
Abstract
Interleukin 17F (IL-17F) is an inflammatory cytokine that plays an important role in autoimmune disease by inducing the expression of multiple chemokines, cytokines, and adhesion molecules. In vitro functional analysis revealed that IL-17F rs763780 polymorphism is associated with IL-17 expression and activity. Thus, considering the abnormal percentage of T helper 17 cells in patients with primary immune thrombocytopenia (ITP), we speculated there was a possible association between the IL-17F rs763780 polymorphisms and genetic susceptibility to ITP in a Chinese Han population. A total of 165 patients with ITP and 149 healthy controls were included in this study, and IL-17F rs763780 polymorphisms were analyzed by a polymerase chain reaction–restriction fragment length polymorphism system. The results showed that the frequency of the IL-17F rs763780 G allele in total patients with ITP or patients with chronic ITP was significantly lower than in normal controls (total ITP 3.6% vs controls 7.7%, P = .026; chronic ITP 3.5% vs controls 7.7%, P = .031). However, no significant difference in genotype frequencies was found among total patients with ITP, patients with chronic ITP, and normal controls. We further analyzed the association of IL-17F polymorphisms with clinical parameters of patients with ITP, and no association revealed between gene distribution and first onset age, clinical therapy response to glucocorticoids, or disease course. What’s more, an evident discrepancy with allelic frequencies was observed between female patients with ITP and gender-matched controls. In conclusion, IL-17F rs763780 polymorphisms may be associated with the development of ITP in a Chinese Han population.
Introduction
Primary immune thrombocytopenia (ITP) is an acquired autoimmune disease characterized by decreased platelet count resulting from increased platelet destruction and insufficient platelet production. 1 The pathogenesis of ITP is not completely clarified but it is widely accepted that more than one mechanism could contribute to this disease, such as autoreactive B lymphocytes secreting antiplatelet antibodies, T-cell mediated platelet lysis, and reduced numbers and poor functions of circulating regulatory T cells. 2,3
Autoantibody production by B cells requires the help of autoreactive T cells, and the platelet-reactive CD4+ T cells are therefore involved in ITP by assisting the production of pathogenic antiplatelet autoantibodies. Based on the cytokine profiles, CD4+ helper T cells are traditionally classified into several subsets among which are T helper 1 (Th1), T helper 2 (Th2), and T helper 17 (Th17). The balance among these 3 subsets has been implicated in the regulation of many immune responses and is known to be impaired in various autoimmune diseases. An increased Th1/Th2 ratio in the peripheral blood has been proposed to correlate with disease activity in ITP. 4 –6 Moreover, upregulated Th17 cells may also play a role in the pathogenesis of ITP. 7 –9
Interleukin 17F (IL-17F) is discovered to share a strong homology to IL-17A. They are the members of the IL-17 cytokine family responsible for the pathogenic activity of the Th17 cells. 10 Binding IL-17 to its receptor initiates signaling pathways which induce the production of proinflammatory cytokines and chemokines and induce the recruitment of neutrophils. 11,12 For the critical proinflammatory effect, IL-17F level were elevated and showed a statistically significant correlation with disease activity in patients with systemic lupus erythematosus. 13 In addition, increased IL-17F levels were also found in patients with rheumatoid arthritis 14 and asthma. 15 In our previous study, we found IL-17F messenger RNA was increased in splenocytes of ITP mice than in controls, which suggested that IL-17F may also play a role in ITP. 16
Interleukin 17F encoded gene is mapped to the human chromosome arm of 6p12.2, which consists of 3 exons and 2 introns. 17 IL-17F rs763780 polymorphism is located within the coding region of IL-17 F gene and causes a His-to-Arg substitution at amino acid 161. In vitro functional analysis revealed that IL-17 expression and activity may be suppressed in carriers of the rare G allele. 18 This polymorphism was reported to be associated with the development of some autoimmune disease among asthma, 19 inflammatory bowel disease, 20,21 and multiple sclerosis. 22 Recently, Saitoh et al 23 found that the IL-17F rs763780 G allele is significantly associated with the development of chronic ITP in a Japanese population. However, due to an ethnic disparity, the distribution of the IL-17F rs763780 polymorphism in Chinese population is still unknown. Considering the abnormal percentage of Th17 cells in patients with ITP, we speculated the IL-17F rs763780 polymorphisms were contributed to the genetic susceptibility to ITP. To further unveil the IL-17F rs763780 allele distribution and association with the risk for ITP in a Chinese Han population, we carried out this study.
