
Abstract
This study evaluated the early hemostatic effects of a novel hemostatic agent (Ankaferd blood stopper [ABS]) during dental extractions in patients on antithrombotic therapy, without interruption or diminution of the medication. In total, 25 patients, who are on antithrombotic therapy and in need of simple dental extractions, were randomized into 2 groups. In group I (control group), which consisted of 10 patients, local hemostasis was achieved with direct packing with gauze. In group II, which consisted of 15 patients, local hemostasis was achieved by the local application of ABS on the extraction sockets. The bleeding time was compared between 2 groups following the tooth extraction. The bleeding time in the dental sockets treated with ABS was statistically lower compared to the sockets of the control group (p = 0.0001). It is concluded that the dental extractions could be performed without interruption of the medication in patients on antithrombotic therapy. The ABS appears to be sufficient as an alternative hemostatic agent.
Introduction
Antithrombotic drugs, which can be divided into 3 major categories, anticoagulants, antiplatelets, and thrombolytics, have been broadly researched and developed as a potential therapy in the prevention and management of arterial and venous thrombosis. These drugs have been associated with an increase in the bleeding time and the risk of postoperative hemorrhage. 1 Dental extractions are common procedures in patients who receive oral anticoagulant treatment. In the past, some authors suggested stopping the anticoagulant treatment for several days before the dental extraction, while others suggested reducing the dose of anticoagulant intake for several days before extraction. In recent years, it has been suggested to carry out the extractions without any interruption or diminution of the anticoagulant treatment but with emphasis on the efficiency of the local hemostasis.2,3 Various local hemostatic agents have been used in oral and maxillofacial surgery practice. The hemostatic agents vary depending on the effectiveness, cost, and convenience. The ideal oral surgery hemostatic agent should be safe, well tolerated, bacteriostatic, preformed for operator convenience, packaged, sterile, single-use, remain where applied, dissolve in the first week postsurgery, and integrate without special procedures within current oral surgery treatment protocols. It should also be used in patients taking antithrombotic drugs. No hemostatic device has met these criteria completely. 4
Ankaferd blood stopper (ABS) is a unique medicinal plant extract, which has historically been used in Turkish traditional medicine as a hemostatic agent. The ABS has been approved in the management of external hemorrhage and dental surgery bleedings in Turkey, based on the safety and efficacy reports indicating its sterility and nontoxicity. The ABS comprises a standardized mixture of the plants which are Thymus vulgaris, Glycyrrhiza glabra, Vitis vinifera, Alpinia officinarum, and Urtica dioica. The basic mechanism of the action for ABS is the formation of an encapsulated protein network that provides focal points for vital erythrocyte aggregation. The ABS-induced protein network formation with blood cells particularly erythrocytes covers the primary and secondary hemostatic system without disturbing the individual coagulation factors.5,6
This study was designed to evaluate ABS, an alternative hemostatic agent, and its effects on bleeding time following the dental extractions. To the best of the authors' knowledge, this is the first study which includes the use of ABS in the dental extraction sockets of the patients on antithrombotic therapy, without drug alteration.
Patients and Method
In total, 25 patients, who were on antithrombotic therapy for >1 year, had an international normalized ratio (INR) ≤4.0 and required dental extractions were included for the present study. The study group comprised 15 patients, being 7 female and 8 males with an average age of 56.20 years. The control group comprised 10 patients, being 5 females and 5 males with an average age of 47.60 years.
The patients with a history of chronic renal or liver disease or who were on drugs that could affect liver function or hemostasis, other than warfarin, were excluded. 2 The indications for antithrombotic therapy included valvular heart disease, ischemic heart disease, atrial fibrillation, and venous thromboembolism. Before the commencement of the study, the informed consents were obtained from all the patients who accepted the management and consultations were made with their physicians.
