
Abstract
Objective:
Emergency physicians frequently deal with patients on vitamin K antagonists (VKAs) suffering major bleeding events, and rapid reversal of anticoagulation in this setting is of paramount importance. In Italy, given the absence of specific national guidelines, local policies are likely to differ, possibly impacting on clinical outcomes. We decided to perform a telephone survey among Italian emergency physicians to evaluate management strategies for VKAs reversal in patients with major bleeding.
Methods:
We conducted a computer-assisted, 10-minute telephone survey of 15 questions, focusing on the local prevalence, assessment, and management strategies of major and intracranial hemorrhage (ICH) occurring in patients on VKAs. We planned to interview a sample of 320 Italian emergency physicians. Institutions from all geographic areas of Italy were to participate in the survey.
Results:
Of the 320 physicians contacted, 150 (47%) completed the survey, 95% being employed in public hospitals. Focusing on ICH, only 29% of the responders stated they would reverse anticoagulation irrespective of the international normalized ratio value, and only 27% would use prothrombin-complex concentrate as first-line agent. In patients needing urgent neurosurgical operation, less than 50% would administer prothrombin-complex concentrate before surgery.
Conclusion:
The average knowledge of management strategies for reversal of anticoagulation displayed by Italian emergency physicians appears to be unsatisfactory. The need for an extensive educational program and for the implementation of specific guidelines, possibly endorsed by Scientific Societies, cannot be underemphasized.
Keywords
Introduction
Vitamin K antagonists (VKAs) are widely used in Western countries for the prevention and treatment of venous and arterial thromboembolism. Due to their narrow therapeutic window, they need to be closely monitored to ensure the best trade-off between efficacy and safety. 1,2 Owing to the numerous interactions of VKA with other commonly employed drugs, food, and herbal compounds, many patients will frequently have international normalized ratio (INR) values outside the therapeutic range. 3 In fact, when the INR falls below 2, patients are at higher risk of developing (recurrent) thromboembolic events; that is, those one wants to prevent or treat by having the patients on anticoagulants. 4 On the other hand, when the INR value raises above 3, the risk of hemorrhagic adverse events increases; among those, the most feared are fatal and major (especially intracranial) bleedings. 4
Emergency physicians are frequently challenged with the management of patients on VKA suffering major bleeding events. In this setting, rapid reversal of anticoagulation along with ongoing cardiovascular resuscitation are of paramount importance. 5
In Italy, given the paucity of available literature and the absence of specific national guidelines endorsed by emergency medicine societies, it is likely that local policies will widely differ, with a possible impact on clinical outcomes. 6,7
To evaluate this important issue, we decided to perform a survey among Italian emergency physicians to evaluate the current management strategies for VKA reversal in patients with major bleeding.
Methods
The survey was conducted in December 2012, employing a computer-assisted telephone interview. We planned to interview a sample of 320 physicians working full time in an Italian Emergency Department; that is, at least 2 physicians from each of the 144 Local Socio-Sanitary Units comprising at least 2 hospitals, located on the Italian territory. Only 1 physician per hospital was eligible for the survey. In order to intercept potential regional patterns, Institutions from the north, the center, and the south of Italy were evenly selected to participate in the survey.
The intended duration of the telephone interview was 10 minutes. The survey comprised 15 multiple-choice or open questions (Table 1), focusing on the local prevalence, assessment, and management strategies of major and intracranial hemorrhage (ICH) occurring in patients on VKA. Furthermore, we also sought to assess the physicians’ general knowledge about the relevant data coming from the literature.