Methods
Patients
One hundred and sixty-five patients with ITP and 149 geno- and sex-matched healthy controls were included in this study. Informed consent was obtained from the patients’ legal guardians or the patients themselves, and this study was approved by the hospital-based ethics committee. The diagnosis of ITP met the diagnostic criteria as described previously. 24 Primary immune thrombocytopenia was defined as thrombocytopenia (platelet count < 100 × 109/L), normal or increased marrow megakaryocytes, and no secondary immune or nonimmune abnormalities that could account for the thrombocytopenic state. According to the age of first onset, the cases were further stratified into childhood ITP (onset age < 18 years) and adult ITP (onset age ≥ 18 years). In addition, most enrolled patients (n = 125) were treated with glucocorticoids (GCs), including methylprednisolone, dexamethasone, and prednisone. Other patients were received with nonimmunosuppressive treatments such as eltrombopag and recombinant human thrombopoietin. We also analyzed the response to GCs according to the response criteria of the ITP International Working Group. 24 A complete response (CR) is defined as any platelet count of at least 100 × 109/L, and a response (R) was defined as any platelet count between 30 and 100 × 109/L or at least doubling of the baseline count. No response (NR) was defined as any platelet count lower than 30×109/L or less than doubling of the baseline count. All patients were followed up in the outpatient department for at least 12 months from diagnosis. And the patients were classified into newly diagnosed ITP if remission within 3 months, the patients were classified into chronic ITP if course of the disease was more than 12 months, and others were classified into persistent ITP .The characteristics of the patients are shown in Table 1.
The Characteristics of Patients With ITP and Normal Controls Enrolled in This Study.
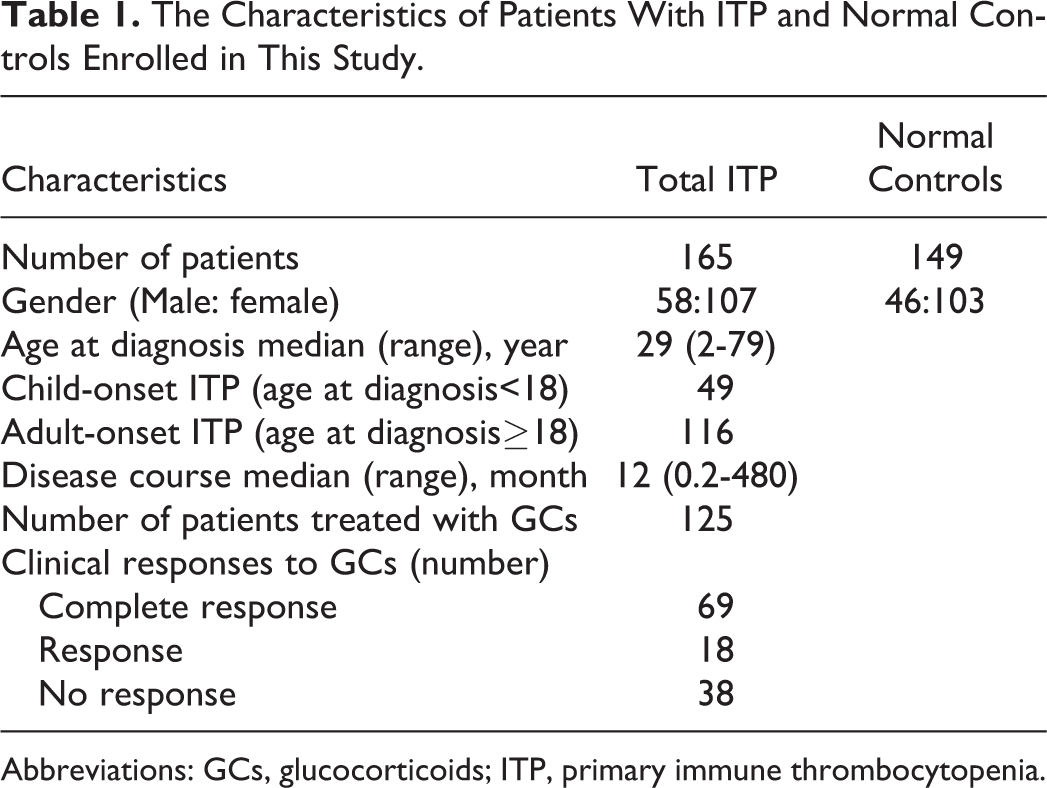
Abbreviations: GCs, glucocorticoids; ITP, primary immune thrombocytopenia.
