
Abstract
Ruptured abdominal aortic aneurysm (AAA) is associated with a high mortality despite surgical management. Earlier reports indicate that a major cause of immediate intraoperative death in patients with ruptured AAA is related to hemorrhage due to coagulopathy. Acidosis is, besides hypothermia and hemodilution, a possible cause of coagulopathy. The aim of the present study was to investigate the incidence of coagulopathy and acidosis preoperatively in patients with ruptured AAA in relation to the clinical outcome with special regard to the influence of shock. For this purpose, 95 consecutive patients who underwent surgery for AAA (43 ruptured with shock, 12 ruptured without shock, and 40 nonruptured) were included. Coagulopathy was defined as prothrombin time (international normalized ratio [INR]) ≥1.5 and acidosis was defined as base deficit ≥6 mmol/L. Mortality and postoperative complications were recorded. The present study shows a state of acidosis at the start of surgery in 30 of 55 patients with ruptured AAA. However, only in 7 of 55 patients with ruptured AAA a state of preoperative coagulopathy was demonstrated. Furthermore, in our patients with shock due to ruptured AAA only 2 of 12 deaths were due to coagulopathy and bleeding. Indeed, our results show a relatively high incidence of thrombosis-related causes of death in patients with ruptured AAA, indicating a relation to an activated coagulation in these patients. These findings indicate that modern emergency management of ruptured AAA has improved in the attempt to prevent fatal coagulopathy.
Introduction
Despite advances in surgical and anesthetic techniques the perioperative mortality remains high in patients with clinical shock due to a ruptured abdominal aortic aneurysm (AAA). 1 The major cause of immediate intraoperative death in patients with ruptured AAA is related to hemorrhage associated with coagulopathy according to earlier reports. 2 Acidosis is, besides hypothermia and hemodilution, a possible cause of coagulopathy. 3 In a recent report, Brohi et al found that early traumatic coagulopathy only occurs in the presence of tissue hypoperfusion and appears to occur without significant consumption of coagulation factors. 4 The authors suggested that acute traumatic coagulopathy is caused by tissue hypoperfusion resulting in the activation of the anticoagulant protein C pathway, not the consumption of coagulation factors. Hence, Brohi et al stated that management of acute traumatic coagulopathy should focus on limiting the degree and duration of shock and tissue hypoperfusion. 4 In patients with shock, the degree of acidosis reflects the grade of hypoperfusion. However, little is known about the influence of acidosis on the outcome in patients with ruptured AAA. Hence, further investigation of the acid–base status in relation to shock, mortality, and complications particularly hemorrhage due to coagulopathy in patients with ruptured AAA is justified.
The aim of the present study was to investigate the incidence of coagulopathy and acidosis preoperatively in patients with ruptured AAA in relation to the clinical outcome and with special regard to the influence of shock.
Materials and Methods
Patients
The study was performed in accordance with the principles of Declaration of Helsinki and subsequent amendment. All patients were of the same ethnic origin and had similar socioeconomic backgrounds. Patients with coexisting malignant disease, uremia, or a current thromboembolic disease were excluded. A total of 55 patients with ruptured infrarenal AAA were consecutively included. All patients had a retroperitoneal hematoma confirmed during operation and 43 had signs of clinical shock with at least 1 episode of hypotension (systolic pressure of <80 mm Hg) prior to aortic cross clamping. 5 Remaining 12 patients were not in clinical shock. A temporary initial aortic clamping at the supraceliac level is the standard approach at our department in patients operated for ruptured AAA. 6 No blood transfusions were given before laparotomy and, in accordance with Crawford, no significant attempt was made in blood volume resuscitation until surgery. 7 The transfusion policy in surgery included rapid administration of large numbers of red blood cell (RBC) units, along with sufficient fresh frozen plasma (FFP) and platelets to treat or prevent coagulopathy. Red blood cell and FFP units were given alternately until 10 units of each were transfused, followed by 1 unit of aphaeresis platelets in a massive transfusion situation. 8 Furthermore, coagulopathy was avoided by prevention of hypothermia and correction of acidosis. For comparison, 40 patients with an elective operation for nonruptured infrarenal AAA were included. The aortic size was confirmed in all patients by ultrasonography and the largest aortic diameter was recorded. All patients underwent conventional open AAA repair through a standard midline laparotomy incision and transperitoneal approach with infrarenal graft repair. The inhospital deaths, 30-day mortality, and complications were recorded.
Blood Sampling and Assays
Peripheral venous blood samples were taken from each patient preoperatively and before any blood products had been transfused.
