
Abstract
This study was conducted to compare the platelet count and the presence of bleeding manifestations at initial diagnosis of immune thrombocytopenic purpura (ITP) between patients with primary and secondary ITP. Medical records for 67 consecutive adult patients with ITP were reviewed retrospectively and the relevant data were abstracted. Thirty-eight (56.7%) patients were diagnosed as having primary ITP and 29 (43.3%) were considered to have secondary ITP. At the time of diagnosis, the median initial platelet count (median: 60 × 109/L) for patients with secondary ITP was significantly (P < .005) higher than that for patients with primary ITP (median: 3.5 × 109/L). Ecchymosis and/or purpura was observed in 4 (13.8%) patients with secondary ITP and in 33 (86.6%) patients with primary ITP (P value <.005). In conclusion, patients with secondary ITP had higher platelet count at diagnosis and were less likely to present with bleeding manifestations than those with primary ITP.
Introduction
Immune thrombocytopenic purpura (ITP) is an autoimmune disorder characterized by peripheral platelet destruction caused by autoantibodies and suppression of thrombopoiesis.1–5 Secondary ITP may be associated with autoimmune diseases, malignancy, infections, and others causes. 6 With regard to the pathogenesis of secondary ITP, it is unclear whether this form of ITP represents a distinct entity or a manifestation in the clinical spectrum of the accompanying disease. Comparing the clinical and laboratory features of patients with primary and secondary ITP may reveal distinct profiles, although few such studies have been performed.
The clinical association of ITP with other diseases is well recognized. The prevalence of secondary ITP among patients with underlying diseases varies considerably from 1% to 60%, depending on the underlying disease.7–11 Most of the studies concerning secondary ITP characterized the underlying diseases 12 but not the core issues of ITP, which include the initial platelet count, the presence or absence of bleeding particularly mucocutaneous purpura, and the need for treatment. Therefore, these core issues need to be further addressed by comparing patients with primary and secondary ITP.
This study was conducted to compare the platelet count and the presence of bleeding manifestations (ie, mucocutaneous purpura) at initial diagnosis of ITP between patients with primary and secondary ITP.
Methods
This study was approved by the King Abdullah University Hospital (KAUH) Institutional Review Board committee. The medical records of all consecutive patients who were diagnosed with ITP in the outpatient clinics at KAUH between September 2002 and August 2010 were reviewed. The KAUH is an 800-bed tertiary care center located in Irbid, northern Jordan. Patients were included in this study if their age at diagnosis was 16 years or more, their ITP was defined according to the American Society of Hematology (ASH) criteria,13,14 and their platelet count was low (<100 × 109/L). Exclusion criteria included the following: pregnancy, the presence of splenomegaly (except those autoimmune hemolytic anemia with positive direct antiglobulin test [DAT] and the presence of mild splenomegaly), and having received treatment that may cause drug-induced thrombocytopenia.
The demographic and clinical characteristics of patients at the initial diagnosis of ITP were abstracted from their medical records. These data included age, gender, initial platelet count, initial presentation of mucocutaneous purpura, the need for treatment of ITP according to ASH guidelines,13,14 and whether or not treatment was prescribed. Furthermore, data about the response to treatment and results of screening for antinuclear antibody (ANA), hepatitis C virus (HCV), hepatitis B virus (HBV), and human immunodeficiency virus (HIV), and antiphospholipid (APL) antibody were abstracted from the medical records. The performed clinical investigations included chest X-ray, abdominal ultrasound, and further tests according to the concurrent clinical condition. All of the previous tests were done routinely in our hospital in patients with thrombocytopenia for the first time. Based on the investigations at the time of diagnosis, patients were admitted if the platelet count was <20 × 109/L and/or if they had bleeding including ecchymosis or purpura.
Data were analyzed using the Statistical Package for Social Sciences software (Version 15; SPSS, Inc, Chicago, Illinois). Frequency and percentage were used to describe categorical variables and the mean (standard deviation [SD]) and median were used to describe continuous variables wherever appropriate. An independent t test was used to test for the differences between 2 means, Mann-Whitney U test was used to test for the differences between 2 medians, and a chi-square test was used to test for the differences between percentages. A P value of less than .05 was considered statistically significant.
Results
A total of 67 patients who were diagnosed with ITP at KAUH between September 2002 and August 2010 met the inclusion criteria and were included in this study. Their age at diagnosis ranged between 16 and 82 years, with a mean (SD) of 32.5 (14.3). More than two thirds of the patients (71.6%) were females. All patients were tested for the presence of HCV, HBV, and HIV, and none tested positive.