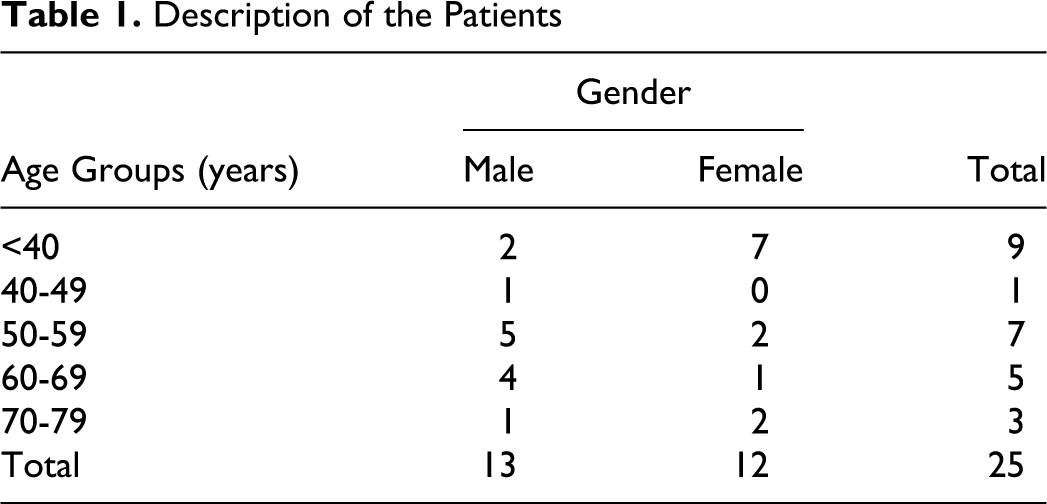
A group of 25 patients (13 males and 12 females), ranging from 26 to 73 years (mean 51 years) underwent 32 dental extractions without any modification of their antithrombotic therapy (Table 1 ).
Description of the Patients
Simple single extraction and multiple (up to 4 elements) simple extractions were considered low-risk interventions. Therefore, the patients in the present study were classified in a low surgical risk group. All the surgical procedures were simple extractions that did not require elevation of a mucoperiosteal flap.
The antithrombotic activity of the associated drugs (aspirin and coumarin) was evaluated by the INR on the date of the procedure. The INR levels, the number of extracted teeth, and postoperative spontaneous bleeding are shown in Table 2 .
Distribution of INR Levels, Number of Teeth Extracted and Postoperative Bleeding in All Groups
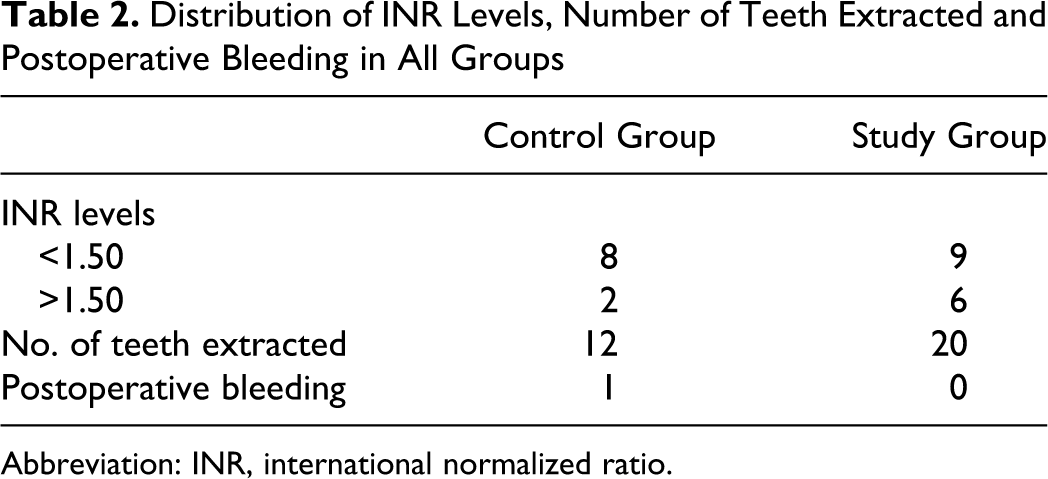
Abbreviation: INR, international normalized ratio.
The patients with cardiac valvular disease received prophylactic antibiotic therapy according to the institutional protocol. The extractions were performed under local anesthesia with 2% mepivacain without any vasoconstructor. No more than 2 carpules were used in each intervention.
Two qualified oral surgeons carried out the extractions using forceps and/or elevator. The extractions were carried out in the least traumatic way possible and the extraction sites were carefully removed. In group I (control group), local hemostasis was achieved with direct packing with gauze. In group II (ABS-treated group), local hemostasis was achieved within the local application of ABS on the extraction sockets. The ABS was topically applied by homogeneously spraying with a high pressure into the cavity.
The patients were given a list of postoperative instructions. On the day of surgery, the patients were followed-up for hemorrhage during the 2 hours after the extractions. The appointments for the next control have been made for 1, 3, and 7 days after the surgery.