The Telephone Survey.a,b
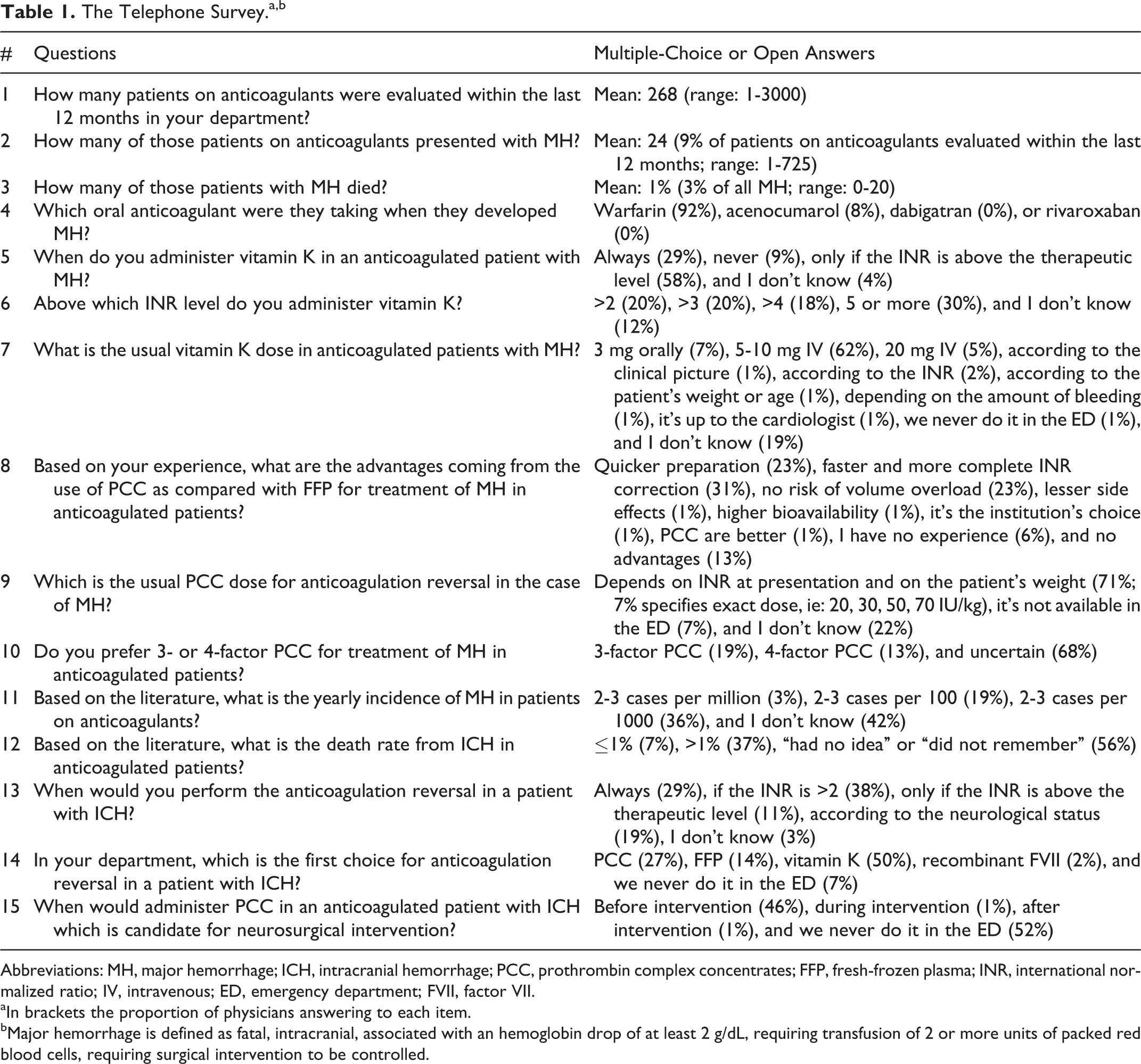
Abbreviations: MH, major hemorrhage; ICH, intracranial hemorrhage; PCC, prothrombin complex concentrates; FFP, fresh-frozen plasma; INR, international normalized ratio; IV, intravenous; ED, emergency department; FVII, factor VII.
aIn brackets the proportion of physicians answering to each item.
bMajor hemorrhage is defined as fatal, intracranial, associated with an hemoglobin drop of at least 2 g/dL, requiring transfusion of 2 or more units of packed red blood cells, requiring surgical intervention to be controlled.