Extraction of Genomic DNA
Peripheral blood samples were collected in vacuum tubes containing 5% EDTA. Genomic DNA was isolated from peripheral blood using the Wizard genomic DNA purification kit (Promega, Madison, Wisconsin) according to the instructions.
Genotyping
Genotyping was performed using a polymerase chain reaction (PCR)–restriction fragment length polymorphism (RFLP) system. The PCR primers for amplification of the IL-17F rs763780 polymorphism were 5′-GTGTAGGAACTTGGGCTGCATCA AT-3′ (forward) and 5′-AGCTGGGAATGCAAACAAACT-3′ (reverse). The PCR reaction was performed in a final volume of 25 μL containing 50 ng of genomic DNA, 10 pmol of each primer, and 12.5 μL 2 × Premix Taq (Takara, Dalian, China). For PCR amplification, an initial denaturation at 94°C for 5 minutes was followed by 35 cycles at 94°C for 30 seconds, 58°C for 45 seconds, 72°C for 45 seconds, and a final extension at 72°C for 10 minutes. Cleavage was performed with restriction enzymes NIaIII (New England BioLabs, Ipswich, Massachusetts) according to the manufacturer’s protocols. Digested fragments were separated on 2% agarose gels, and RFLP bands were visualized by ethidium bromide staining under UV light. Reproducibility was confirmed by repeating analysis of a random selection of 10% of the cases and controls.
Statistics
Statistical analysis was performed using SPSS 16.0, and the Hardy-Weinberg equilibrium, genotype and allele frequencies were analyzed using the chi-square test or Fisher exact test in case of expected frequencies< 5. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated for each variable. P < .05 was considered as statistically significant.
Results
There were 165 patients with ITP and 149 normal controls included in current study. And most patients with ITP (n = 125) were treated with GCs. At our center, the routine usage of GCs for patients with ITP were methylprednisolone (0.8 mg/kg of body weight) or prednisone (1 mg/kg of body weight) for 2 to 3 months or dexamethasone 40 mg/d for 4 consecutive days (for adults patients).
The genotype of 165 patients with ITP and 149 normal controls were detected, and the genotype frequencies in controls and patients were in the Hardy-Weinberg equilibrium (both P > .05).
The genotype and allele frequencies of IL-17F in total patients with ITP and controls were summarized in Table 2. We first evaluated the IL-17F rs763780 genotype and allele frequencies in all patients with ITP and normal controls, the result showed that the frequency of allele G was significantly lower in total patients with ITP than in the control group. In addition, although IL-17F rs763780 GG genotype was only found in normal controls, the difference of genotype frequency between patients and normal controls did not reach statistic difference. Furthermore, the distribution of this polymorphism was compared between the adult/childhood ITP group and the control with no statistical difference found.
Distribution of the Genotype and Allele Frequencies of IL-17F rs763780 Site in all Patients With ITP and Controls.
