
Abstract
Introduction
Thrombosis is a major complication of COVID-19. D-dimer (DD) is an important coagulation fibrinolysis marker in COVID-19 and has been extensively studied. However, very little is known about the role of other fibrinolysis markers, plasmin-plasmin inhibitor complex (PIC), and fibrin monomer complex (FMC) in COVID-19. This study investigated and compared the associations of DD, PIC, and FMC with COVID-19 severity.
Methods
Archived plasma samples from patients with COVID-19 (n = 50) were assessed for DD, FMC, and PIC levels. We compared the levels between patients with mild (n = 36) and moderate (n = 14) COVID-19 and evaluated their correlation with other COVID-19 severity markers, including lactate dehydrogenase (LD), serum albumin (Alb), C-reactive protein (CRP), and neutrophil-lymphocyte ratio (NLR).
Results
Patients with moderate COVID-19 had significantly higher DD and PIC levels than those with mild disease, while FMC levels were comparable. DD and PIC levels significantly correlated with LD, Alb, and NLR. Additionally, PIC levels significantly correlated with CRP levels. However, FMC levels correlated only with Alb but not with LD, NLR, or CRP.
Conclusions
COVID-19 severity was significantly associated with PIC and DD levels but not with FMC levels. PIC was the variable with the most clearly significant difference between patients with moderate disease and those with mild disease, highlighting its potential as an indicator of coagulation and fibrinolysis imbalance in patients with COVID-19. Further studies with larger sample sizes and more diverse severity groups are required to confirm these findings.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) causes COVID-19, which is a global pandemic. Initially, only acute respiratory failure associated with airway infection was considered in COVID-19; however, thrombosis soon became the focus of attention because of the high incidence of thrombotic complications. The overall estimated pooled incidence of venous thromboembolism (VTE) was 17.0% among hospitalized patients with COVID-19. 1 VTE increases the risk of death in patients with COVID-19 by several times. 2
In COVID-19, coagulation factor VIII and von Willebrand factor are released from vascular endothelial cells damaged by viral infection, thereby activating the coagulation system and platelet aggregation.3–5 There have been several reports on the significance of D-dimer (DD) in COVID-19.6–10 DD assays are commonly used in clinical practice to exclude a diagnosis of deep vein thrombosis or pulmonary embolism, and elevated DD indicates increased risk of abnormal blood clotting. High DD levels predict disease severity, pulmonary complications, and thromboembolic events. 11 Patients with DD levels >1 μg/ml present a 20-fold higher mortality risk than those with lower DD levels. 10 While DD is a very good marker for evaluating thrombophilic conditions in COVID-19, it alone cannot determine the degree of coagulation and fibrinolytic activation because DD appears in the blood as a result of coagulation activation and clot breakdown. In addition, DD levels are elevated by various factors. 12
Plasmin-plasmin inhibitor complex (PIC) and fibrin monomer complex (FMC) are other important markers of coagulation and fibrinolysis. However, there are only a few reports on their significance in COVID-19. This study aimed to investigate the association of DD, FMC, and PIC with COVID-19 severity.
Materials and Methods
Patients and Clinical Samples
This research involved 50 patients diagnosed with COVID-19 who were admitted to the Infectious Disease Unit at Tottori University Hospital in Japan between March 2022 and August 2022. We classified the symptoms into mild and moderate based on the Japanese Ministry of “Health, Labor” and Welfare guidelines. Blood samples were collected using standard venipuncture blood collection tubes containing one-tenth volume of sodium citrate (3.2%/0.109 M) to achieve a final citrate concentration of 0.32%/0.0109 M. Platelet-poor plasma was obtained by centrifuging the citrated whole blood for 15 min at 1500 g. Plasma samples were stored at −80 °C and thawed at 37 °C immediately before the assays. All samples were analyzed within one month. The study received approval from the Ethics Committee of Tottori University Faculty of Medicine (approval number: 19A056). Informed consent was obtained through an opt-out approach.
Measurement of Coagulation/Fibrinolysis Markers
The FMC levels were quantified using a latex immunoturbidimetry assay (LIA) with the Auto LIA FM Kit (Nissui Pharmaceutical Co., Ltd, Tokyo, Japan). In this method, the sample reacts with latex particles coated with anti-fibrin monomer antibodies, leading to the aggregation of FMC complexes. The resulting turbidity is directly proportional to the FMC concentration in the sample, allowing for optical measurement of FMC levels. Additionally, levels of DD and PIC were also measured using LIA. All measurements were carried out using a CN-6000 instrument.