Thirty-eight (56.7%) patients were diagnosed as having primary ITP and 29 (43.3%) were considered to have secondary ITP because the ITP was associated with another underlying disorder or condition. A concurrent autoimmune disease was observed in 22 (75.9%) patients who were diagnosed with secondary ITP. Of those who were diagnosed with secondary ITP, 9 (31.0%) had systemic lupus erythematosus, 7 (24.1%) had APL syndrome, 2 (6.9%) had Evan syndrome, and 2 (6.9%) had Hodgkin disease. Each of the remaining patients had only one of these conditions: renal cell carcinoma, sarcoidosis, and positive ANA.
Table 1 shows the characteristics of patients with primary and secondary ITP. Patients with secondary ITP were significantly older than patients with primary ITP (P = .027). About two thirds of patients (64.3%) with secondary ITP and one third (36.8%) of patients with primary ITP were aged ≥30 years. The mean (SD) age was 30.4 (14.5) years for patients with primary ITP and 35.4 (13.6) years for patients with secondary ITP. Among patients with secondary ITP, the mean age of patients with an associated autoimmune diseases (mean: 30.2 years) was significantly (P = .002) lower than that for patients with other disorders (mean: 51.1 years). At the time of diagnosis, the median initial platelet count (median: 60 × 109/L) for patients with secondary ITP was significantly (P < .005) higher than that for patients with primary ITP (median: 3.5 × 109/L). More than two thirds of patients with secondary ITP (69.0%) and no patient with primary ITP had an initial platelet count >30 × 109/L. Among patients with secondary ITP, the median initial platelet count for patients with an associated autoimmune disease was not significantly different from that for patients with other disorders (P = .636).
Demographic and Clinical Characteristics of Patients With Primary or Secondary Immune Thrombocytopenic Purpura.
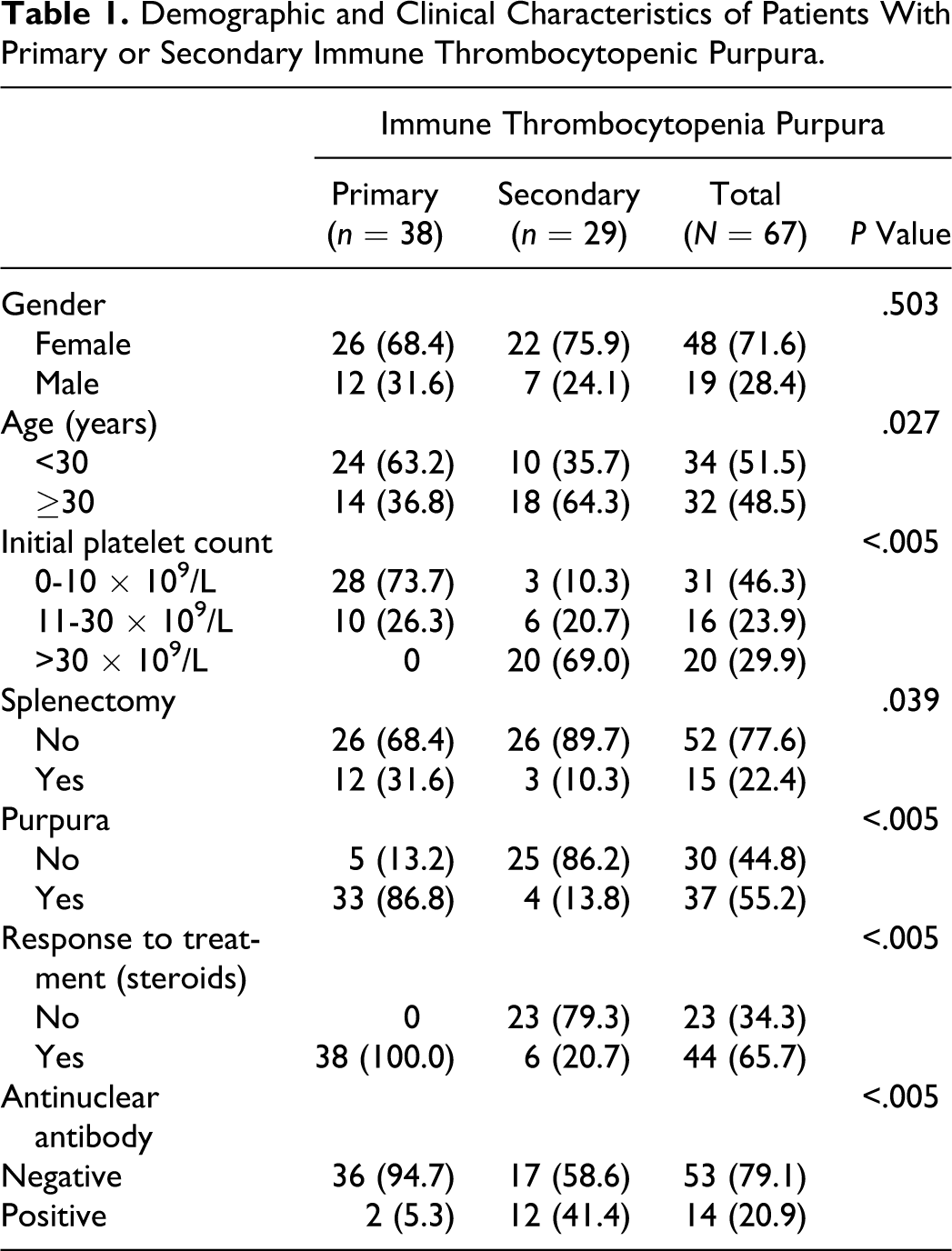
At the time of diagnosis, ecchymosis and/or purpura was observed in 4 (13.8%) patients with secondary ITP and in 33 (86.6%) patients with primary ITP (P value <.005).