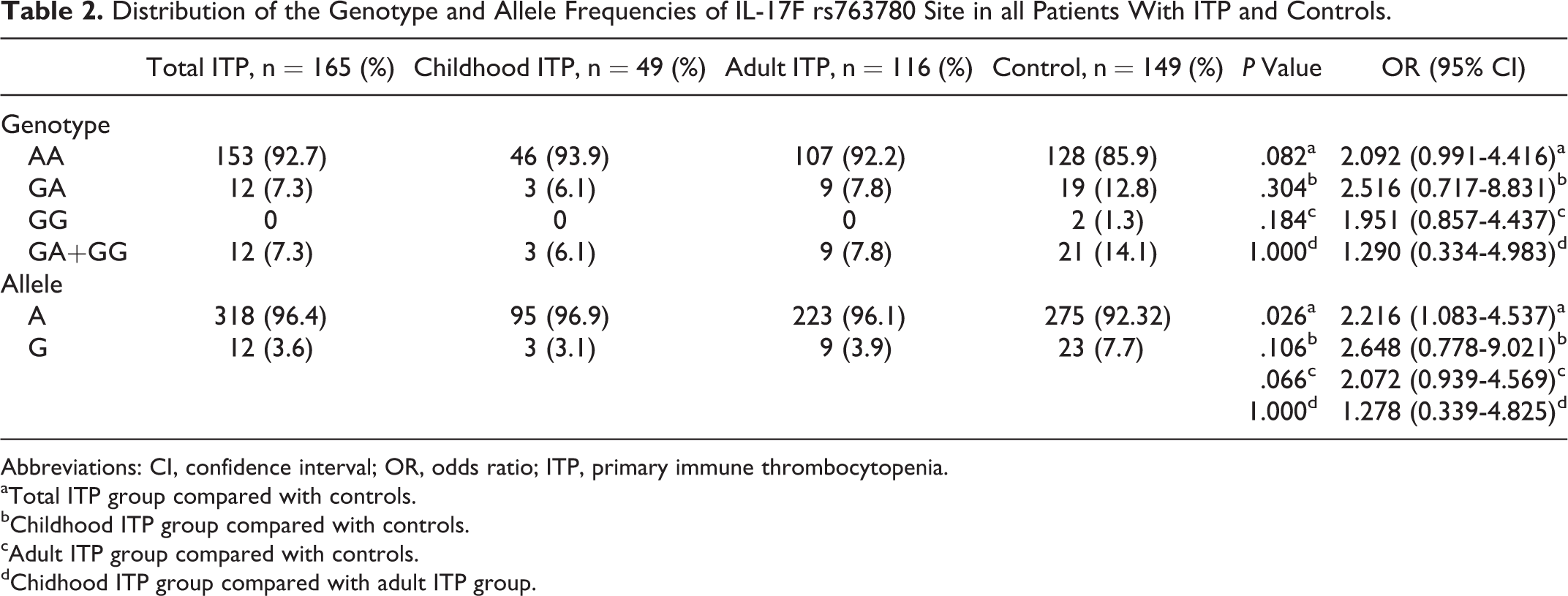
Abbreviations: CI, confidence interval; OR, odds ratio; ITP, primary immune thrombocytopenia.
aTotal ITP group compared with controls.
bChildhood ITP group compared with controls.
cAdult ITP group compared with controls.
dChidhood ITP group compared with adult ITP group.
As a first-line therapy strategy, most of the enrolled patients (n = 125) received the GCs treatment, thus, we analyzed the association between IL-17F polymorphisms and the clinical responses to GCs treatment. However, no statistical differences were detected in genotypes and allelic frequencies between the CR + R and NR groups (Table 3).
Stratification Analysis of the Relation Between IL-17F rs763780 Site Polymorphism and Clinical Responses to Glucocorticoids in Patients With ITP.