Results
Participants
Of 320 physicians contacted, 150 (47%) completed the survey. Responders were uniformly distributed among the 3 main geographic areas (north, n = 50; center, n = 50; and south, n = 50) of Italy, and 95% were employed in public hospitals. The physician’s mean age was 48 years (range: 31-62), 37% were female (north, 50%; center, 34%; and south, 28%), and 80% of them graduated before 2000.
In all, 85% (128 of 150) of the participants had a full-time job in the emergency department; 69% (104 of 150) were consultant either in emergency or internal medicine, while only a minority (13%) had a residency in general or vascular surgery. Specifically, 14% (21 of 150) were employed in institutions serving a population of more than 300.000 people, 37% (55 of 150) worked in hospitals serving a population between 150.000 and 300.000 people, and the remaining in organizations serving between 80.000 and 150.000 people.
All of the interviewed physicians claimed to be personally concerned with the management of major hemorrhage (MH) occurring in patients on VKA, though in almost 90% of the cases they were assisted by another specialist. Among them, those more often involved were internists (39%), general or vascular surgeons (36%), cardiologists (17%), and neurologists (13%). Interestingly, intensive care specialists were barely (3%) called on in these cases.
A formal internal protocol or guideline for the management of VKA-induced major bleeding was in use in 29% of the emergency departments surveyed.
Survey: Overall Findings
First of all, participants were asked to give an estimate of the magnitude of the issue. The reported average number of patients on VKA presenting to the 150 sampled emergency departments during the 12 months preceding the survey was 268 (range: 1-3000), being 24 (9%, range: 1-725) the mean number with MH, and 1% (3% of all MH, range: 0-20) the corresponding figure for MH-related deaths. Warfarin was used by 92% of the patients presenting with MH, the remaining 8% being on acenocumarol.
Responders were then queried about VKA reversal strategies employed at their institutions for patients with MH. First, they were asked when would they give vitamin K, and the large majority stated they would either use it in the case of supratherapeutic INR values (58%), or “always” (29%). Notably, 9% claimed they would never give vitamin K to those patients, and 4% admitted they “didn’t know.” When questioned about the INR threshold above which they would administer vitamin K, 80% of the physicians indicated an INR value between 2 and 6 (namely, >2 = 20%, >3 = 20%, >4 = 18%, and >5 = 22%), another 8% specified an INR of “6 or higher,” and 12% stated they “had no idea.” Coming to the dose of vitamin K to be used, most physicians (62%) indicated they would give 5 to 10 mg intravenously, while some 10% favored either 20 mg intravenously (5%) or 3 mg orally (7%). Another 20% answered they “had no idea” (19%) or that they would “never use” vitamin K in those patients (1%). The remaining 6% specified vitamin K dose should be established “based on the clinical picture,” on the intensity of bleeding, or according to the patients’ INR, weight, and age.
Second, physicians were asked which advantages would they expect from using prothrombin complex concentrates (PCCs) instead of fresh-frozen plasma for treatment of MH. A quicker preparation (23%), a faster and more complete INR correction (31%), and no risk of volume overload (23%) were perceived as the most important benefits of PCC by the majority of responders. Another 13% reported they saw no advantage of PCC over fresh-frozen plasma, and 6% reported to have “no experience with PCC.” The remaining 4% pointed either to the higher bioavailability (1%) or to the reduced side effects (1%), or claimed that PCCs were “the institution’s choice” (1%) or—simply—“better” (1%). When considering how to establish the dose of PCC to be used, 71% related it either to the INR at presentation or to the patient’s weight; although only 7% of them specified a given amount of IU per kg (eg, 20 IU/kg, etc). The remaining reported that PCC were not available at their institution (7%) or that they didn’t know (22%). Finally, physicians were asked whether they preferred 3-factor or 4-factor PCC. In all, 68% stated they were uncertain, lacking head-to-head comparisons in the literature, while 19% favored the 3-factor PCC, and 13% the 4-factor PCC, respectively.