Hematocrit (Hct), platelet count, activated partial thromboplastin time (aPTT), and prothrombin time (PT) transformed to the international normalized ratio (INR) were analyzed by routine clinical methods with intra-assay coefficient of variation (CV) <3.2% and interassay CV <3.6% in all assays. We use platelet count, aPTT, and PT as preoperative screening for the risk of bleeding. 9
Arterial blood samples were taken before any correction of acidosis at the start of operation. Arterial blood gas analysis was performed on an automated blood gas analyzer in a point-of-care testing laboratory using a radiometer (Copenhagen, Denmark) device. From the primary data, the base deficit (BD) was calculated. Coagulopathy was defined as PT (INR) ≥1.5 and acidosis was defined as BD ≥6 mmol/L in accordance with established practice. 10
Statistical Analysis
All analyses were carried out using SPSS statistical software 14.0 for Windows (SPSS, Chicago, Illinois). Data are presented as the median (interquartile range) or the number (percentage) of patients. Differences in findings between study groups were assessed by chi-square tests (2-tailed without Yates correction) for categorical variables and by Mann-Whitney tests for continuous variables. AP value <.05 was considered significant.
Results
There were no significant differences between patients with nonruptured and ruptured AAA according to age, gender, and current smoking habits (Table 1). As shown inTable 1 the diameter of the ruptured AAAs was larger than the nonruptured AAAs (P = .011). In patients with ruptured AAA, Hct and platelets were significantly lower than that in the nonruptured AAA group (Table 2). Furthermore, PT and BD were significantly higher in the group with rupture (Table 2). As expected there was a significant difference (P = .005) in BD between patients with (7.0 [3.8-10.1] mmol/L) and without (3.4 [1.0-6.3] mmol/L) shock due to ruptured AAA. In the patient group with ruptured AAA and shock 12 of 43 patients died, the main cause of death was multiple organ failure (n = 7), other causes were cardiac related (n = 3) and coagulopathy/hemorrhage with abdominal compartment requiring relaparotomy (n = 2). In the group with ruptured AAA there were no significant differences in age, gender, current smoking habits, AAA diameter, Hct, platelets, and aPTT between survivors (n = 43) and nonsurvivors (n = 12). As shown in Table 3, current data show that measurement of BD is a better mortality predictor than PT. Estimated total blood loss and transfusion in patients with ruptured AAA were shown in Table 3.
Age, Gender, Current Smoking Habits, and Abdominal Aortic Diameter in Patients With Nonruptured and Ruptured AAA a
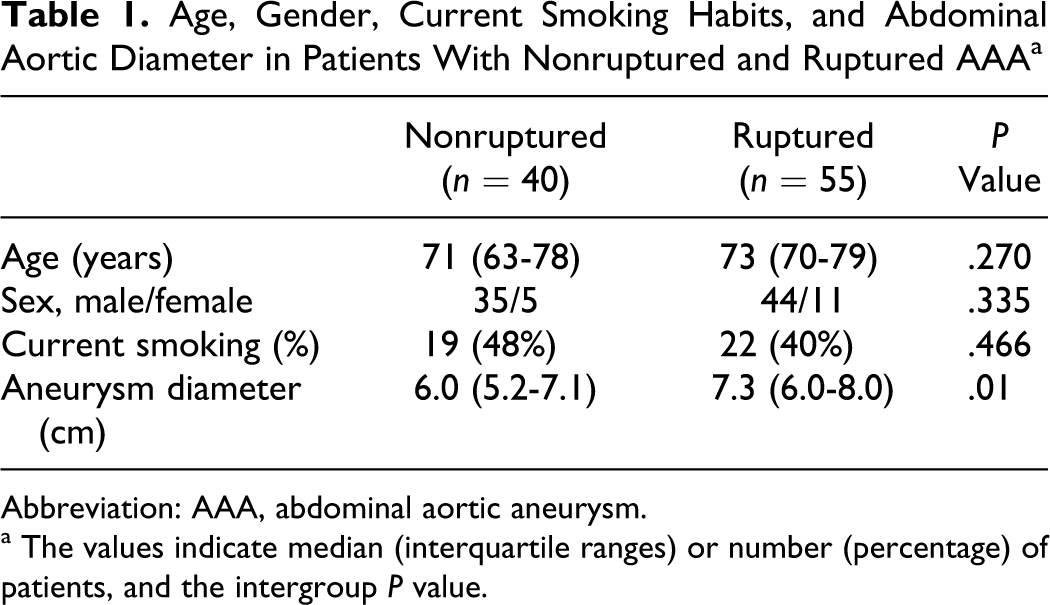
Abbreviation: AAA, abdominal aortic aneurysm.
a The values indicate median (interquartile ranges) or number (percentage) of patients, and the intergroupP value.