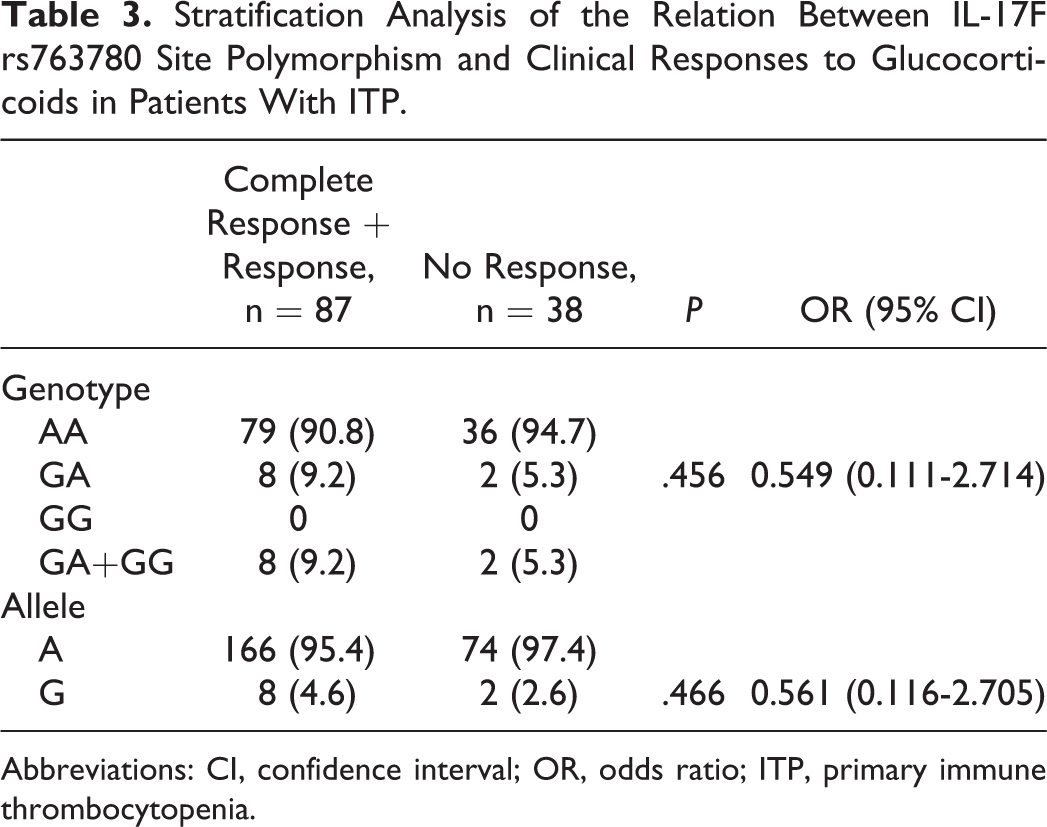
Abbreviations: CI, confidence interval; OR, odds ratio; ITP, primary immune thrombocytopenia.
In addition, based on the disease course after follow-up, we subdivided the patients into 3 groups: newly diagnosed, persistent, and chronic ITP. We then evaluated the genotype and allele distribution among each of these 3 subsets, and no differences were found (Table 4). However, the frequency of allele G was significantly lower in chronic ITP groups than in the control group, In detail, the G allele frequency was 3.5% in patients with chronic ITP versus 7.7% in controls (P = .031, OR = 2.333, 95% CI =1.059-5.136)
Stratification Analysis of the Relation Between IL-17F rs763780 Site Polymorphism and Disease Course of Patients With ITP.