Statistical Analysis
We performed all analyses using the EZR software (ver. 1.54; Saitama Medical Center, Jichi Medical University, Saitama, Japan) and a Japanese user interface for R (ver. 4.0.3, The R Foundation for Statistical Computing, Vienna, Austria). 13 Differences between coagulation and fibrinolysis markers were compared using the Mann-Whitney U test. To explore the relationship between coagulation markers and COVID-19 severity markers, we calculated Spearman's correlation coefficient.
Results
The median age of the 50 enrolled patients was 73 years, while that of patients with mild and moderate disease was 57 and 79 years, respectively (p = 0.008). Table 1 lists other clinical characteristics of the study population. Age > 65 years, male sex, and respiratory diseases were significantly more common in patients with moderate disease than in those with mild disease.
Clinical Characteristics of the Patients.
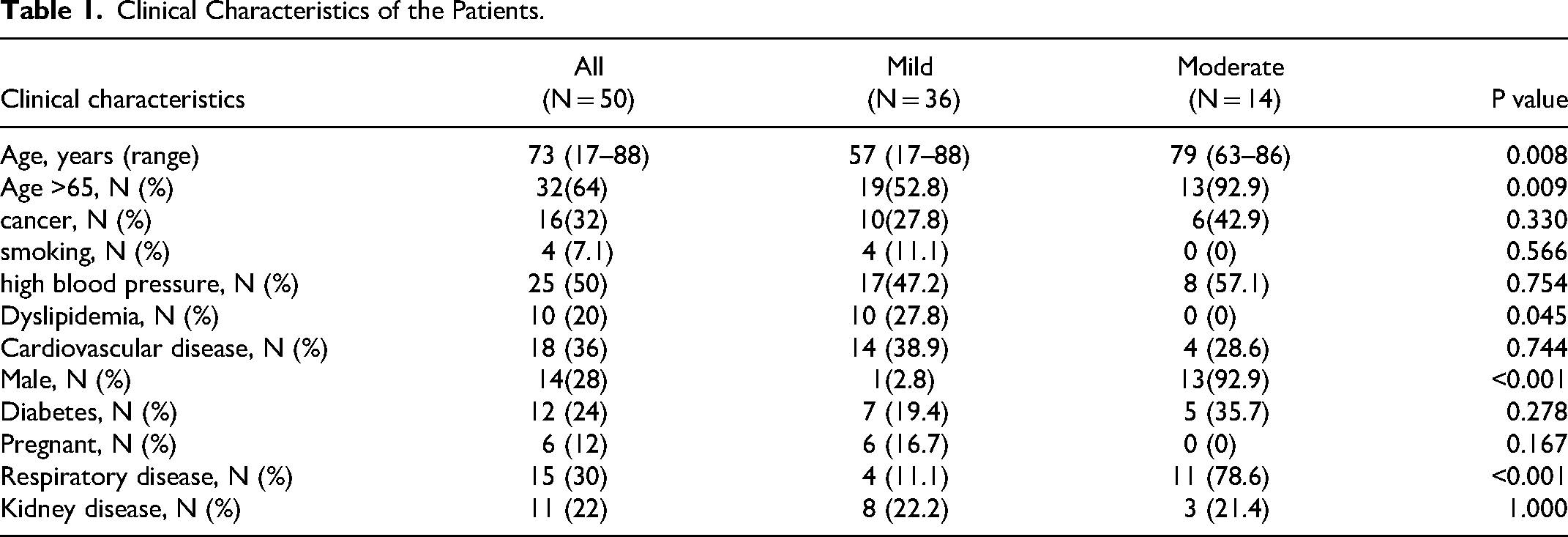
Figure 1 shows the distribution of FMC, DD, and PIC levels. The median (range) FMC, DD, and PIC levels were 2.4 (0.6-120.4) μg/mL, 1.8 (0.5-25) μg/mL, and 1.1 (0.1-5.21) μg/mL, respectively. DD and PIC levels were significantly higher in the moderate disease group than in the mild disease group, while FMC levels were comparable. (FMC: 2.3 vs 2.6 μg/mL, P = 0.374; DD: 1.2 vs 2.3 μg/mL, P = 0.022; and PIC: 0.8 vs 1.4 μg/mL, P = 0.001)(Figure 2).