In the subsequent part of the survey, physicians were interviewed about the anticoagulation reversal strategies they would employ in patients with ICH.
First, they were asked when would they perform anticoagulation reversal: 38% claimed they surely would if the INR level were >2, 11% if the INR were >3, and 29% affirmed they would “always” reverse anticoagulation. Another 19% stated they would perform reversal according to the neurological status, and only 3% admitted they didn’t know.
Second, physicians had to specify the first choice for VKA reversal in the setting of ICH. The large majority indicated vitamin K (50%), or PCC (27%), or fresh-frozen plasma (14%), while only 2% would use recombinant factor VII. Seven percent claimed that anticoagulation reversal was not a standard emergency department procedure at their institution.
Third, participants were asked when would they administer PCC if a patient with ICH needed urgent neurosurgical intervention. More than half (52%) reported that such patients were never managed in the emergency department (ie, after the diagnosis had been established, patients were always moved to the intensive care unit, or the directly to the operating theater/room). Of the remaining, 46% stated that the right timing for administration was “before” the intervention, 1% “during” intervention, and 1% “after” intervention. Finally, responders were asked to rate the annual incidence of MH and of ICH-related mortality in anticoagulated patients, based on their knowledge of the literature.
Concerning the incidence of MH, 19% of the physicians rated it at 2 to 3 cases per 100 patients, 36% estimated it at 2 to 3 cases per 1000, and 3% at 2 to 3 cases per million. The remaining 42% stated they “had no idea,” or they “did not remember.” As to the incidence of ICH-related death, 7% of the responders rated it at ≤1%; 56% stated they either “had no idea” or “did not remember”, and the remaining valued it at >1%.
Survey—Patterns
The physicians participating to the survey gave, in general, quite consistent answers, irrespective of the geographic location of their institutions (ie: north, center, or south of Italy), with few exceptions. Namely, we were able to observe statistically significant differences between the answers given by physicians based in the North versus those based in the South only regarding 2 questions (Table 2).
Regional Patterns With Statistically Significant Differences.
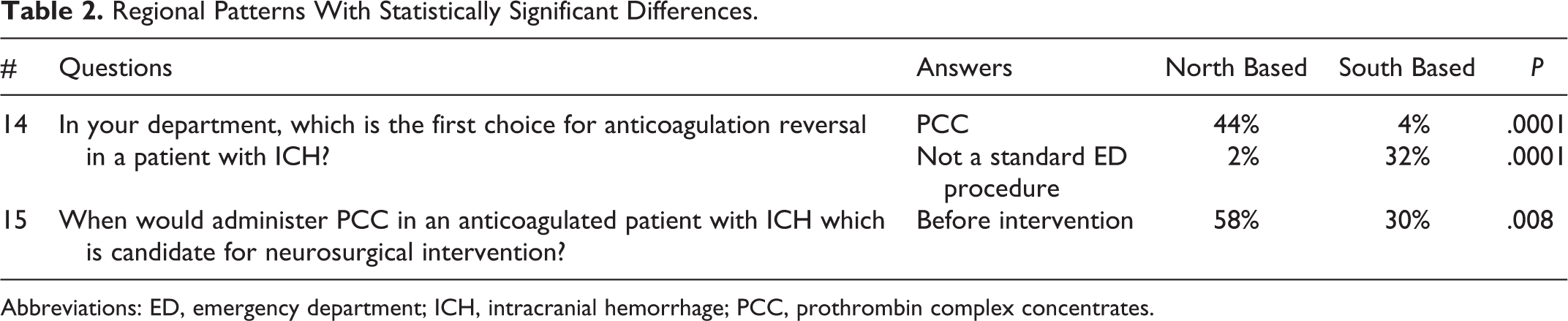
Abbreviations: ED, emergency department; ICH, intracranial hemorrhage; PCC, prothrombin complex concentrates.