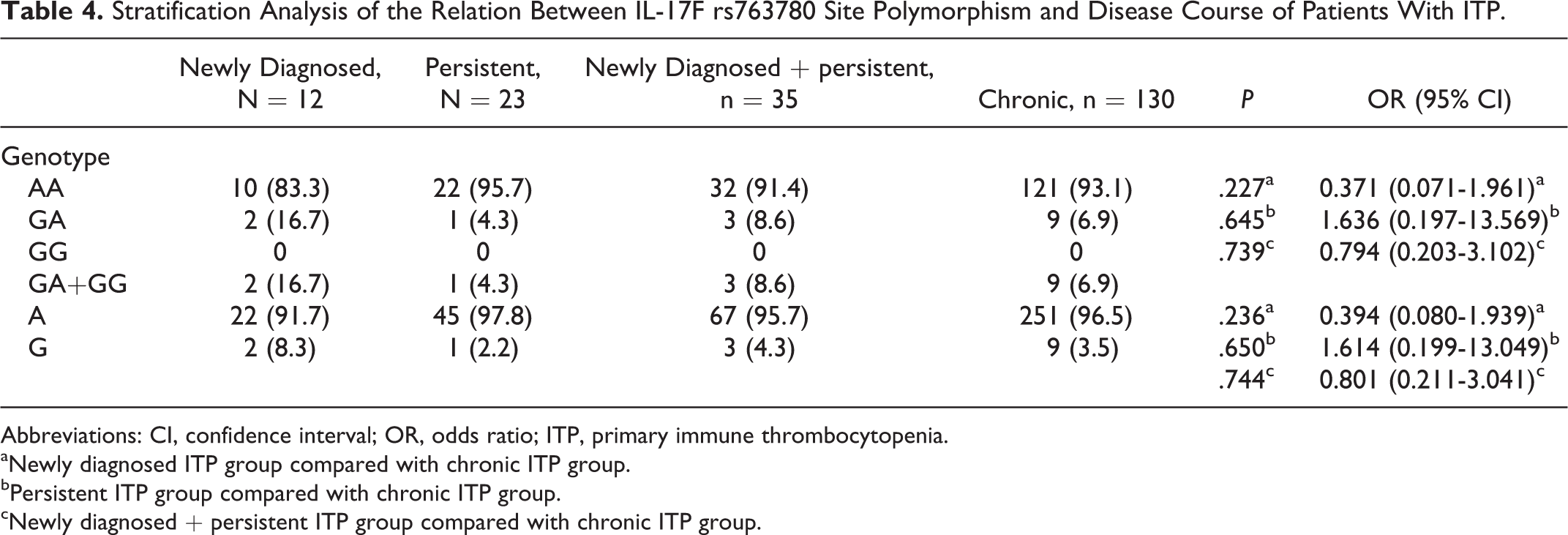
Abbreviations: CI, confidence interval; OR, odds ratio; ITP, primary immune thrombocytopenia.
aNewly diagnosed ITP group compared with chronic ITP group.
bPersistent ITP group compared with chronic ITP group.
cNewly diagnosed + persistent ITP group compared with chronic ITP group.
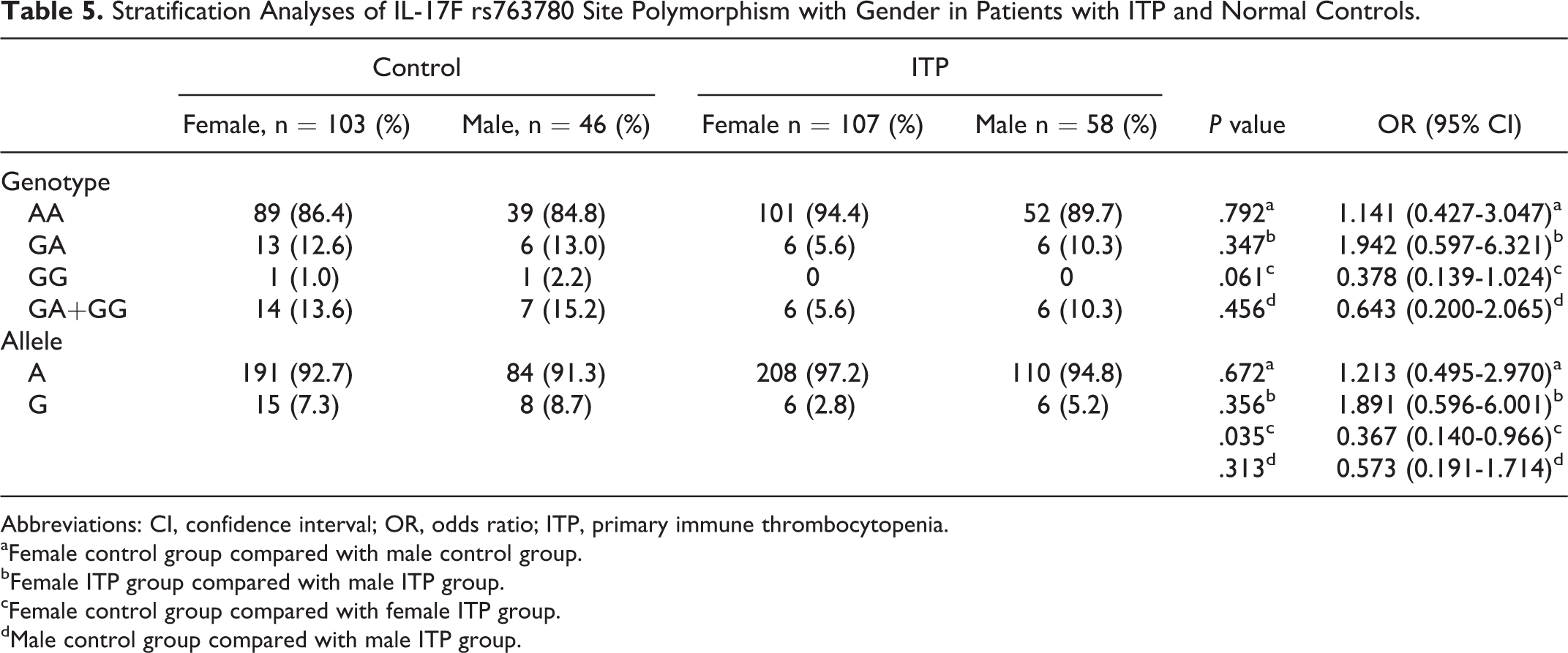
As shown in Table 5, an evident discrepancy with allelic frequencies was observed between female patients with ITP and gender-matched controls. However, no differences was detected in genotypes between these 2 groups. In addition, no statistical differences were detected in genotypes and allelic frequencies between the male cohorts and between female controls and male controls.
Stratification Analyses of IL-17F rs763780 Site Polymorphism with Gender in Patients with ITP and Normal Controls.
Abbreviations: CI, confidence interval; OR, odds ratio; ITP, primary immune thrombocytopenia.
aFemale control group compared with male control group.
bFemale ITP group compared with male ITP group.
cFemale control group compared with female ITP group.
dMale control group compared with male ITP group.
Discussion
Although ITP was previously thought to be Th1-cell driven, it is now recognized that a distinct lineage of effector T cells, Th17 cells, is also involved in the development of ITP. Recently, more and more researchers found the circulating percentage of Th17 was markedly higher in patients with ITP than in normal controls. 9,8,25,26 However, some groups argued that Th17 cells count did not differ between patients with ITP and normal controls. 27,28 These differences could be due to the heterogenicity of ITP and sensitivity of the technique used. Besides Th17, Hu et al found that the number of Tc17 (defined as CD3+CD8+IL-17+) was significantly increased in newly diagnosed patients but not in patients who had CR, which indicated the importance of Tc17 in the development of ITP. Moreover, the percentage of Tc17 in patients with ITP was decreased with the addition of dexamethasone in vitro, strongly suggesting that Tc17 may be involved in the pathogenesis of ITP. 29
Considering the key role of Th17/Tc17 in immunity, as a main effector cytokine, IL-17 is believed to play a crucial role in inflammation by inducing activation of various proinflammatory cytokines, such as IL-1, IL-6, and interferon γ. Until now, although the exact mechanism of IL-17F in ITP is still unknown, IL-17F expression was elevated in splenocyte from ITP mice, and the genotype and IL-17F rs763780 G allele are significantly associated with the development of chronic ITP in a Japanese population, suggesting a role for IL-17F in the pathogenesis of ITP. 23 Thus, in the present study, we evaluated the association between IL-17F polymorphisms and ITP susceptibility in a Chinese Han population.