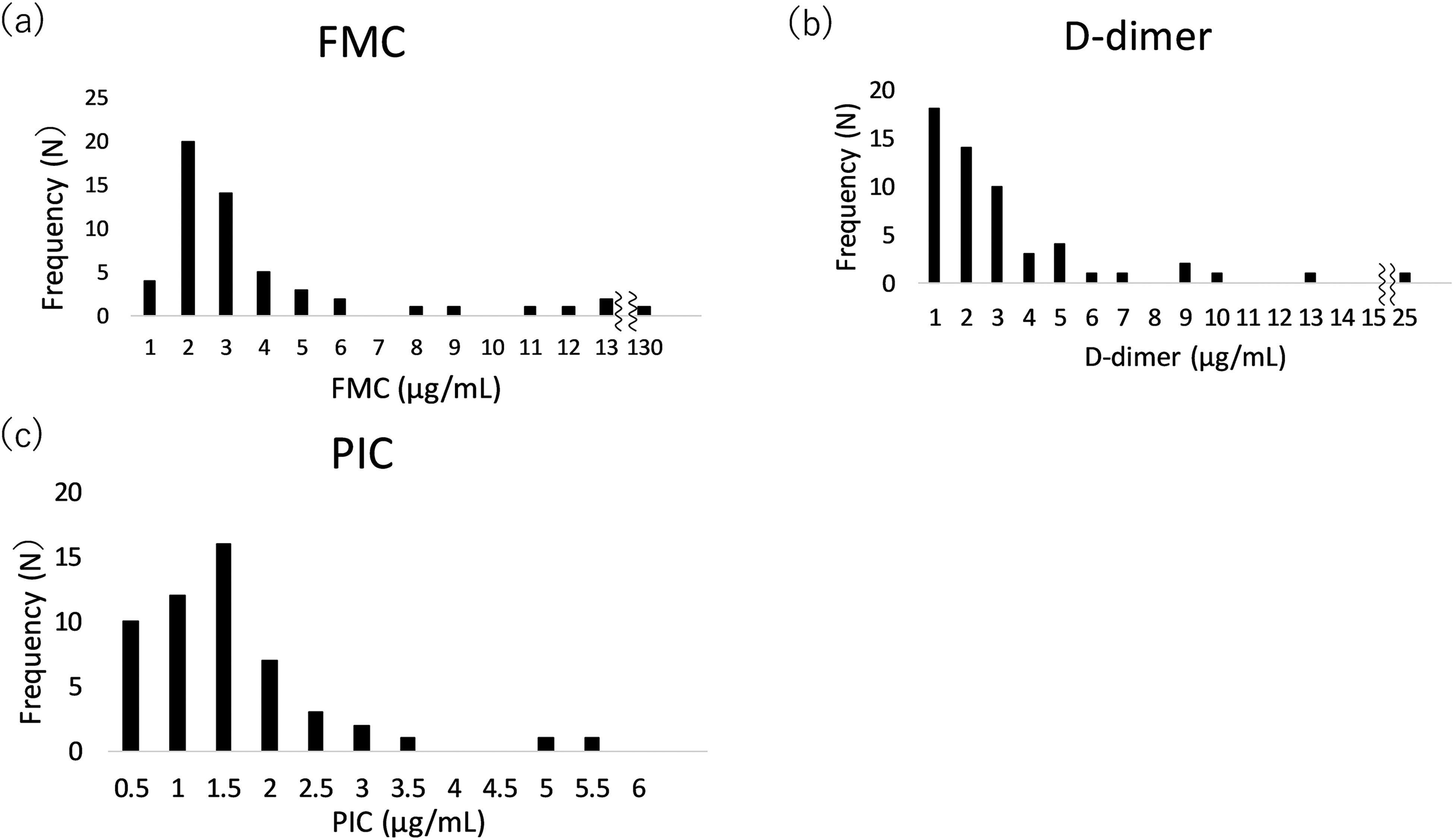
Distribution of FMC, DD, and PIC levels in patients with COVID-19. Each bar represents the frequency of people within a certain range of FMC,
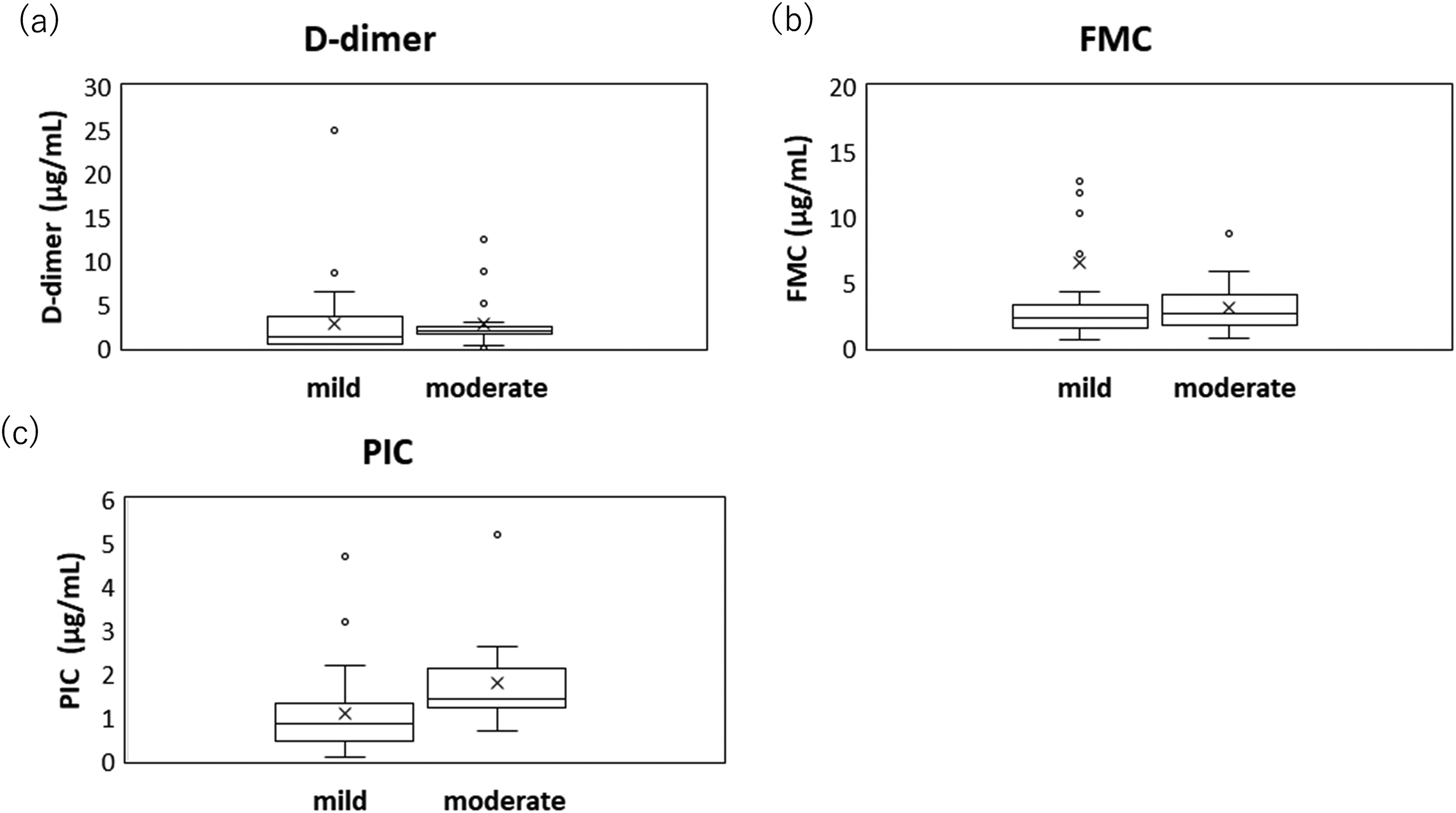
Comparison of coagulation markers in patients with mild versus moderate COVID-19. Each box represents percentile (25th–75th), while the upper and lower whiskers indicate the maximum and the minimum value, respectively.(a) DD: 1.2 versus 2.3 μg/mL, P = 0.022; (b) FMC: 2.3 versus 2.6 μg/mL, P = 0.374; and (c) PIC: 0.8 versus 1.4 μg/mL, P = 0.001.
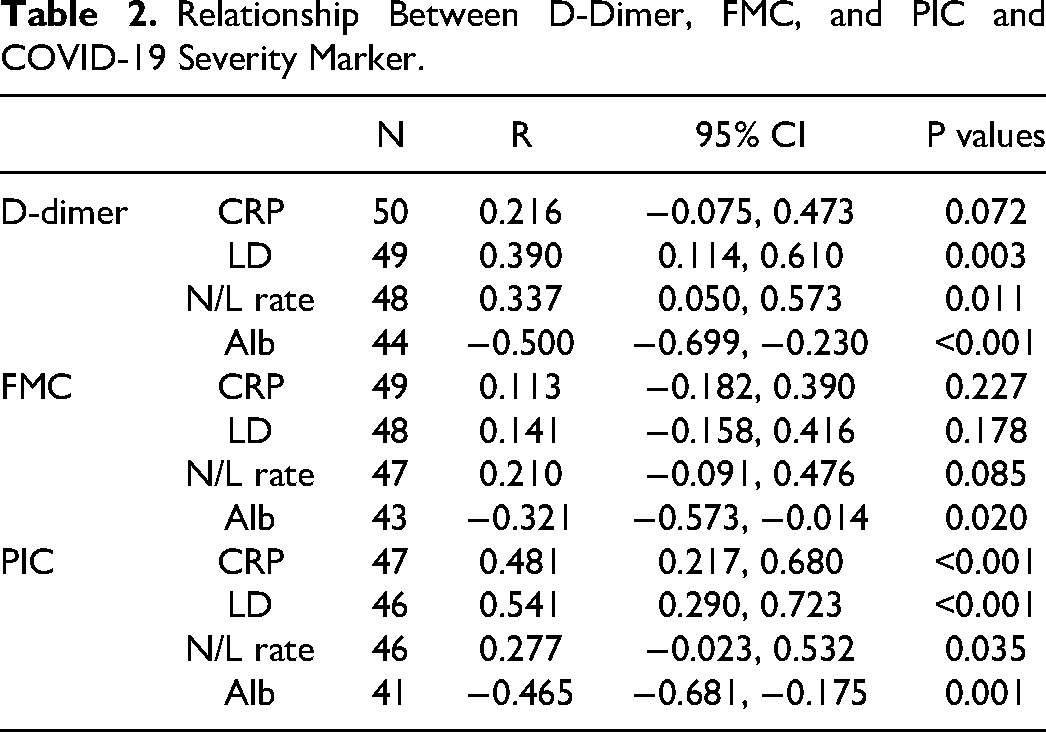
