
Abstract
Objective:
Reduced effect of antiplatelet therapy following coronary artery bypass grafting is associated with reduced graft patency. We sought to evaluate the impact of hybrid coronary revascularization on the effect of aspirin and clopidogrel and whether high baseline platelet aggregation, high postoperative levels of platelet turnover, and acute-phase response may contribute to the effect.
Methods:
We prospectively studied platelet aggregation (VerifyNow and Multiplate Analyzer), platelet turnover (immature platelets, mean platelet volume, and thrombopoietin), and acute-phase reactants (C-reactive protein, von Willebrand factor, and coagulation factor VIII) in 40 patients undergoing elective hybrid coronary revascularization (off-pump surgical revascularization through J-hemisternotomy followed by percutaneous coronary intervention [PCI]). Preoperative blood samples on- and off-aspirin were compared with blood samples obtained postoperatively, following PCI when dual antiplatelet therapy had been initiated and at 1-year follow-up.
Results:
The antiplatelet effect of aspirin was significantly reduced in the early postoperative period as measured by VerifyNow Aspirin but not by Multiplate ASPI test. The antiplatelet effect of clopidogrel was significantly reduced following PCI as measured by VerifyNow P2Y12 and Multiplate ADP test. The level of baseline aggregation did not predict the antiplatelet effect of aspirin or clopidogrel, and no association was found between platelet aggregation and postoperative platelet turnover or acute-phase reaction.
Conclusions:
A transient reduction in the antiplatelet effect of aspirin and clopidogrel was observed after hybrid coronary revascularization despite limited surgical trauma and off-pump technique. Neither baseline platelet aggregation nor postoperatively increased platelet turnover and acute-phase response could explain this finding. ClinicalTrials.gov identifier, NCT02293928.
Introduction
Low-dose aspirin is recommended early after coronary artery bypass graft surgery (CABG) to prevent graft occlusion. 1 However, the effect of aspirin on myocardial infarction, stroke, and death is significantly reduced among patients who recently underwent CABG compared to patients with stable coronary artery disease. 2 Several laboratory investigations have shown a transient reduction in the antiplatelet effect of aspirin during the first weeks following on-pump CABG. 3 –6 Evidence is conflicting regarding the antiplatelet effect of aspirin following off-pump CABG. 7 –11 Reduced antiplatelet effect of aspirin has been shown to be associated with an increased vein graft occlusion rate following on- and off-pump CABG. 11,12
Hybrid coronary revascularization combining minimally invasive off-pump CABG and percutaneous coronary intervention (PCI) is increasingly used to minimize the surgical trauma and prevent periprocedural complications. Dual antiplatelet therapy is recommended following hybrid coronary revascularization with implantation of stents to prevent stent thrombosis. 13 The impact of hybrid coronary revascularization on the antiplatelet effect of aspirin and clopidogrel has not yet been investigated.
The suggested mechanisms explaining a reduced effect of oral antiplatelet therapy are manifold. 14 The inhibitory effect of aspirin on platelet aggregation is based on irreversible inhibition of cyclooxygenase leading to blockage of thromboxane production. Clopidogrel exerts its antiplatelet effect by blocking the P2Y12 receptor, which is the major receptor to amplify and sustain platelet activation in response to adenosine diphosphate. Recently, the occurrence of increased platelet turnover has attracted particular attention, as it may cause a reduced antiplatelet effect of aspirin and clopidogrel. 15 –19 Immature platelets contain messenger RNA enabling de novo synthesis of cyclooxygenase 1 and other hemostatic proteins. 16 Moreover, newly formed platelets express more cyclooxygenase 2, which is largely unaffected by low-dose aspirin. 16 This theory is substantiated by the fact that increased mean platelet volume (MPV), which is another marker of thrombopoiesis, is associated with prothrombotic and proinflammatory conditions. 20
Inflammation may be another contributor to reduced effect of antiplatelet agents. 14 Increased levels of C-reactive protein have been linked with reduced antiplatelet effect of aspirin in patients with stable coronary artery disease. 21 Furthermore, levels of C-reactive protein and von Willebrand factor antigen are increased shortly after CABG. 10,22,23
We hypothesized that hybrid coronary revascularization is associated with a transiently reduced antiplatelet effect of aspirin and clopidogrel. Furthermore, we hypothesized that the reduced antiplatelet effect of aspirin and clopidogrel could be explained by increased platelet turnover and increased inflammatory markers in the early postoperative phase. Thus, the aims of our study were to investigate (1) the impact of hybrid coronary revascularization on the antiplatelet effect of aspirin and clopidogrel, (2) the influence of baseline platelet aggregation on the postoperative antiplatelet effect of aspirin and clopidogrel, and (3) to what extent platelet turnover and the postoperative acute-phase response were associated with the antiplatelet effect of aspirin and clopidogrel.