Statistical Analysis
The statistical analysis was presented with Number Cruncher Statistical Systems (NCSS) 2007. Mann-Whitney U test was used to evaluate descriptive statistical methods (mean and standard deviation) and also the differences between the groups. Chi-square test was applied for nonparametric comparisons. It is used for the comparisons of the quantitative data, including the gender and bleeding time ≤1 minute and >1 minute, in control and study groups. P < 0.05 was considered statistically significant.
Results
Twenty-five antithrombotic-medicated patients (15 in study group and 10 in control group) were enrolled in the study. There was no statistically significant difference between the gender and age of the groups regarding the bleeding time (Table 3 ).
The Demographic Comparison of the Control and Study Groups
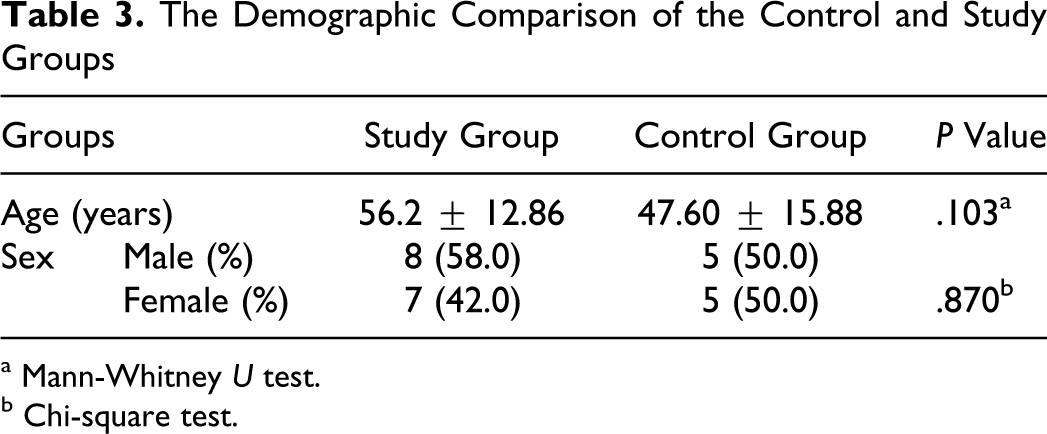
a Mann-Whitney U test.
b Chi-square test.
The most significant clinical difference between the groups was associated with the use of ABS. A protein network formation was observed immediately after the application of the agent, in all dental extraction sockets treated with ABS.
The highest levels of INR in groups I and II were 2.10 and 2.55, respectively. There was no statistically significant difference regarding the INR level in the operation day between the groups (Table 4 ).
Comparison of Control and Study Groups Regarding the Levels of INR and Bleeding Time
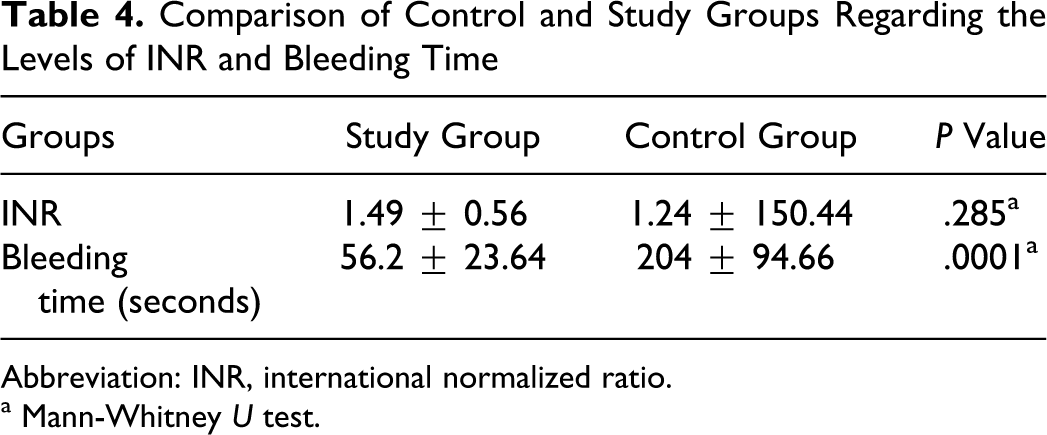
Abbreviation: INR, international normalized ratio.
a Mann-Whitney U test.
