G, they were not correlated with D-dimers F and H. The slope of correlation varied between the 2 groups of D-dimer assays. The cutoff values and suitable working range varied among the 8 D-dimer assays, suggesting that the standardization of D-dimer would be required before its effective application in the diagnosis, prediction, and exclusion of DVT. 29 These differences in the slope of correlation among D-dimers A-H, cutoff values, and odds ratios depended not only on the unit of reference but also on the epitope of the D-dimer or the reagents used.
In conclusion, increased D-dimer levels were useful for diagnosing subclinical VTE and predicting the risk of DVT. However, several different cutoff values for the diagnosis of subclinical DVT or for the prediction of postoperative DVT, or exclusion of DVT were identified. Cutoff values of ≥1.7 µg/mL (D-dimer A-D) and ≥1.0 µg/mL (D-dimer E-H) were deemed useful for the prediction of postoperative DVT, whereas values of ≥2.1 µg/mL (D-dimer A-D) and ≥1.2 µg/mL (D-dimer E-H) were deemed useful for the diagnosis of subclinical DVT.
Footnotes
Authors' Note
K. Hasegawa, Y. Yamasita, and K. Nakatani assayed plasma D-dimer levels; T. Yamaguchi, H. Wakabayashi, M. Hasegawa, and A. Sudo managed the patients; T. Matsumoto and N. Katayama analyzed the data; N. Fujimoto, N. Yamada, and M. Ito diagnosed VTE; and H. Wada wrote the manuscript in accordance with the above analysis. All members discussed this manuscript. The D-dimer assay systems used in this study were provided by Sekisui Medical, Sysmex and Instrumentation Laboratory.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by a Grant-in-Aid from the Ministry of Health, Labour and Welfare of Japan for Blood Coagulation Abnormalities and the Ministry of Education, Culture, Sports, Science and Technology of Japan.