The relationship between FMC, DD, and PIC and the COVID-19 severity markers was evaluated using Spearman's correlation coefficients. The DD levels showed a significant correlation with lactate dehydrogenase (LD) (Rs = 0.390, P = 0.003), serum albumin (Alb) (Rs = −0.500, P < 0.001), and neutrophil-lymphocyte ratio (NLR) (Rs = 0.337, P = 0.011). Similarly, the PIC level significantly correlated with LD (Rs = 0.541, P < 0.001), Alb (Rs = −0.465, P = 0.001), and NLR (Rs = 0.277, P = 0.035). Additionally, PIC levels significantly correlated with C-reactive protein (CRP) (Rs = 0.481, P < 0.001). However, the FMC levels correlated only with Alb (Rs = −0.321, P = 0.020) but not with LD (Rs = 0.141, P = 0.178), NLR (Rs = 0.210, P = 0.085), or CRP (Rs = 0.113, P = 0.227) (Figure 3) (Table 2). Finally, DD levels significantly correlated with PIC levels (Rs = 0.42, P = 0.003; Figure 4).
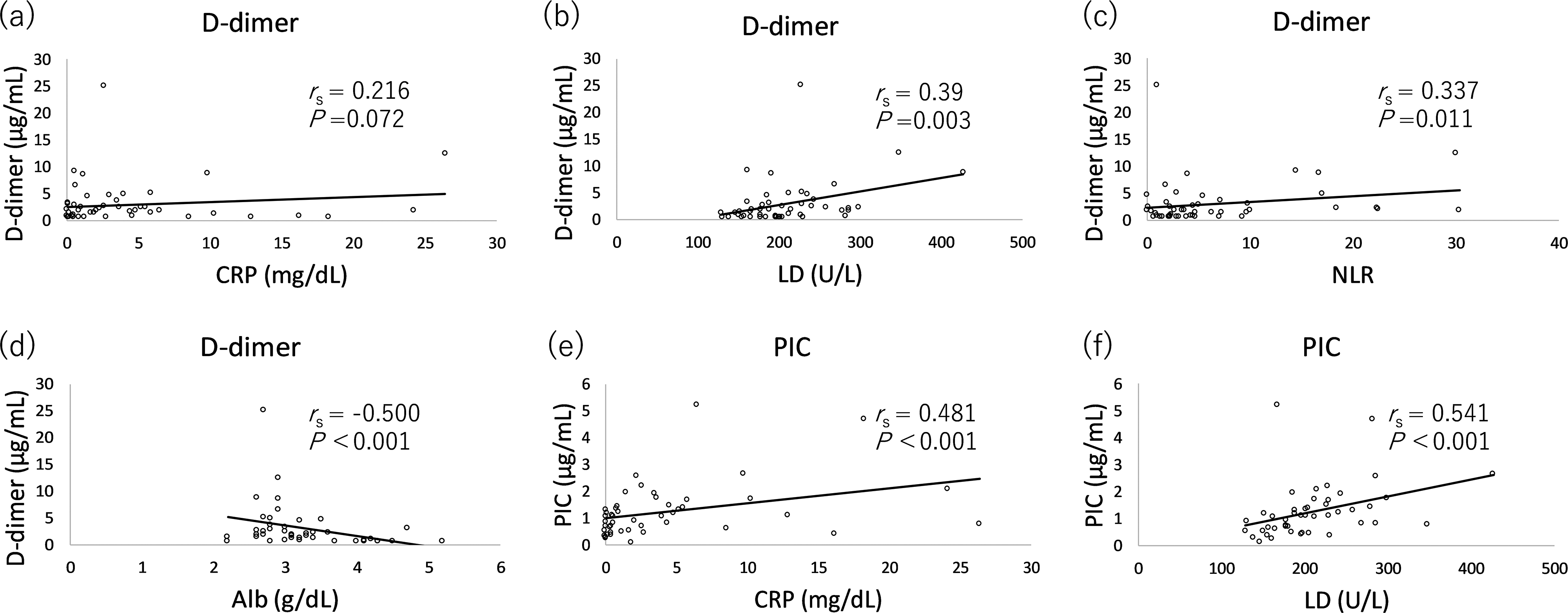
Correlation between D-dimer, FMC, and PIC and COVID-19 severity marker. (a) DD versus CRP; (b) DD versus LD; (c) DD versus NLR; (d) DD versus Alb; (e) PIC versus CRP; (f) PIC versus LD; (g) PIC versus NLR; (h) PIC versus Alb; (i) FMC versus CRP; (j) FMC versus LD; (k) FMC versus NLR; and (l) FMC versus Alb.