Material and Method
Study Population
A total of 40 patients with coronary artery disease were included in this prospective cohort study between October 2010 and April 2012. The study cohort was recruited from a prospective pilot study (n = 100) conducted to assess feasibility and safety of elective hybrid coronary revascularization combining minimally invasive off-pump CABG and PCI (ClinicalTrials.gov identifier: NCT01496664). 24 Criteria for inclusion in the present prespecified substudy were age ≥18 years, symptomatic multivessel coronary artery disease, and treatment with nonenteric-coated aspirin 75 mg once daily. Exclusion criteria were aspirin or clopidogrel allergy or intolerance, conditions prohibitive of aspirin discontinuation prior to surgery (eg, acute coronary syndrome or critical stenoses), use of anticoagulants or any drugs other than aspirin known to affect platelet function, use of immunosuppressive drugs, platelet count <100 or >450 × 109/L, and inability to give informed consent. The predicted mortality was assessed by means of the logistic European System for Cardiac Operative Risk Evaluation (EuroSCORE) I. 25
Written informed consent was obtained from all patients. The study conformed to the principles outlined in the Declaration of Helsinki and was approved by the Central Denmark Region Committee on Biomedical Research Ethics (Project ID M-20100151).
Study Design
All patients were treated with nonenteric-coated aspirin 75 mg once daily prior to study participation. Aspirin treatment was discontinued 8 to 10 days prior to surgery and resumed 6 to 9 hours after surgery. Left internal mammary grafting of the left descendent coronary artery was performed off-pump through an inferior J-hemisternotomy (JOPCAB). Anesthesia was induced and maintained using propofol, sufentanyl, and rocuronium. All patients received prophylactic tranexamic acid perioperatively (2 g at induction and 1 g at completion of surgery). Unfractionated heparin 300 IU/kg was administered during harvest of the mammary artery, and additional boluses were given as required to maintain an activated clotting time >400 seconds. After completion of the anastomosis, heparin was neutralized with protamine sulfate. All patients received an oral loading dose of aspirin 300 mg 6 to 9 hours after surgery followed by daily maintenance doses of 75 mg aspirin. An oral loading dose of clopidogrel 300 mg 12 hours prior to PCI was followed by daily maintenance doses of 75 mg for 12 months. Subcutaneous dalteparin 5000 IU was given twice daily from first postoperative day until the day before PCI to prevent deep venous thrombosis. Prior to PCI, unfractionated heparin was given to achieve an activated clotting time >250 seconds. We recorded adverse cardiovascular events during 1-year follow-up (graft dysfunction, myocardial infarction, stroke, and pulmonary embolism).
Six blood samples were obtained from each patient: the first in the outpatient setting while patients were on aspirin 75 mg daily (Pre-OP), the second in the morning prior to surgery after 8 to 10 days of aspirin discontinuation (baseline; off-aspirin), the third on the first postoperative day when aspirin had been resumed (Post-OP), the fourth on the day prior to PCI (Pre-PCI), the fifth on the first day after PCI following initiation of dual antiplatelet therapy (Post-PCI), and the sixth at 1-year follow-up when patients were still on maintenance aspirin 75 mg and clopidogrel 75 mg (1-year follow-up). The timing of intervention and blood sampling is outlined in Figure 1. All postoperative samples were drawn in the morning prior to ingestion of antiplatelet medication.
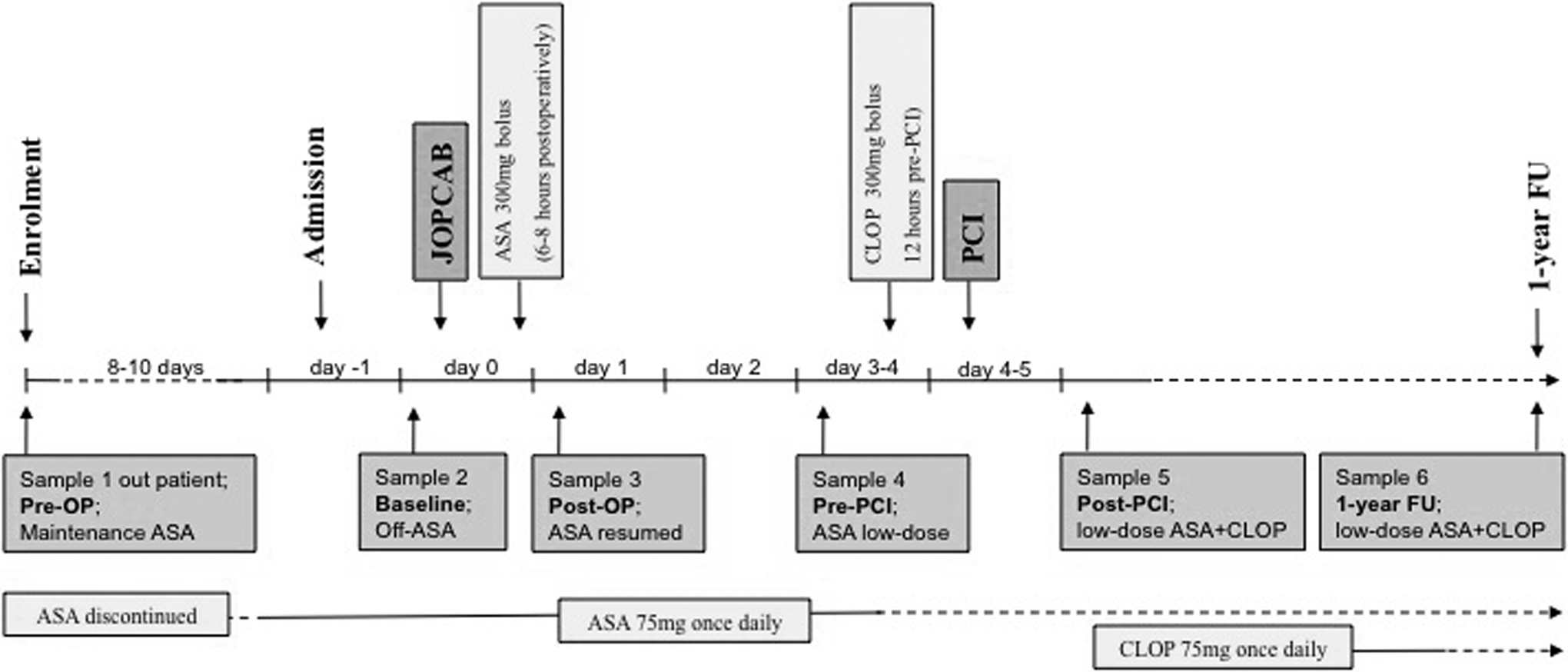
Study design including timing of intervention and blood sampling.