IL-17F rs763780 polymorphism causes a His-to-Arg substitution at amino acid 161 (H161R) of IL-17F and lacked the ability to activate the mitogen-activated protein kinase pathway, cytokine production, and chemokine production. 18 Paradowska-Gorycka et al 30 discovered that the presence of the rare IL-17F G variant (rs763780) associated with lower expression of IL-17F and thus affect the disease susceptibility and activity of rheumatoid arthritis in the Polish population. A growing body of researchers found IL-17F rs763780 G and genotype GG to be associated with a decreased risk for many autoimmune diseases, including ITP. 23 For gene distribution frequency is correlated with ethnicity, in order to known the association of IL-17F rs763780 polymorphism and genetic suspect to Chinese patients with ITP, we investigated the genotype and allele frequencies of IL-17F rs763780 sites in a Chinese Han population. In accordance with Saitoh’s research, the frequency of G allele of IL-17F single nucleotide polymorphism (SNP) rs763780 was found to be significantly decreased in patients with ITP, suggested that the G allele has protective effect on the development of ITP. This is in accordance with 2 independent studies highlighted the possibility that IL-17F SNP might be an important regulator in ITP pathogenesis. However, the exact mechanisms by which IL-17F SNP modulates the susceptibility is still unknown, we speculated the carriers of G allele suppressed IL-17F expression and activity, thus further protected the development of ITP. Besides comparing the gene distribution between total patients with ITP and normal controls to well understand the contribution of IL-17F rs763780 polymorphism to ITP pathogenesis, we analyzed the distribution of genotype and alleles between normal controls and different subsets of patient with ITP, which were divided by different clinical parameters including first onset age, clinical responses to GCs, disease course, and gender. And consistent with previous research, 23 we found the frequency of G allele was decreased in patients with chronic ITP, implying the rare IL-17F G variant associated with disease development of ITP. In addition, in the gender-matched analysis, we observed an association of IL-17F rs763780 allele G with ITP in female, suggesting that the decreased distribution of protective allele may contribute to elevated morbidity of ITP in female. However, no significant association was detected between IL-17F polymorphism and GCs responses/first on-set age of ITP patients. Saitoh et al 23 also found patients with the IL-17F rs763780 AA genotype showed a severe thrombocytopenic state at diagnosis than those with the IL-17F rs763780 AG genotype. In our study, we could not get the exact platelet number at diagnosis because most patients were first diagnosed in other hospital, we cannot compare the number of platelet among the patients with ITP harboring different genotypes of alleles.
In general, the result of this investigation indicated that G allele of rs763780 was significantly associated with the susceptibility to ITP in the Chinese population. However, this research may have several limitations. It is worthwhile to point out how this SNP exerts its role to achieve pathogenesis of ITP. Besides, additional prospective studies with large samples and different ethnic populations are needed to evaluate the role of IL-17F gene polymorphism in patients with ITP in the future.
Footnotes
Authors’ Note
Huiyuan Li and Zeping Zhou contributed equally to this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by grants of National Natural Science Foundation of China (81270581, 81260091, 81300385, and 81470286), Tianjin Municipal Science and Technology Commission (14JCZDJC35100), Specialized Research Fund for the Doctoral Program of Higher Education (20131106120039), Peking Union Medical College Youth Fund and the Fundamental Research Funds for the Central Universities (3332013068), Yunnan Provincial Science and Technology Department-Kunming Medical University Joint Special Foundation (2013FB152), High-level health technical leader training plan of Yunnan Province (D-201216), and Young prospective academic and technical leader training plan of Yunnan Province (2013HB088).