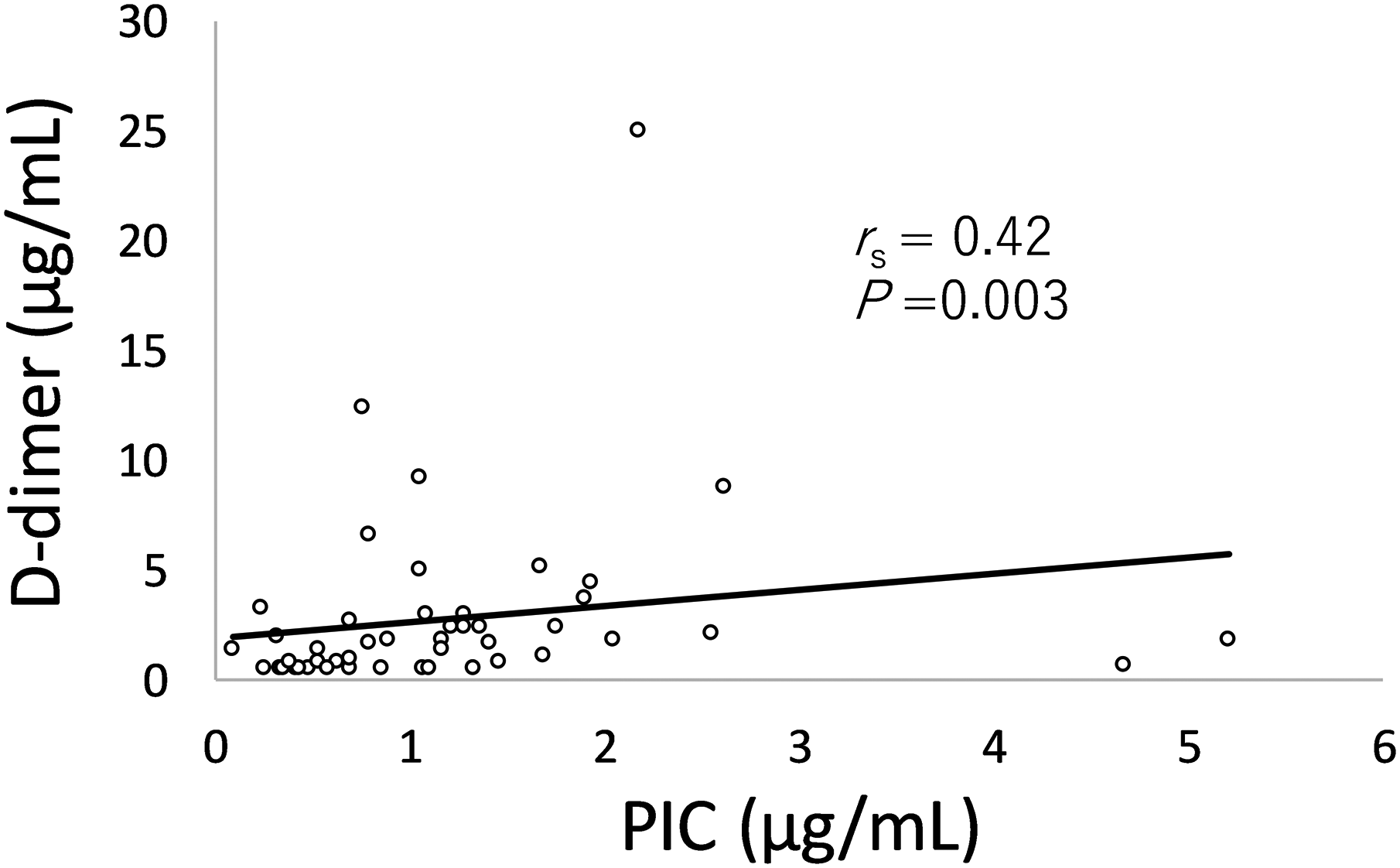
Correlation between D-dimer and PIC.