Laboratory Measurements
Standardized blood sampling was performed between 7
Platelet function analyses were performed in whole blood within 2 hours of sampling using Multiplate Analyzer, VerifyNow Aspirin, and VerifyNow P2Y12. For VerifyNow, the intra-assay coefficient of variation was ≤1% and the interassay coefficient of variation was ≤3%. 26 For Multiplate Analyzer, arachidonic acid (1.0 mmol/L) and adenosine diphosphate (6.4 and 20 μmol/L) were used as agonists. Intra- and interassay variability for Multiplate Analyzer were ≤12% and ≤ 23%, respectively. 26 Multiplate Analyzer results are expressed as area under the aggregation curve (aggregation units × minute). VerifyNow test results are expressed as aspirin reaction units or P2Y12 reaction units.
Blood samples for hematological analyses were analyzed within 90 minutes of sampling. Complete blood counts, including immature platelet fraction (IPF), immature platelet count (IPC), and MPV, were performed using a Sysmex XE-5000 hematology analyzer (Sysmex, Kobe, Japan) with upgraded software (XE IPF Master; Sysmex), enabling flow cytometric detection of the IPF as described previously. 27 Intra- and interassay coefficients of variation for MPV measurement were <5% and <8%, respectively. For platelet count, intra- and interassay coefficients of variation were <10%.
Enzyme-linked immunosorbent assays were used according to the manufacturers’ instructions to measure serum thromboxane B2 (Cayman Chemical, Ann Arbor, Michigan) and thrombopoietin (R&D Systems Europe, Abingdon, United Kingdom). Intra- and interassay coefficients of variation were ≤20% for thromboxane B2 and <3% and <7% for thrombopoietin.
Plasma C-reactive protein was measured by immunoprecipitation using the Cobas 6000 (Roche, Basel, Switzerland). Coefficient of variation was <8%. Von Willebrand factor (antigen) and coagulation factor VIII (functional) were measured using the ACL TOP (ILS Laboratories, Bedford, Massachusetts). For von Willebrand factor (antigen), the intra- and interassay coefficients of variation were <3%, and for coagulation factor VIII (functional), the intra- and interassay variation was <10%.
Statistical Analysis
Since most data were nonnormally distributed, continuous variables are presented as medians and range, and dichotomous variables as numbers and percentages. Comparisons of continuous paired variables between the 2 groups were performed with the Wilcoxon signed-rank test. Analyses of repeated measurements across more than 2 time points were performed using Friedman’s test for repeated measures. Spearman’s ρ coefficient was calculated for bivariate analyses. Multiple linear regression analyses (including age, gender, body mass index, smoking, diabetes, and platelet count) were used to identify independent preoperative determinants of platelet aggregation. Two-sided P values <.05 were considered significant. Statistical analyses were performed in Stata version 12.1 for Windows (StataCorp, College Station, Texas), and graphs were made in GraphPad Prism version 6 for Windows (GraphPad Software, Inc, La Jolla, California).
Results
Baseline characteristics of the study population are shown in Table 1. The study population had a low-risk profile with a large proportion of patients with stable coronary artery disease and a low predicted mortality, as reflected by the EuroSCORE I. No events of death, stroke, or pulmonary embolism were observed during 1-year follow-up. The PCI-related myocardial infarction was diagnosed in 1 patient.
Baseline Characteristics of Study Population.
Abbreviations: CABG, coronary artery bypass grafting; CAD, coronary artery disease; EuroSCORE I, European System for Cardiac Operative Risk Evaluation (logistic EuroSCORE, range 0%-100%) 24 , PCI, percutaneous coronary intervention; IQR, interquartile range.
aData are presented as medians (IQR).
bData are presented as numbers (%).
cFirst-degree relatives with onset of ischemic heart disease before the age of 60 years.