Laboratory Results in Patients With Nonruptured and Ruptured AAA a
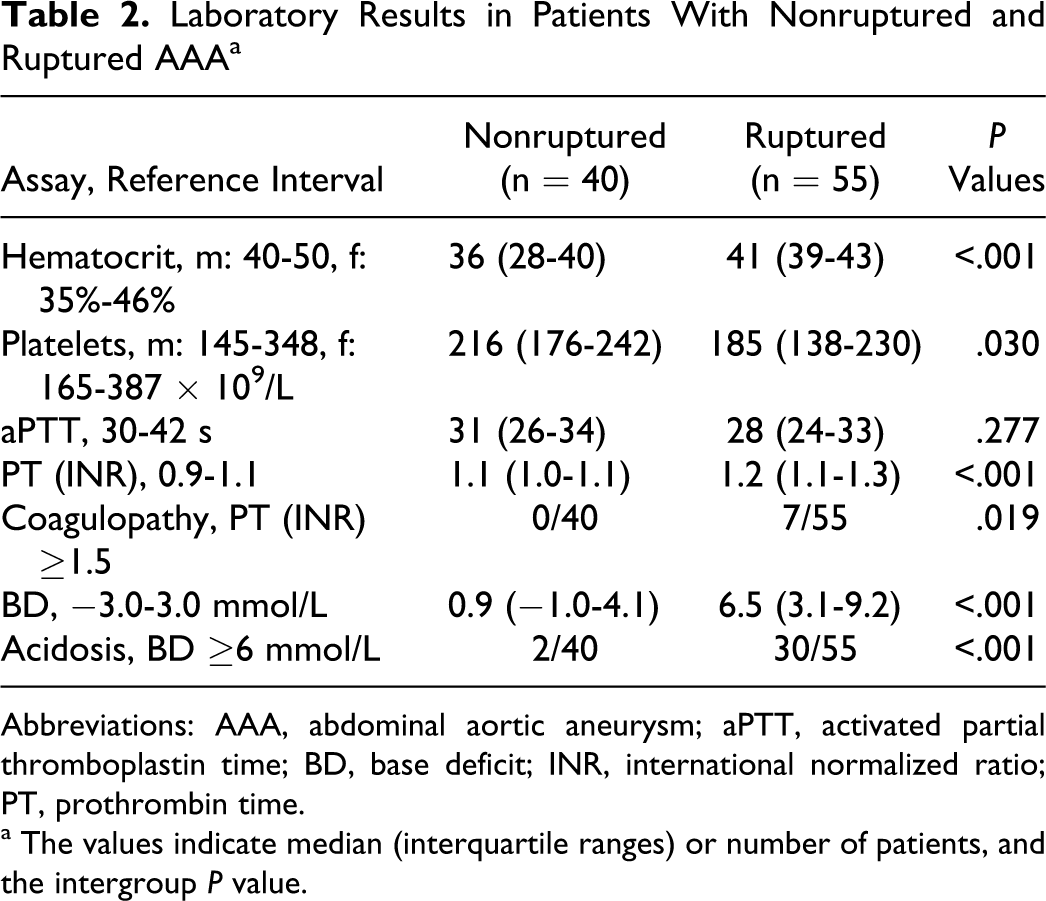
Abbreviations: AAA, abdominal aortic aneurysm; aPTT, activated partial thromboplastin time; BD, base deficit; INR, international normalized ratio; PT, prothrombin time.
a The values indicate median (interquartile ranges) or number of patients, and the intergroupP value.
Laboratory Results for the 2 Subgroups (Survivors and Nonsurvivors) of Ruptured AAA a
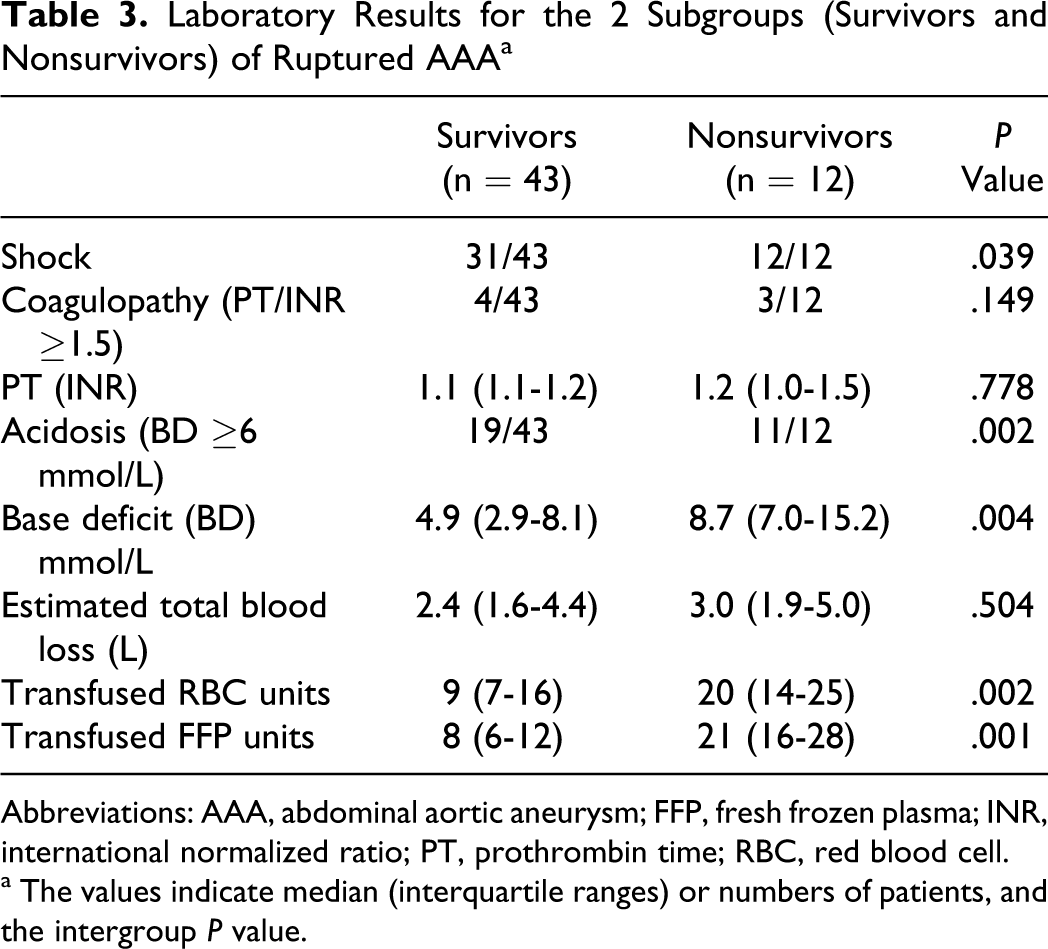
Abbreviations: AAA, abdominal aortic aneurysm; FFP, fresh frozen plasma; INR, international normalized ratio; PT, prothrombin time; RBC, red blood cell.
a The values indicate median (interquartile ranges) or numbers of patients, and the intergroupP value.
Discussion
Shock at admission is a well-known poor predictor in patients with ruptured AAA. Furthermore, in patients with shock the degree of acidosis reflects the grade of hypoperfusion. In the present study, clinical shock was defined as at least 1 episode of hypotension (systolic pressure of <80 mm Hg) prior to aortic cross clamping. We found acidosis in the start of surgery in 30 of 55 patients with ruptured AAA, which means that a majority of the so-called shock group was hemodynamically unstable and suffering the consequences of malperfusion. In fact, acidosis at admission was a better mortality predictor than shock at admission. Acidosis is, besides hypothermia and hemodilution, a possible cause of coagulopathy. 3 Coagulopathy is both a laboratory finding and a clinical condition associated with poor outcome. 2 Patients with hemorrhagic shock can go on to develop an acquired coagulopathy. However, the present data demonstrate a low frequency of preoperative coagulopathy (7 of 55) in patients with ruptured AAA. Furthermore, in our patients with ruptured AAA only 2 patients have fatal coagulopathy and bleeding. The main causes of death were multiple organ failure and cardiac failure. Adam et al have shown a procoagulant state in patients with ruptured AAA, which may contribute to microvascular and macrovascular thromboses that, in turn, lead to the common causes of perioperative morbidity and mortality, namely myocardial infarction, multiple organ failure, and thromboembolism. 