The criteria used to compare the treatment groups were local hemostasis and late bleeding. In this point, complete hemostasis was immediately obtained from 2 groups, except 1 patient from the study group. In the study group, the patients were administered 1 to 2 mL of ABS. One milliliter of ABS was enough for most of the patients to control bleeding. One patient from the study group, who was on coumarin and aspirin therapy with an INR level of 2.38, experienced immediate postoperative bleeding. A secondary dose of ABS was applied in the extraction socket. The bleeding time was 100 seconds for this patient.
The mean of the bleeding time in group I was measured as 204 seconds, while it was 56.2 seconds in group II. The bleeding time in group II was found statistically lower than the group I (Table 4). On average, 66.7% of the ABS-treated dental extraction sockets achieved hemostasis in ≤1 minute, and 80% of the nontreated sockets achieved hemostasis longer than 1 minute.
Late bleeding was only observed at the first day after the surgery in a patient from the control group. The patient was on coumarin therapy with an INR level of 2.10. The bleeding time was 30 minutes, and therefore 1 unit of plasma was given to the patient.
No wound infection associated with the extraction sockets was observed at the last appointment.
Discussion
In the past, stopping anticoagulant treatment for 2 to 6 days before dental extractions was suggested as severe hemorrhage may occur postoperatively. 7 In recent years, it has been suggested to carry out the extractions without any interruption or diminution of the anticoagulant treatment but with an emphasis on the efficiency of the local hemostasis. 8 Various hemostatic agents (oxidized cellulose, gelatin sponge, fibrin glue, bone wax, fibrin glue, and tranexamic acid) have been used in order to maintain local hemostasis. 9 A retrospective study showed that there is no marked difference in local hemostasis among oxidized cellulose, gelatin sponge, and fibrin glue, for tooth extraction in patients on oral antithrombotic therapy. 10 Blinder et al compared 3 local measures, including gelatin sponge, sutures, and tranexamic acid for controlling bleeding on 150 patients undergoing 359 extractions with INR values ranging from 1.5 to 4.0. The results showed that 13 patients presented postoperative bleeding, which were equally distributed among the 3 groups. No statistically significant difference was found among the groups regarding the incidence of postoperative bleeding. 3
Malmquist et al evaluated the efficacy of the hemostatic oral wound dressing (HemCon Dental Dressing) and whether the early hemostasis affects postoperative care and surgical healing outcomes following the oral surgical procedures. They reported that all patients taking oral anticoagulation therapy achieved hemostasis within 1 minute and were treated without altering their anticoagulant regimens. 4 Baykul et al investigated the efficacy of the topical application of ABS in 4 patients on hemorrhagic diathesis, following dental procedures under different conditions. The ABS was found to be effective within 10 to 20 minutes in controlling bleeding in most of the patients after dental surgery. 11 In the present study, we used ABS as an effective and safe alternative hemostatic agent. Only 2 patients had postoperative bleeding that was stopped with the reuse of ABS. It is shown that the mean of the bleeding time in ABS-treated dental extraction sockets was 56.2 seconds. On the other hand, further studies are required in order to compare its effects with the other hemostatic agents.
Isler et al reported that the application of ABS decreased the occurrence of inflammation and necrosis, while increasing new bone formation in early bone healing period in bone defects of rats. In the present study, there was no clinically obvious difference between the groups regarding the healing of the extraction sites. 6
In this study, there was no correlation between the appearance of postoperative bleeding and the value of the INR measured on the day of extraction as reported by Blinder et al. 12
Within the limit of this study, it is thought that ABS is effective, safe, quick, and easy to use. Another advantage is associated with the mechanism of action. Blood stopping process is driven by protein agglutination. The ABS stimulates the formation of an encapsulated protein network that provides spaces for erythrocyte aggregation in the injured vascular area. Furthermore, ABS also interacts with fibrinogen as well as other blood proteins. The ABS-induced formation of the protein network affected the entire physiological hemostatic process without affecting any individual clotting factor. The levels of coagulation factors II, V, VII, VIII, IX, X, XI, and XIII were not affected by ABS. Therefore, it might be used in patients with deficient primary hemostasis and/or secondary hemostasis, including the patients with disseminated intravascular coagulation. 5
It is important to emphasize that there are currently no reported side effects after ABS application in the literature, possibly due to its natural ingredients, except the metallic taste in the mouth lasting to approximately 5 minutes as reported in the present study. 5
Conclusion
This study suggests that the ABS significantly shortens bleeding time and appears to be sufficient as a hemostatic agent for the management of patients on antithrombotic therapy and who have an INR ≤4.0, without interruption or diminution of the medication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.