At enrollment and at 1-year follow-up, all patients were compliant with aspirin as confirmed by levels of serum thromboxane B2 below 30 ng/mL, which corresponds to more than 95% inhibition of platelet cyclooxygenase 1 activity. 28 At enrollment (Pre-OP), median serum thromboxane B2 levels were 2.86, range 0.36 to 28.4 ng/mL. At 1-year follow-up, median serum thromboxane B2 levels were 1.85, range 0.40 to 17.7 ng/mL.
Platelet Aggregation
Figures 2 and 3 show the time-related platelet aggregation pre- and posttreatment. According to VerifyNow Aspirin, platelet aggregation was significantly increased postoperatively (Post-OP, Pre-PCI, and Post-PCI) when compared to Pre-OP (all P values below .003) and 1-year follow-up (all P values below .03). No significant change in cyclooxygenase-dependent platelet aggregation was found with Multiplate Analyzer when using arachidonic acid as the agonist. Both platelet function tests showed significantly increased levels of P2Y12-receptor-dependent platelet aggregation Post-PCI when compared to 1-year follow-up (all P values below .03).
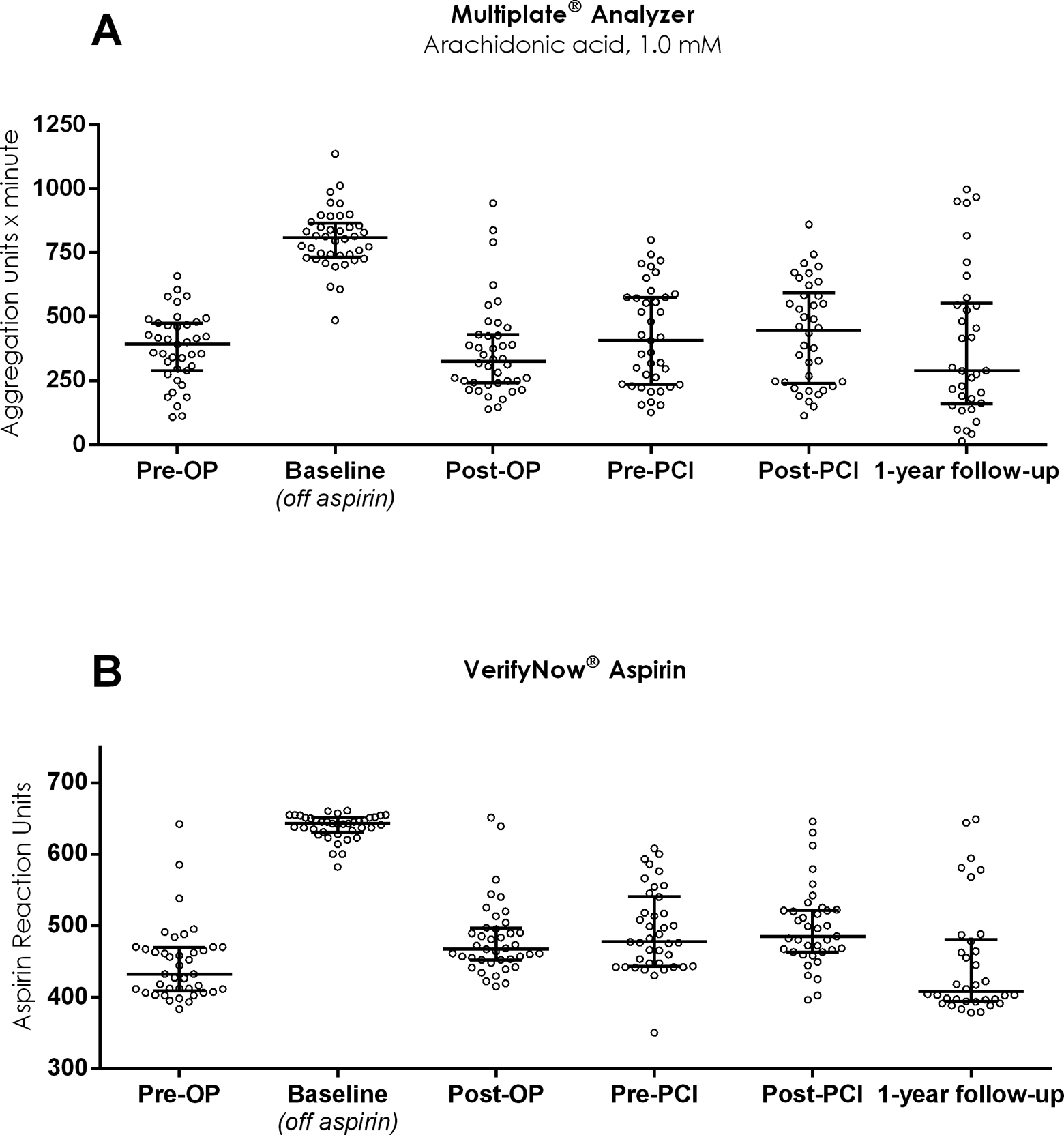
Cyclooxygenase-dependent platelet aggregation evaluated before and after hybrid coronary revascularization using Multiplate Analyzer, arachidonic acid 1.0 mmol/L (A), and VerifyNow Aspirin (B).