11 Our results show a relatively high incidence of thrombosis-related causes of death in patients with ruptured AAA, indicating a relation to an activated coagulation in these patients.
The low overall mortality in patients with shock due to ruptured AAA in the present study was in agreement with the improvement in survival in a recent report. 12 The improvement in mortality has many causes. For instance, modern management of the patient with hemorrhage due to ruptured AAA included rapid administration of large numbers of RBC, along with sufficient plasma and platelets to treat or prevent coagulopathy. Furthermore, aggressive rewarming to prevent hypothermia by warm fluid infusion, forced air warming, and the use of warm water on the surgical field also prevent coagulopathy. Correction of acidosis also has a high priority during the initial evaluation.
There are some limitations to the present study. First, as was stated by Brohi et al coagulopathy is hard to measure. 4 Second, the overall low mortality in patients with shock due to ruptured AAA in the present study may indicate that the shock was not deep. However, more than half of the patients have acidosis which means that they suffered the consequences of malperfusion due to clinically important hypotension. Last, the estimated time in shock was not considered in the present study. Despite these limitations our results showed a low incidence of laboratory coagulopathy preoperatively. Indeed, fatal coagulopathy was relatively uncommon, instead there was a high incidence of thrombosis-related deaths in AAA patients with shock due to rupture.
In conclusion, our findings counteract with previous results and probably imply that modern emergency management of ruptured AAA has improved in the attempt to prevent fatal coagulopathy.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.