Answers to questions 5 to 7 and 13 to 15 (Table 1) were more likely, although not significantly (P = .08), to match international guidelines if physicians worked in institutions with an approved protocol for the management of VKA-induced major bleeding than those employed in hospitals without specific guidelines. Physicians working in hospitals serving a population of ≤150.000 people tended to report more frequently the presence of a protocol for the management of VKA-induced MH, than those employed in larger hospitals (P = .07).
Discussion
Vitamin K antagonists have been on the market for more than 50 years now, being, until recently, the only available resource for the management of several cardiovascular diseases, including prevention of ischemic stroke in patients with atrial fibrillation or myocardial infarction, and long-term treatment of venous thromboembolism. This class of drugs carries well-known drawbacks; in particular, spontaneous or posttraumatic (severe) bleeding events.
It is expected that emergency physicians, facing ongoing or potential (severe) bleeding events in patients treated with VKA almost on a daily basis, should be familiar with recommended strategies for rapid anticoagulation reversal. The present survey performed in 150 Italian emergency departments raises some concern about these assumptions.
Indeed, although recommended by the most recent American College of Chest Physicians guidelines and by the latest Italian guidelines issued by the Federation of the Centers for Anticoagulation, only one-third (29%) of the responders stated they would surely give vitamin K in patients with MHs induced by VKA. 2,8 Similarly, only about one-third (27%) of them indicated PCC as the first choice for anticoagulation reversal in the setting of ICH, and less than 50% of the physicians would administer PCC before neurosurgical intervention, although the use of PCC in this situation is recommended. Of all MH, ICH is a most devastating condition, associated with high morbidity and mortality; and, when occurring in anticoagulated patients, it carries an even worse outcome. Actually, being the mortality rate as high as 40% at 7 days, these patients really necessitate an expedited and relentless anticoagulation reversal. 9 According to the literature, PCC are at least as effective as fresh-frozen plasma at restoring effective hemostasis and significantly more effective at returning INR values toward the normal range, meantime displaying a similar safety profile and avoiding significant fluid overload complications. 10 –15 To the contrary, the preferential use of the more expensive 4-factor PCC instead of 3-factor PCC is still debated, and needs to be further investigated. 16 In this respect, the uncertainty displayed by the responders appears to be justified.
Physicians working in institutions with an approved protocol for the management of VKA-induced major bleeding tended to answer according to current guidelines more than those employed in hospitals without such protocols. Furthermore, physicians working in first-level hospitals (ie, those serving a population of ≤150.000 people) showed a higher awareness about the management of MH, than those employed in higher-level centers, possibly related to the absence of neurosurgeons “in-house.”
Coming to the knowledge of epidemiological data concerning the use of VKA, of importance both for the logistics of the emergency department and for a correct patient counseling, only 1 of the 5 responders (19%; 95% confidence interval [CI] 14%-26%) correctly rated the annual incidence of warfarin-associated MH, which is estimated at 1% to 3%. 17,18 Interestingly, the majority (42%) of physicians simply stated they had “no idea,” or did “not remember” of the data published in the literature. Similarly, only 7% (95% CI 4.0%-13%) of the responders was able to correctly rate the incidence of (fatal) ICH associated with long-term VKA use, which is reported to range between 0.3% and 0.7% per year. 18 –20
In conclusion, the average knowledge of the management strategies for VKA reversal displayed by physicians working in 150 emergency departments, evenly distributed upon the Italian territory, appears to be unsatisfactory. Considering the high mortality/disability burden carried by MH in patients treated with VKA, the need for an extensive educational program, and for the implementation of specific guidelines, possibly endorsed by Scientific Societies, cannot be underemphasized. Ideally, given the availability of new oral anticoagulants (anti-Xa and anti-II selective inhibitors) that are going to rapidly replace VKA for most of their indications, emergency physicians should also be made aware of suitable reversal strategies to be employed in patients treated with those novel drugs.
Footnotes
Acknowledgments
The authors wish to acknowledge DoxaPharma for performing the telephone survey, and for technical support and Doctor Paola Del Bianco (Istituto Oncologico Veneto IRCCS) for statistical advice.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.