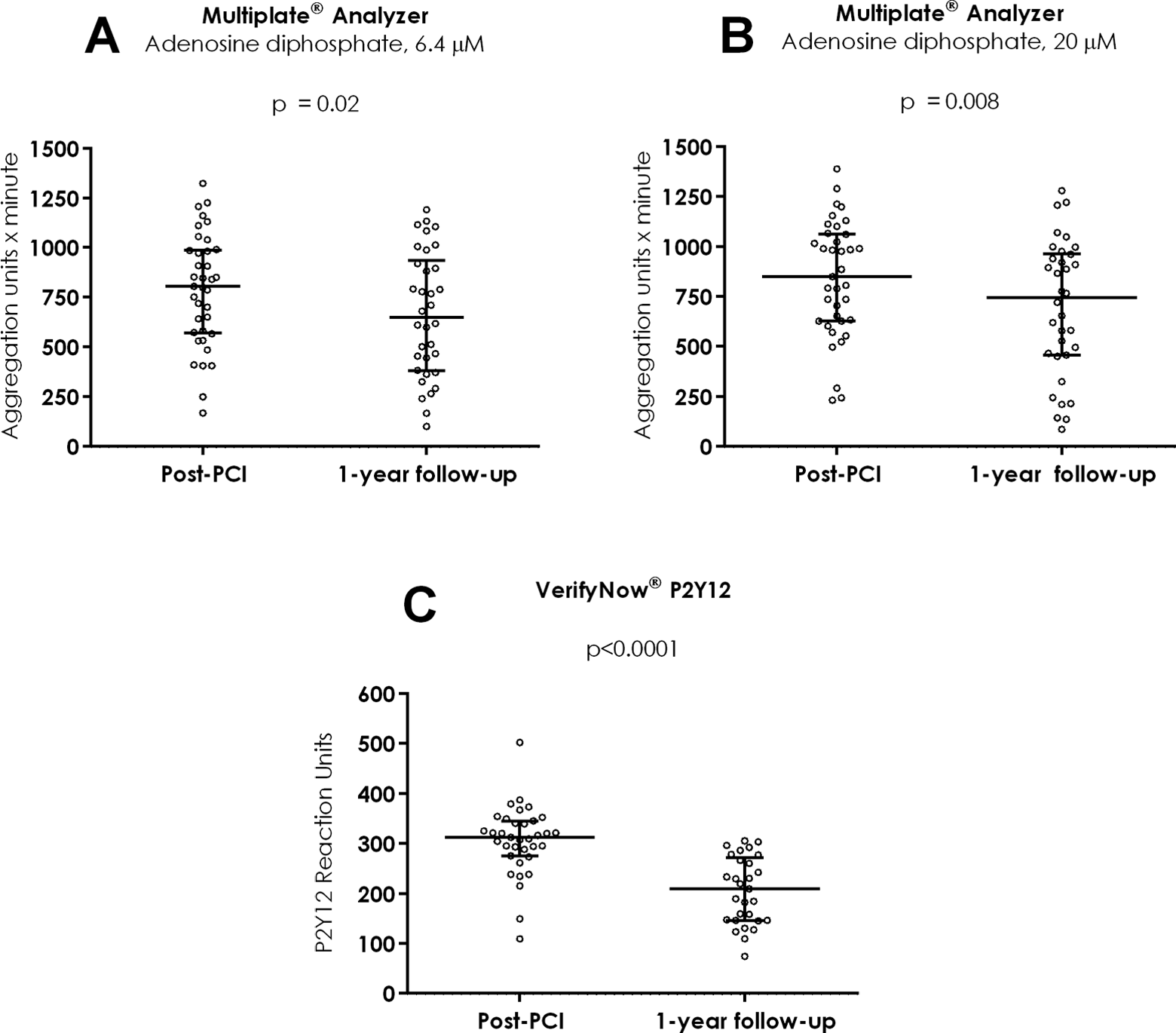
P2Y12 receptor-dependent platelet aggregation evaluated after hybrid coronary revascularization and at 1-year follow-up using Multiplate Analyzer adenosine diphosphate 6.4 μmol/L (A), Multiplate Analyzer adenosine diphosphate 20 μmol/L (B), and VerifyNow P2Y12 (C).
In multiple linear regression analysis, baseline platelet aggregation (off-aspirin) as measured by VerifyNow Aspirin and Multiplate Analyzer was not found to be an independent predictor of the level of platelet aggregation, Pre-OP (on maintenance aspirin treatment), or Post-OP (when aspirin was resumed; all P values >.40).