Twelve patients with primary ITP underwent a splenectomy. Of those, 2 patients needed other forms of treatment for ITP (ie, Rituximab). Three patients with secondary ITP received treatment at the time of diagnosis because of severe thrombocytopenia (platelet count <5 × 109/L) with bleeding symptoms in the form of ecchymosis and purpuric rash. All 3 had poor responses to corticosteroid treatment and required splenectomy.
Discussion
Despite the distinction between primary and secondary ITP, 6 comparative studies of well-defined groups of patients with ITP associated with an underlying disease (secondary ITP) or with primary ITP are lacking. In an attempt to better define the distinctive features of secondary ITP, we compared the clinical and laboratory characteristics and treatment requirements between 29 patients with well-defined secondary ITP and 38 patients with primary ITP. In this study, we included only patients who were referred to the KAUH Internal Medicine Department for low platelet count. To avoid any misdiagnosis, we excluded pregnant women and patients who were on medications associated with thrombocytopenia.
In clinical practice, ITP may present with a variety of underlying diseases and conditions. For this reason, we strongly agree that ITP should be classified as primary (idiopathic) or secondary (associated with an underlying disorder). 15 The high rate and the variety of associated conditions or diseases found in the present study strongly support the need for this classification.
Secondary ITP was predominantly associated with autoimmune diseases (76%). Systemic lupus erythematosus was the most common autoimmune disorder associated with ITP, followed by APL syndrome. Seven patients with autoimmune disorders were taking immunosuppressive drugs. Malignant conditions including Hodgkin lymphoma, T cell lymphoma, and renal cell carcinoma were less common.
The female-to-male ratio in our patients with ITP was 2.5:1, which is consistent with the findings of other investigators.16,17 With regard to age at the time of diagnosis, patients with secondary ITP were significantly older than patients with primary ITP. The mean age for patients with secondary ITP associated with autoimmune disorders was significantly lower than that for patients with other disorders. Thus, looking for secondary causes other than autoimmune disorders in elderly patients is very useful.
The severity of thrombocytopenia at the time of diagnosis was strikingly different between the groups. We found that the initial median platelet counts were significantly lower in patients with primary ITP. This finding suggests that thrombocytopenia in patients with secondary ITP is usually asymptomatic and not associated with significant bleeding manifestations compared with primary ITP. The reasons for this difference could be explained by the presence of different mechanisms for thrombocytopenia in primary and secondary ITP or because patients with secondary ITP were already under medical attention which led to the incidental finding of low platelets. Nearly three quarters of patients with primary ITP presented with an initial platelet count ≤10 × 109/L compared with only one tenth of those with secondary ITP. Therefore, bleeding manifestations in the form of skin purpura were more predominant in patients with primary ITP than in patients with secondary ITP.
The core issue when determining the treatment for a patient with ITP is to decide whether the patient should be treated at all. According to ASH guidelines,13,14 the need for treatment in patients with ITP depends on the severity of thrombocytopenia and the presence of bleeding.
Corticosteroids are the frontline therapy for ITP. As observed in our study, all patients with primary ITP needed treatment with steroids an initial therapy, and 12 (31.6%) of 38 patients underwent a splenectomy because they required a high dose of steroids for a long period. Only 3 patients (10.3%) with secondary ITP needed treatment for severe thrombocytopenia, and these patients had the following conditions: sarcoidosis, renal cell carcinoma, and APL syndrome. However, the majority of patients with secondary ITP did not require treatment of thrombocytopenia. This may be explained that some patients with secondary ITP especially with underlying autoimmune disorders are already on immunosuppressive agents.
We did not find any case of viral-associated ITP. We did not find any patient with HCV-, HBV-, or HIV-associated thrombocytopenia; however, the exclusion of patients with splenomegaly may have led to the exclusion of some of those patients.
In conclusion, the median initial platelet count for patients with secondary ITP was significantly higher than that for patients with primary ITP at the time of diagnosis. Patients with secondary ITP were less likely to present with ecchymosis and/or purpura as compared to patients with primary ITP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.