Relationship Between D-Dimer, FMC, and PIC and COVID-19 Severity Marker.
The ratio of DD to Alb (DAR) was significantly higher in the moderate disease group than that in the mild disease group (Figure 5).
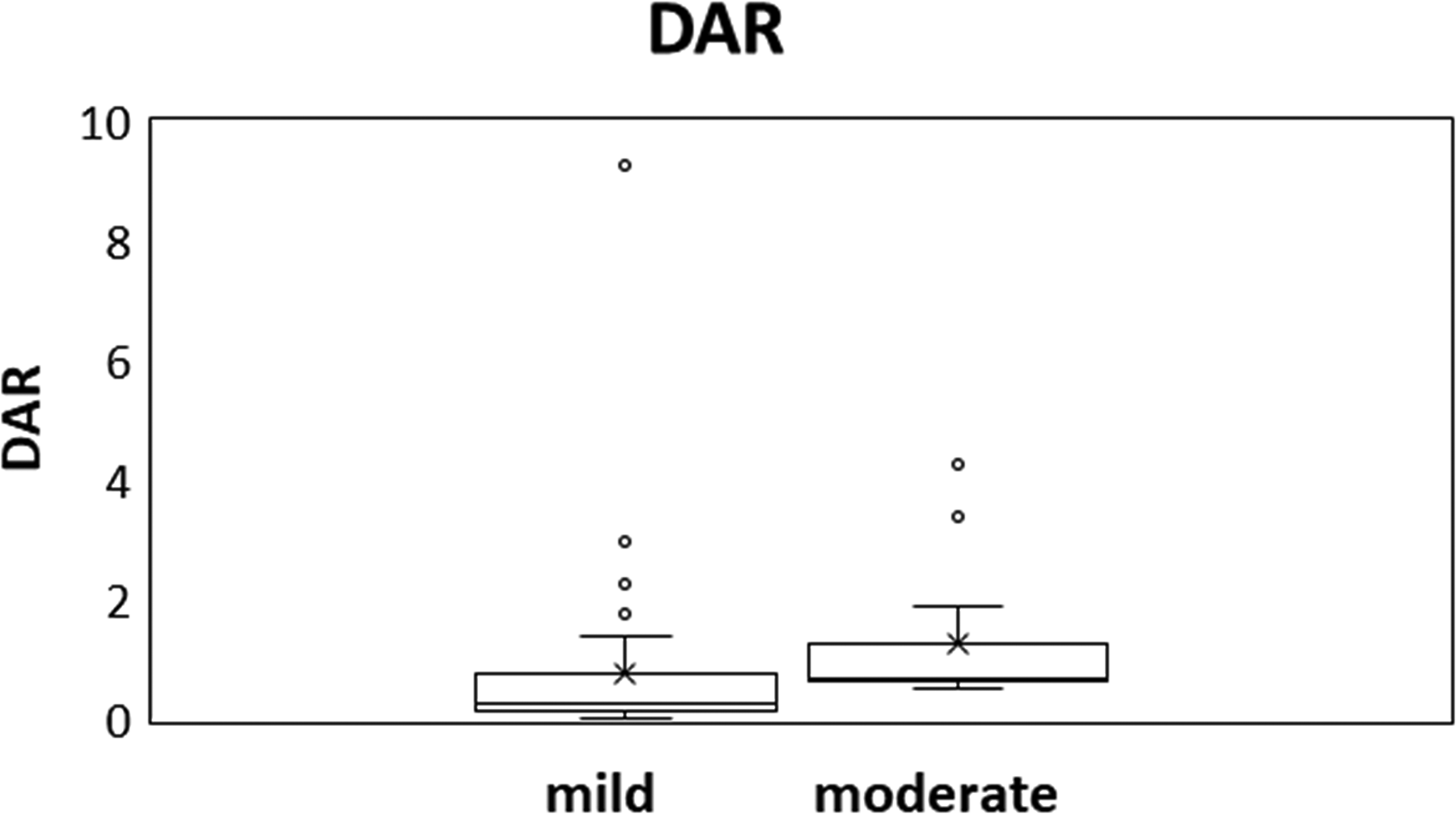
Comparison of DAR in patients with mild versus moderate COVID-19. Each box represents percentile (25th–75th), while the upper and lower whiskers indicate the maximum and the minimum value, respectively.