Platelet Turnover
Figure 4 shows the time-related platelet turnover indices. Both IPF and MPV did not change during the early postoperative period but decreased significantly from Pre-PCI to Post-PCI (IPC: P = .03; MPV: P < .0001) and increased significantly from Post-PCI to 1-year follow-up (IPC: P = .001; MPV: P = .0001). We observed a significant decrease in platelet count and IPC from Pre-OP to Post-OP: Platelet count median 231 [range 165-361] versus 183 [102 to 302] × 109/L, P < .0001; IPC median 4.9 [range 2.7-8.8] versus 4.6 [2.8-8.8] × 109/L, P = .009). Hemoglobin levels decreased significantly from baseline to Post-OP (median 8.8 [range 7.1-9.9] vs 7.5 [5.4-8.9] mmol/L, P < .0001). A significant increase in platelet count from Post-OP to Post-PCI (183 [range 102-302] vs 259 [118-461] × 109/L, P < .0001) was accompanied by an increase in thrombopoietin (median 97 [range 13-456] vs 249 [range 92-999] ng/mL, P < .0001). Changes in thrombopoietin and platelet turnover indices did not correlate with the corresponding changes in platelet aggregation (all P values >.10).
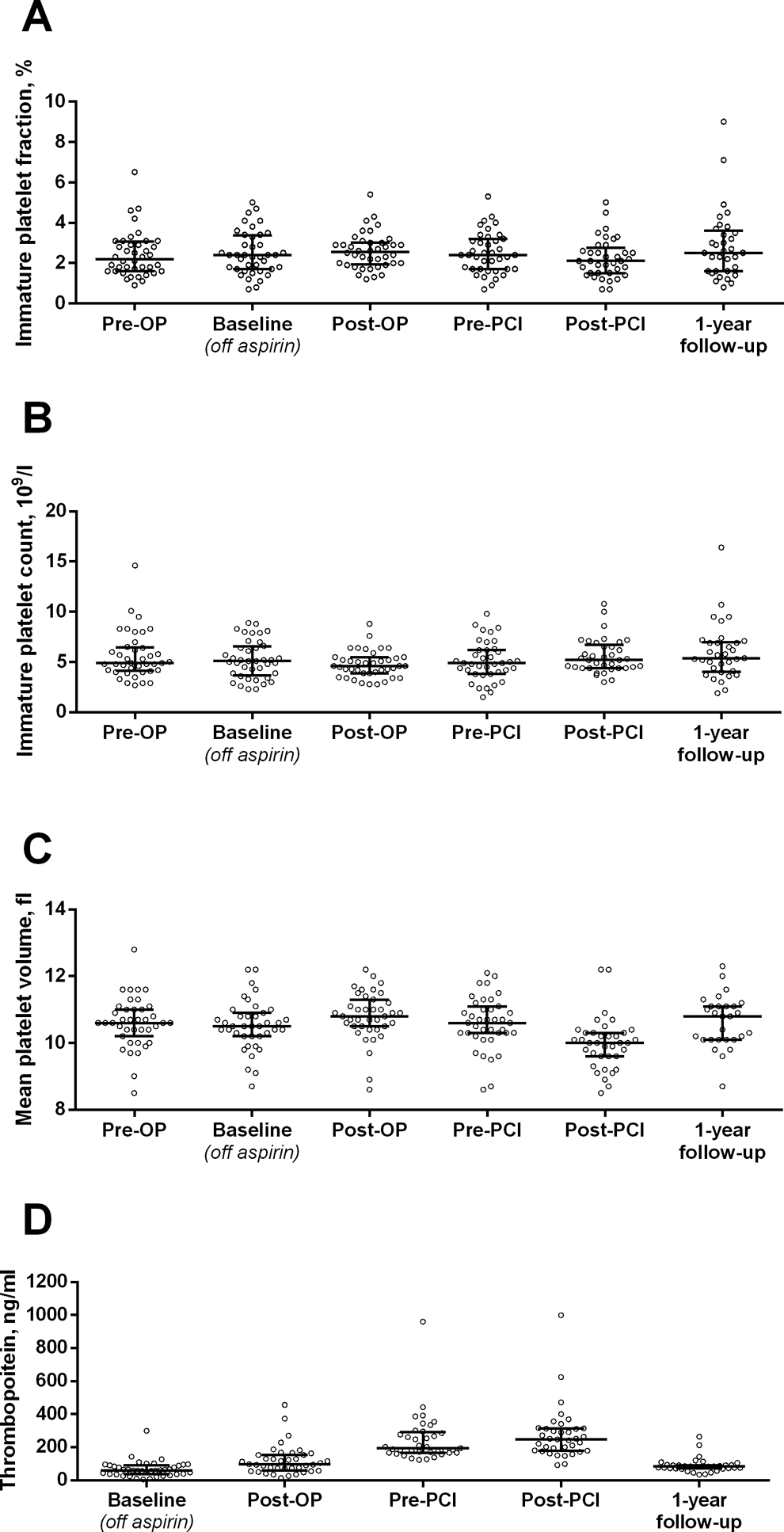
Platelet turnover before and after hybrid coronary revascularization evaluated by immature platelet fraction (A), immature platelet count (B), mean platelet volume (C), and thrombopoietin (D).
Acute-Phase Response
Acute-phase reactants are presented in Figure 5. C-reactive protein, von Willebrand factor (antigen), and coagulation factor VIII (functional) were all significantly increased during the entire postoperative period (Post-OP, Pre-PCI, and Post-PCI) when compared to baseline (all P values below .0001) and 1-year follow-up (all P values below .03). The perioperative changes in levels of the acute-phase reactants did not correlate with the corresponding changes in platelet aggregation (all P values >.10).
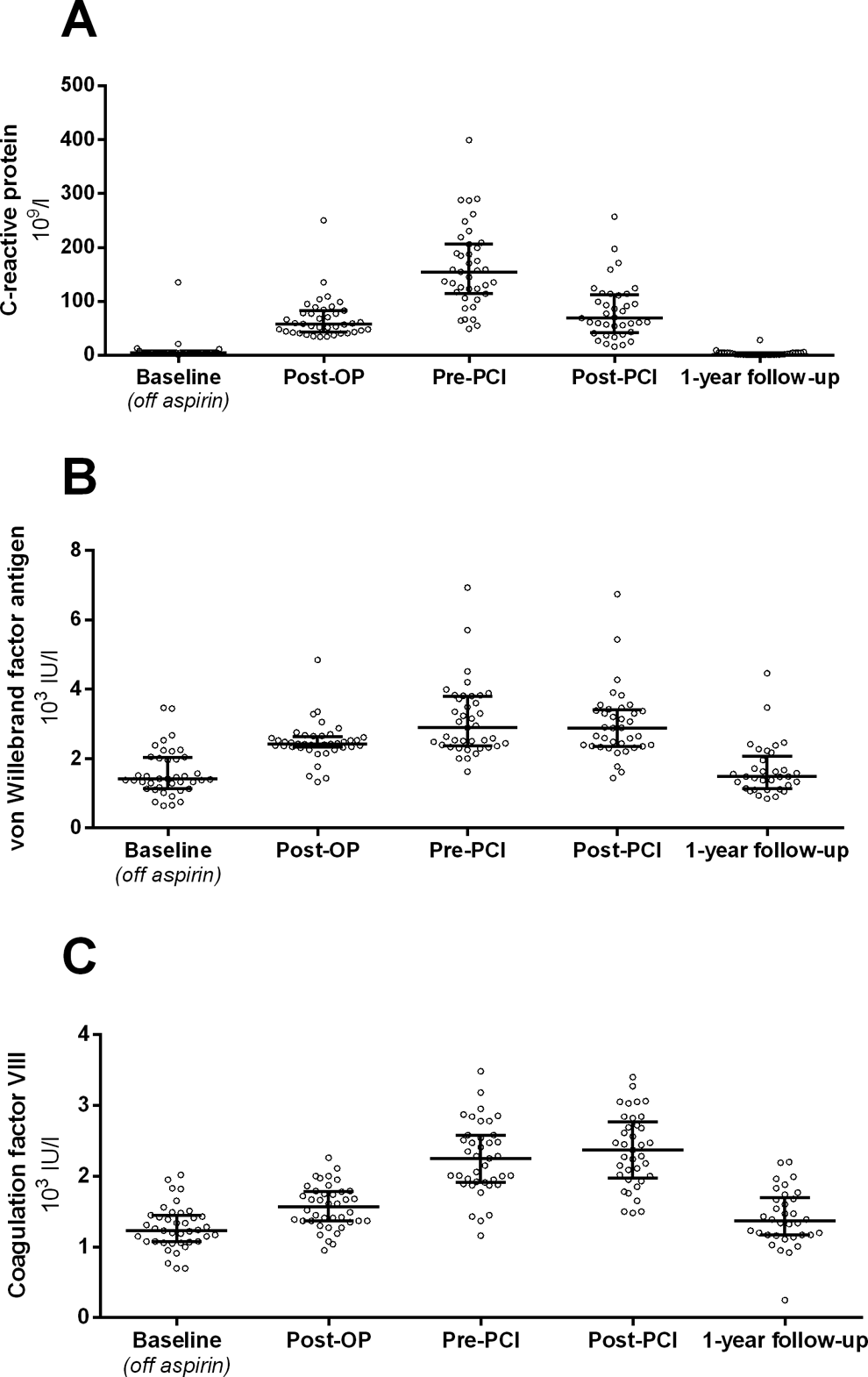
Levels of acute-phase reactants before and after hybrid coronary revascularization evaluated by C-reactive protein (A), von Willebrand factor (antigen; B), and coagulation factor VIII (functional; C).
Discussion
Our study showed that the antiplatelet effect of aspirin and clopidogrel was significantly reduced following hybrid coronary revascularization. Thus, the present study provides evidence that a transient reduction in the effect of antiplatelet therapy emerges, despite efforts to minimize surgical trauma and avoidance of cardiopulmonary bypass. As expected, platelet turnover and acute-phase reactants were increased following hybrid coronary revascularization, but these changes were not associated with the corresponding changes in platelet aggregation. Baseline platelet aggregation did not predict the antiplatelet effect of aspirin and clopidogrel.