Discussion
This study investigated the association of COVID-19 severity with DD, FMC, and PIC levels. We found that the DD and PIC levels in patients with moderate COVID-19 were significantly higher than those in patients with mild COVID-19, while the FMC levels were not significantly different between the two patient groups.
As previously reported, DD levels showed correlation with severity. DD, a product of fibrin degradation, plays a mechanistic role in thromboinflammation in COVID-19. 14 In another study with 183 COVID-19 patients, Tang et al concluded that the D-dimer level was approximately 3.5 times higher in patients with severe conditions than in their nonsevere counterparts, 15 Ozen et al showed that when the threshold D-dimer value was 370 ng/ml in the ROC analysis, this value was calculated to have 77% specificity and 74% sensitivity for lung involvement in patients with COVID-19. 16 The low sensitivity in our study may be due to the small number of patients with moderate disease compared to those with mild disease.
PIC is a fibrinolytic marker, and an elevation in its levels signifies fibrinolytic activity due to plasmin production. This increase occurs during endogenous fibrinolytic activation in pathological situations where an in vivo thrombus forms. PIC is a marker of fibrinolytic system activation that predicts thrombus formation, assists in disseminated intravascular coagulation (DIC) diagnosis, and guides antifibrinolytic treatment. Studies on changes in PIC levels in patients with COVID have been inconclusive.17,18
In this study, the PIC level was the variable with the most clearly significant difference between patients with moderate disease and those with mild disease, indicating that it may be a useful indicator of coagulation and fibrinolysis imbalance in patients with COVID-19. PIC levels were most closely correlated with CRP and LD levels, whereas DD levels were most closely correlated with the NLR and the Alb level. Interestingly, CRP and LD are inflammatory markers, whereas the NLR and Alb are markers associated with the immune system.
In recent years, DAR has been shown to play an important role in assessing the prognosis and determining the risk of patients with various diseases, such as COVID-19, subarachnoid hemorrhage, ischemic heart disease, and hepatitis B virus-related cirrhosis.19,20 In patients with COVID-19, the DAR is useful to predict disease severity and prognosis. A high DAR may pose a high risk of thrombus formation and a strong systemic inflammatory response. This has been shown to increase the risk of severe disease and death. 20 In our study, the DAR was significantly higher in the moderate disease group than that in the mild disease group. The results of this study support these findings.
In contrast to DD and PIC, we found that FMC levels were not related to COVID-19 severity. FMC levels are employed to monitor the proteolytic cleavage of fibrinogen by thrombin. Consequently, they serve as a marker of thrombin activity. 21 FMC levels increase when the body is hypercoagulable. Sridharan et al reported that only 23.1% of patients with elevated DD levels had elevated SFMC levels. It has been hypothesized that the elevated DD levels noted in COVID-19 pulmonary infections are a direct consequence of acute lung injury and not overt DIC. 22 Hunt et al also proposed this hypothesis, 23 which is consistent with our findings. Although our study did not include patients with severe COVID-19, such patients reportedly also present with intravascular coagulation limited to the pulmonary vessels. 24 COVID-19-associated coagulopathy rarely progresses to disseminated intravascular coagulation, and only in the late stages of severe cases.25,26 Other reports have indicated that the increase in plasma tissue plasminogen activator exceeds the increase in plasminogen activator inhibitor-1, enhancing the fibrinolytic system. 27
This study had few limitations. First, it was a single-center study with a relatively small number of participants. Second, we did not include severely ill patients. Despite these limitations, this study is important because it is a rare study that evaluates SFMC and PIC levels in patients with COVID-19.
In conclusion, we found that while DD and PIC levels correlated with the severity of COVID-19, FMC levels did not. PIC may be a useful indicator of coagulation and fibrinolysis imbalance in patients with COVID-19. While the first study showed that a high proportion of patients with non-surviving COVID-19 met the ISTH criteria for DIC, 26 subsequent studies have failed to demonstrate a high proportion of patients with COVID-19 meeting the conditions for overt DIC according to the ISTH criteria. 28 We support the hypothesis that the elevated DD levels noted in pulmonary COVID-19 is a direct consequence of acute lung injury and not overt DIC because patients with COVID-19 do not meet the conditions for overt DIC according to the ISTH criteria, and FMC levels do not increase. To further investigate the relationship among FMC, PIC, and COVID-19 severity, larger studies controlling for the time of sample evaluation with respect to COVID-19 are required.
Footnotes
Authors’ Contributions
T.I. designed and performed the study and wrote the first draft of the manuscript; Y.H, N.Y. and H.I. acquired and analyzed the data; K.K. supervised the study.
Data Availability
The data that support the findings of this study are available from the corresponding author, T I, upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.