A reduced antiplatelet effect of aspirin in the early postoperative period could not be confirmed using Multiplate Analyzer. The susceptibility of Multiplate Analyzer to changes in platelet count and red blood cell count in the early postoperative setting may partly explain this finding. 19,29 Currently, individual tailoring of antiplatelet therapy according to point-of-care platelet function tests after CABG is advocated to reduce graft failure rates. 30 The applicability of Multiplate Analyzer in the early postoperative phase may be limited. Our results are consistent with those of a recent study, in which VerifyNow Aspirin was the most reproducible method and showed the strongest correlation with arachidonic acid-induced light transmission aggregometry. 26
Our hypothesis, enhanced regeneration of platelets could explain a reduced antiplatelet effect of aspirin and clopidogrel following hybrid coronary revascularization, could not be confirmed. We observed no correlation between the increase in platelet turnover indices (IPF, IPC, and MPV) and the corresponding changes in platelet aggregation whether measured by VerifyNow or Multiplate Analyzer. Likewise, platelet aggregation did not correlate with changes in thrombopoietin or platelet count. Thus, none of the parameters reflecting platelet turnover were associated with the reduced antiplatelet effect of aspirin and clopidogrel following hybrid coronary revascularization. Noteworthy, a significant increase in thrombopoietin levels during the early postoperative period preceded the rebound recovery of platelet count without associated increases in IPF, IPC, or MPV. Prior studies have identified immature platelets to reflect the extent of thrombopoiesis in the diseased bone marrow. 27,31 In the present study, levels of IPF, IPC, and MPV were within the normal range, 27,32 and all patients displayed normal platelet counts prior to the intervention. The postoperative decrease in IPC was accompanied by a decrease in total platelet count. This observation is consistent with previous studies showing a substantial reduction in platelet count following on- and off-pump CABG, which is likely related to the extent of perioperative hemodilution. 10,22
We hypothesized that a postoperative acute-phase response could explain the reduced antiplatelet effect of aspirin and clopidogrel following hybrid coronary revascularization. However, we found no association between any of the acute-phase reactants and platelet aggregation levels following hybrid coronary revascularization. This seems to contrast a recent study on stable coronary artery disease, in which the inflammatory markers high-sensitive C-reactive protein and leukocytes were increased in patients with increased on-aspirin platelet reactivity. 21
As none of our hypotheses to explain a transiently reduced effect of antiplatelet therapy following hybrid coronary revascularization were confirmed, other explanatory mechanisms should be considered. The loading doses of aspirin or clopidogrel may prove inadequate due to impaired gastrointestinal absorption in the early postoperative phase, but no data regarding oral absorption of antiplatelet drugs following cardiac surgery are available. Another contributing factor may be the perioperative use of pharmacologic agents known to affect platelet aggregation. In accordance with current recommendations, all patients received antifibrinolytic tranexamic acid to reduce postoperative blood loss. Tranexamic acid has been shown to preserve platelet aggregation following cardiopulmonary bypass in the absence of any anticoagulant therapy. 33 Furthermore, tranexamic acid has been shown to partially reverse the effect of dual antiplatelet therapy on arachidonic acid-induced and adenosine diphosphate-induced platelet aggregation. 34 Thus, the inconsistent use of tranexamic acid in prior studies may contribute to the conflicting reports regarding the prevalence and degree of reduced aspirin response following CABG. In addition, some patients have been anesthetized with propofol, and conflicting evidence exists as to whether propofol enhances platelet aggregation. 35,36
A limitation of our study was the relatively small sample size recruited over a period of 19 months. It was a consequence of the strict inclusion requirements. Timing of blood sampling was defined precisely, and we assessed platelet aggregation both prior to the intervention (Pre-OP; on maintenance aspirin) and after aspirin discontinuation (baseline; off-aspirin). The individual variability in the antiplatelet effect of aspirin and clopidogrel was taken into account as patients served as their own controls. Off-aspirin baseline values were measured to eliminate the risk of overestimating the antiplatelet effect of aspirin. Compliance with aspirin was confirmed in all patients by suppressed levels of thromboxane B2 prior to intervention and at 1-year follow-up. Finally, no platelet concentrate transfusion could interfere with the results. Consequently, interpretation of our data based on a relatively small sample size was legitimated by the highly homogeneous study population exposed to a well-defined intervention.
Another limitation of our study was that we were not able to measure the active metabolite of clopidogrel or to gather reference values of platelet aggregation on clopidogrel maintenance therapy.
In conclusion, the effect of antiplatelet therapy is transiently reduced following hybrid coronary revascularization despite minimized surgical trauma and avoidance of cardiopulmonary bypass. In this study, the surgical intervention stimulated an increase in platelet turnover and acute-phase reactants, but none of these changes explained the reduced antiplatelet effect of aspirin or clopidogrel.
Footnotes
Acknowledgments
We wish to thank research nurse Vibeke Laursen, research secretary Helle Bargsteen and laboratory technicians Vivi Bo Mogensen, and Mai Stenulm Therkelsen for their invaluable support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Danish Heart Foundation (R78-A2911-22606 to SDK) and the Aase and Ejnar Danielsen’s Foundation (10-000439).